DENGUE
Dengue, the commonest Arthropod-borne (ARBO) viral illness, is a major public health problem in India with many outbreaks in recent years, usually in urban population.
Disease presents with many clinical variants-asymp- tomatic illness, classical dengue fever (DF), dengue hemorrhagic fever (DHF) and dengue shock-like syndrome (DSS).
Epidemiology: Dengue fever is caused by one or more of the four serotypes (DENV 1-4), though severe disease, e.g. DHF/DSS is more common with serotype 2.
An infected case is the usual reservoir of infection, which is mainly transmitted by a mosquito ‘ Aedes aegypti'. This mosquito has typical daytime biting habit and breeds on stored water in houses. Rain water collected on terrace junks, is a major cause of increased vector density and focal outbreaks in urban slums at the end of rainy season. As the vector cannot fly for long distance, movement of infected persons is the major cause of distant transmission in dengue fever.
Mosquito is infected after feeding on a patient in viremic stage (1-5 day after onset of illness) and becomes infective after an extrinsic incubation period of 8-10 days. Vector, once infected, remains infective for life.
Etiopathogenesis is complex and still evolving.
• First infection in previously unexposed person leads to transient viremia after an incubation period of 5-7 days, which is either asymptomatic or presents with nonspecific febrile illness or classical dengue fever. At the end of viremia, these patients develop—(a) homo-type neutralizing antibodies to provide life-long immunity against same serotype; and (b) heterotype nonneutralizing antibodies, which unfavourably alter the course of second infection with different serotype.
• Second infection with same serotype is asymptomatic but by different serotype may present with severe DHF/DSS due to pre-existing non-neutralizing antibodies, immune complex formation and intense inflammatory response.
Pathology of DHS/DSS is mediated by activation of complement system and release of many inflammatory mediators, like cytokines, leading to:
• Vasculopathy, i.e. increased permeability with extravascular shift of fluids, leading to shock and hemoconcentration,
• Coagulopathy, due to activation of clotting/fibrinolytic mechanisms with DIC-like bleeding manifestations, and
• Multi-organ dysfunction due to above changes.
Clinical spectrum of dengue spans from asymptomatic infection to severe life-threatening disease, and includes: Undifferentiated dengue fever, more common in younger children, presents as non-specific febrile illness, usually associated with—(a) generalized erythematous flush over body with suffused face (Fig. 10.12), and (b) absence of catarrh, despite nasopharyngeal and ocular congestion. Signs of bleeding or capillary leakage are absent.
Classic dengue fever usually presents as biphasic illness as follows:
• Febrile phase with—(a) sudden onset of continuous high fever, (b) severe headache, myalgia, arthralgia and retro-orbital pain, (c) generalized macular rash/ flush after 48-72 hours, usually sparing palms and soles, (d) disproportionate bradycardia, and (e) conjunctival congestion, rhinopharyngitis and nausea/vomiting. Fever usually comes down by lysis and profuse sweating after 3-5 days.
• Critical (leakage) phase begins after 3-5 days with development of increased capillary permeability and signs of plasma leakage from intravascular to extravascular compartment, e.g. hypotension, pleural

Fig. 10.12: Dengue: (A) Suffused or flushed face; (B) Macular rash.
effusion and rising hematocrit. Many warning signs during this phase (Table 10.38), may herald the onset of dengue hemorrhagic fever (DHF) and/or dengue shock syndrome (DSS), discussed later. This phase usually lasts for 36-48 hours.
• Convalescent (recovery) phase begins after 6-7 days of fever with clinical improvement due to control of capillary leakage and return of the leaked plasma back into intravascular compartment.
Patient may develop pulmonary edema due to fluid overload, if the overzealous fluid replacement continues.Dengue hemorrhagic fever or shock-like syndrome (DHF/DSS), is a serious, life-threatening manifestation, with first phase similar to classical dengue fever. However, these cases deteriorate rapidly on 2nd-5th day, with bleeding tendency, thrombocytopenia, evidence of plasma leakage with or without circulatory shock. Severity of DHF/DSS may be classified into four grades, according to two clinical hallmarks—bleeding and shock (Table 10.39). After 24-36 hours of crisis, recovery begins in adequately treated cases, though mortality is high (40-50%) in others.
Expanded dengue syndrome denotes multiple organ involvement in these cases, e.g. encephalopathy, hepatitis, renal failure, myocarditis or ARDS, more common in adults or those with co-morbidities.
National guidelines for clinical management of dengue fever (2023) classify dengue fever as asymptomatic and symptomatic, later further sub-classified as mild (without warning signs), moderate (with warning signs) or severe (with shock, bleeding or organ involvement) dengue based on various indicators (Fig. 10.13).
