Critical Events During the Weight Acceptance Task
The two phases associated with weight acceptance, initial contact and loading response, coincide with the period of initial double support, and include four critical events. The first critical event, a heel-first initial contact, must be present if forward momentum is to be preserved (24) and the energy from the falling body COM is to be redirected in the direction of progression (32).
It is also necessary to prepare the new support limb for the demands of the next phase. The next three critical events of hip stability, controlled knee flexion for shock absorption, and controlled ankle plantar flexion, must occur during the loading response phase. Hip stability requires dynamic joint stiffness in the sagittal and frontal planes at the hip to prevent unnecessary forward pelvic tilt or increased pelvic obliquity, respectively. This places a high demand on the torque (moment) production ability of the hip extensors and hip abductors of the forward load-bearing limb. This demand is reflected in increased muscle activation (recorded using dynamic EMG) in the gluteus maximus, gluteus medius, and hamstrings. If a patient has weak hip extensors and fails to compensate for this weakness, there will be an increased anterior pelvic tilt and/or forward trunk lean directly associated with the inability of the hip extensors to meet the demand of this critical event. Alternatively, if the subject is successfully compensating for the weakness, they will exhibit a posterior trunk lean to position the whole body COM behind the hip joint center, thus reducing the torque production demand on the hip extensors. Evidence of either strategy is reflected in recordings of the hip sagittal plane angles (kinematics), the weight line (ground reaction force vector), dynamic EMG of the hip extensors, or by calculating the hip extensor moments and powers (kinetics). Similar strategies are used when there is weakness in the hip abductors, leading to either uncompensated or compensated Trendelenburg’s gait patterns in the frontal plane. All can be related to the loss of the critical event of hip stability during the loading response phase.Controlled knee flexion for shock absorption must occur to prevent unnecessary knee flexion during loading response, which wastes energy and places a higher demand on the quadriceps. Similar to the hip, quadriceps weakness can also be either compensated or uncompensated. Uncompensated quadriceps weakness will present as abnormal or increased knee joint angular displacements in the sagittal plane (increased knee flexion) with possible collapse at the knee. Compensated patterns will display body postures that shift the COM forward (forward trunk lean) so that the ground reaction force vector is closer to or in front of the knee joint, thereby reducing the quadriceps demand (quadriceps avoidance gait). Again, these patterns are reflected in kinematic, kinetic, and dynamic EMG measurements, within the context of meeting the needs of this critical event. Correctly controlled knee flexion during loading response is reflected in the slope and maximum knee flexion value during the first peak of the sagittal plane knee joint angular displacement curve, in the magnitude of the knee extensor moment and power absorption curve, and the EMG activity of different heads of the quadriceps.
The final critical event during loading response is controlled ankle plantar flexion. In this context, “controlled” is referring to the ability of the ankle dorsi- flexors to eccentrically contract and lower the initially neutral foot carefully to the ground to provide a more stable base of support than can be provided by the calcaneus alone. This action is referred to as the heel or first rocker (40), the first of three important mechanisms that occur at the foot and ankle and facilitate progression of the entire stance limb (31).
These three rockers are illustrated in Figure 16.13. If the pretibial muscles have sufficient strength to restrain the rate of foot drop, the action of the first rocker pulls the tibia forward, which in turn is transferred to the femur by the active quadriceps that is attempting to restrain the rate of knee flexion. This is how the energy of the falling body COM is redirected to provide forward progression, an important energy-conserving mechanism often lost when the heel rocker is absent. If the pretibial muscles did not have sufficient strength but the subject was able to achieve a heel-first initial contact, a noticeable foot-slap would occur as the unstable lever at the ankle allows the foot to plantar-flex uncontrollably. This is reflected in a steep descending initial slope on the sagittal plane ankle kinematic curve and absence of either a dorsiflexor moment or dorsiflexor power absorption on the corresponding sagittal plane kinetic curve (22). Experienced clinicians can also detect this event without all the modern conveniences by simply listening for the sound of the foot-slap! The effects of uncontrolled ankle plantar flexion at loading response are not as easy to detect when the subject fails to achieve a heel-first initial contact, as is the case with foot-flat, forefoot, or equinus initial contact. In this case, kinetic data are helpful, because as the point of foot/floor load bearing moves further in front of the ankle with progressively increasing plantar flexion at initial contact, there is a proportional increase in the magnitude of the incorrect plantar flexor moment during loading response. This plantar flexor moment (via the triceps surae) has opposite the desired effect on the knee, as occurs with eccentric contraction of the pretibial muscles when a true heel rocker is present; the knee extends when it should be flexing (41). This reduces the effectiveness of knee shock absorption and may eliminate it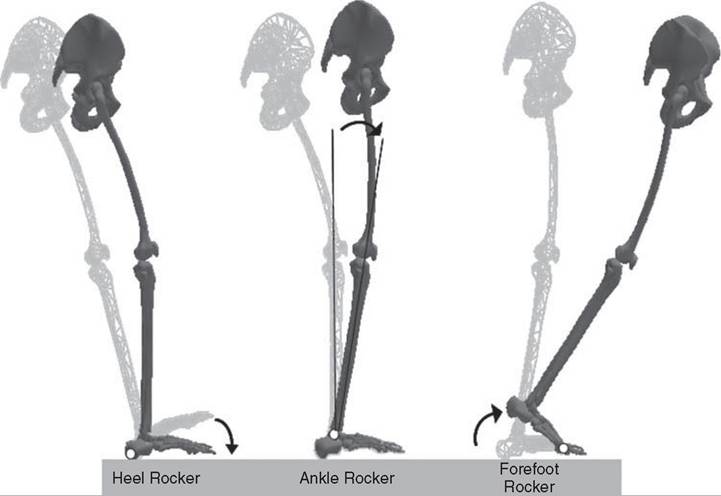
Figure 16.13 The three rockers representing normal ankle function in gait: These are the heel or first rocker, the ankle or second rocker, and the forefoot or third rocker.
The lighter gray skeleton represents the beginning of each rocker, and the arrows signify the movement that is associated with each. Refer to the text for a full description of these important critical events.completely, increasing bone-on-bone forces at the knee. The amount of shock-absorbing energy transferred to the hip and ankle is reflected in the hip, knee, and ankle powers during this phase, and is useful for describing the potential degree of impairment associated with incorrect ankle function at loading response. Note that the magnitude of the EMG activity of the pretibial and posterior compartment muscles by themselves do not explain the moments at the ankle, since major force contributors arise from the inertial and gravitational forces that occur during the first rocker. The EMG activity does help sort out if the pattern of motion is due to weakness (pretibial muscles with first rocker present, triceps surae without it), neglect (often seen in traumatic brain injury [TBI]), or poor motor control (seen in cerebral palsy or cerebrovascular accident [CVA]). This information can assist in determining whether a solid, leaf-spring, hinged, or floor-reaction AFO, Botox injections into the calf musculature, or tendon lengthening or transfer surgery would be the most appropriate intervention to use when the critical event of controlled ankle plantar flexion is abnormal or absent. Table 16.4 summarizes many of the gait measurements that are useful for identifying functional causes for absent or abnormal critical events during the weight acceptance task, and while not exhaustive, can help organize the array of measures available for assessing impairments during this task.