Diagnosis rests on clinical suspicion, with laboratory tests to confirm the presence of virus, antigen or antibodies. Timing of the tests is important, dependent on the course of disease. Commonly used diagnostic tests include:
• NS 1 antigen test: Non-structural protein (NS1) antigen is present in the serum during first 5-7 days of fever and its detection by an ELISA-based test helps in early diagnosis of dengue. However, the antigen disappears after 4-5 days and the test becomes negative. While rapid card tests for qualitative detection of NS1 using immunochromatography are also available, results are unreliable as compared to ELISA test, due to poor sensitivity.
• Anti-dengue IgM antibody test: These antibodies are detectable usually by day 5 of the illness and persist for ~ 60 days.
Detection of these antibodies by ELISA or rapid tests help in diagnosis of disease after 5 days. However, rapid tests are not recommended due to high rate of false-negativity.• Polymerase chain reaction (PCR): Molecular diagnosis based on detection of viral nucleic acid by RT-PCR is confirmatory in acute phase but the test may be negative after first week of illness.
Viral isolation or IgG antibody tests are of limited value in the diagnosis of acute disease.
Supporting investigations include hematocrit, platelet count and relevant tests for organ dysfunction, which need to be repeated frequently to monitor the progression of disease. Hematocrit and platelet count should be monitored at least every 24 hours for early detection of warning signs, i.e. hemoconcentration (due to capillary leak) and thrombocytopenia, though more frequently in severe dengue.
Table 10.40 presents current WHO/NVBDCP case definitions for dengue fever and related conditions.
TABLE 10.38: Warning symptoms and signs in dengue fever
• Persistent vomiting
• Abdominal pain or tenderness
• Lethargy, restlessness or irritability
• Hepatomegaly (gt;2 cm)
• Clinical fluid accumulation (ascites, pleural effusion)
• Bleeding manifestations, usually mucosal bleeds
• Rising hematocrit with concurrent drop in platelet count
TABLE 10.39: Severity grading of DHF/DSS
I Dengue fever + positive tourniquet test and evidence of plasma leakage
II As above + spontaneous bleeding and abdominal pain
III As above + evidence of circulatory failure
IV Profound shock with undetectable BP/pulse
Plus Thrombocytopenia lt;100000 cells/mm3, and more than 20% rise in hematocrit.
D/D of dengue includes other causes of viral and non- viral hemorrhagic fevers (Ch. 10.1.14). Dengue-like illnesses have also been reported in India from other arboviruses, e.g. chikungunya virus and West Nile virus. Management is essentially symptomatic and supportive, depending on the severity of disease, as follows:
DF without warning signs need not be hospitalized and may be managed at home with bed rest, antipyretics, adequate oral hydration and monitoring for the warning signs.
NSAIDs, e.g. aspirin or Ibuprofen should be avoided due to risk of gastritis, platelet dysfunction and bleeding. ORS or fruit juices are preferable to plain water for rehydration to replenish fluid and electrolyte losses due to excessive sweating or vomiting. However, parents should be counselled about the need to observe for warning signs, which require urgent medical attention. DF with warning signs: Immediate hospitalization is recommended to all cases with warning signs for close
Fig. 10.13: Clinical case classification of Dengue: National Guidelines 2023.
TABLE 10.40: Case definitions for dengue fever/DHS/DSS
Probable dengue fever (any one of following)
• Acute febrile Illness (2-7 days) with (any 2 of following) Headache, retro-orbital pain, rash, myalgia, arthalgia, bleeding, thrombocytopenia or leucopenia, warning signs or symptoms
• Positive NS1/IgM test (non-ELISA based)
Confirmed dengue fever (Clinically compatible, with any one of following)
• Positive NS1 test by ELISA
• Positive anti-dengue IgM antibodies by ELISA
• Positive dengue PCR test
• Viral isolation from serum, plasma or leukocytes
• gt;4 fold rise in IgG antibodies after 2 weeks
Dengue hemorrhagic fever* (all four of following)
a. Clinical criteria for dengue fever, as above
b. Hemorrhagic tendency (any one of following)
- Positive touniquet test
- Petechiae, ecchymoses or purpura
- Bleeding from mucosa, GIT, injection or other sites
c. Thrombocytopenia (lt;100,000 cells/mm3)
d. Evidence of plasma leakage (any one)
- Rise in hematocrit gt;20% over baseline for age/sex
- Drop in hematocrit gt;20% after volume replacement
- Signs, e.g. pleural effusion, ascites, hypoproteinemia Dengue shock syndrome* (both of the following)
a. All of the above criteria for DHF with
b. Circulatory failure: Rapid/weak pulse, pulse pressure lt;20 mm Hg, hypotension, cold-clammy skin, restlessness
*As per National guidelines 2014; (DHS/DSS are not defined in Guidelines 2023).
monitoring with serial hematocrit and platelet count daily, till the patient is afebrile for 1-2 days. Cases with persistent vomiting may need parental fluids and electrolyte therapy.Admission criteria in dengue include presence of: (a) warning signs, (b) significant bleeding, (c) persistent high fever, (d) sudden drop in body temperature, (e) rapid fall in platelet counts, (f) hypotension, and (g) organ dysfunction, e.g. renal, hepatic or CNS involvement.
Hemoconcentration due to plasma leakage from intravascular compartment is the major concern in these cases. These patients require closely monitored intravenous fluid therapy with crystalloid fluids along with supportive measures. Fig. 10.14 presents an algorithm for fluid replacement in these cases, as per national guidelines.
Severe Dengue with Shock: These cases essentially need intensive care with close monitoring for vital signs, hematocrit and bleeding. Fluid therapy may be supplemented by colloids and if necessary, whole blood transfusions in selected cases. Fig. 10.15 presents an algorithm for fluid replacement in these cases, as per national guidelines.
Fluid replacement therapy: Some general principles of fluid replacement therapy as follows:

Fig. 10.14: Fluid management in moderate Dengue with warning signs.
Improvement: Hct falls, HR and BP stable, urine output rises. No Improvement: Hct and HR rises, pulse pressure fall lt; 20 mm Hg, urine output falls
*Whole blood 10 ml/kg or packed cells 5 ml/kg.
IVF: IV fluids; Hct: Hematocrit
• Volume of fluid therapy should be calculated on the basis of body weight with 5% deficit, revised every 1-3 hours.
• First-hour fluid therapy should begin with 6 ml/kg in moderate dengue without shock and 10-20 ml/kg in severe cases with compensated shock, while those with decompensated shock must be infused 10-20 ml/kg over 15-30 minutes.
• Ringer lactate, normal saline or DNS 5% are preferred fluids for this purpose.
• Hematocrit, vital signs, e.g. heart rate and blood pressure, and urine output must be monitored along with indicators of fluid overload, e.g. hepatomegaly or breathlessness due to pulmonary edema. Central venous pressure (CVP) monitoring is advised in unstable cases, if possible.
• In cases showing improvement with falling hematocrit and stable vitals, infusion rate must be reduced gradually after every 2-4 hours. IV fluid may be discontinued after 24-48 hours.
• In cases with no improvement or deterioration, further treatment must be decided on the basis of hematocrit:
- In cases with rising hematocrit suggestive of continuous plasma leak, infusion rate must be increased or maintained at 10-20 ml/kg/hr. Colloids, e.g. dextran-40, may be used in these cases.
- In cases with falling hematocrit, suggestive of bleeding, blood transfusion with whole blood (10 ml/kg) or preferably packed cells (5 ml/kg) is indicated.
• Further management of non-improving cases also includes IV inotropes and cardio-respiratory support, as required.
Management of bleeding: Cases with severe bleeding are best managed with whole blood transfusion, till the specific cause is identifiable, e.g. severe thrombocytopenia or coagulopathy due to hepatic dysfunction. Platelet transfusions are recommended only in cases with: (a) platelet count lt;10,000#8725;mm3 and/or (b) severe clinical bleeding. Packed cell transfusions or fresh frozen plasma may be needed in some cases.
Management of organ dysfunction: Hepatitis, myocarditis and acute kidney injury is common in dengue and need to be managed intensively. Fluid therapy must be closely monitored in cases with renal dysfunction due to potential risk of pulmonary edema. Comorbidities, e.g. malaria, tuberculosis may sometimes complicate these cases and must be considered in non-responding cases.
Antiviral agents, steroids and immunoglobulins have no role in management of dengue.
Criteria for discharge in a dengue case include: (a) absence of fever gt;24 hours without antipyretics, (b) Stable vital signs for gt;2-3 days, (c) platelet count gt; 50,000 cells/mm3, and (d) visible clinical improvement with no respiratory distress and good urine output.
Prevention and control of outbreaks depends on:
• Vector-control measures, e.g. avoidance of breeding sites, e.g. prolonged indoor water-storage and use of larvicides, insecticides.
• Personal protection measures, e.g. repellents, nets and avoidance of travel to outbreak area.
Currently no dengue vaccine is available in India. CYD-TDV (Dengvaxia®) is the first and only licensed vaccine against dengue, being used in some endemic countries of Asia and Latin America, though several other candidates (including one indigenous vaccine by Serum Institute of India, Pune) are under development. (Ch 9.2.4).
Other important arboviral illnesses are as follows: Chikungunya is a benign, dengue-like syndrome, characterized by sudden onset of fever, arthralgia, maculopapular rash and leukopenia. Recent years have witnessed intermittent outbreak of this disease in many parts of India.
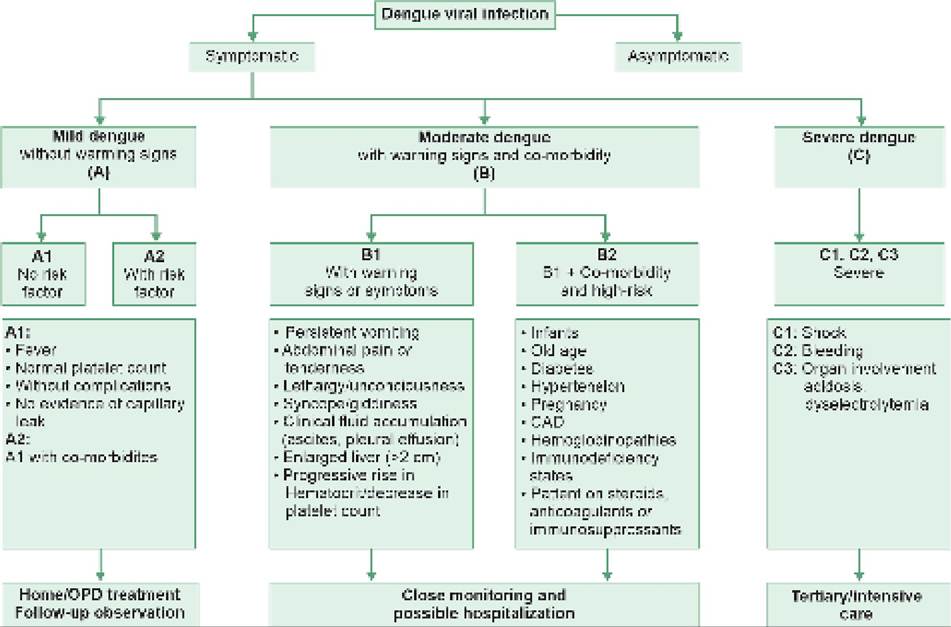
Fig. 10.15: Fluid management in severe Dengue with compensated or decompensated shock.
Improvement: Hct falls, HR and BP stable, urine output rises
No Improvement: Hct and HR rises, pulse pressure fall lt; 20 mm Hg, urine output falls *Whole blood 10 ml/kg or packed cells 5 ml/kg.
IVF: IV Fluids; Hct: Hematocrit
Epidemiology: Chikungunya is a zoonotic RNA virus, widely distributed in many vertebrate species with asymptomatic or symptomatic infections. Humans are infected via mosquito bite, with Aedes aegypti being the commonest vector in India. Though subclinical infections are common, chikungunya outbreaks generally indicate substantial rise in susceptible human and A. aegypti population above a threshold level.
Clinical presentation: After an incubation period of 2-4 days, the infection generally follows a different course in different age-groups:
• In infants, clinical illness begins with sudden onset of high fever, flushed skin, conjunctival congestion and pharyngitis, followed by a generalized maculopapular rash and lymphadenopathy after 3-5 days. However, arthralgia-the hallmark of disease in older population, is rare in this age group. Unlike other viral infections, Enanthems are absent.
• In older children, acute onset fever is typically associated with severe headache, arthralgia and myalgia; followed by maculopapular rash and lymphadenopathy after 3-5 days, just before the defervescence. Febrile convulsions are common. Rash, arthralgia and lymphadenopathy disappears in next 2-3 days. Residual arthralgia beyond first week is uncommon in children.
• In adolescents/adults, severe fleeting polyarthritis/ arthralgia, is the hallmark of disease. Typically, the pain shifts from joints to joints, more prominent in morning and worsens with movements. Swellings of ankle, wrist and fingers is common. Arthralgia may persist for many weeks, often confused with rheumatoid arthritis.
Diagnosis depends on: (a) history of on-going outbreak,
(b) clinical suspicion, and (c) serological studies with IgM ELISA after at least a week of complaints. Viral isolation is possible though rarely feasible.
D/D includes other causes of dengue-like illnesses. Important differences with dengue include: (a) shorter duration of fever, generally lt;72 hours, (b) more pronounced arthralgia, terminal rash and conjunctival congestion, and (c) rarity of shock and hemorrhagic manifestations.
Treatment is largely supportive, including bed rest, NSAIDs to control pain and inflammation in cases with arthralgia, nutritional support and correction of fluid and electrolyte balance, if necessary.
Despite acute explosive onset with dengue-like illness, complications, e.g. shock and bleeding are extremely rare and mortality is almost unknown. Though older children/adolescents may continue to experience intermittent arthralgia for many months, complete recovery is the rule except a few reports of destructive arthropathy. Prevention mainly includes mosquito control and bite prevention strategies. No vaccine is available, though a formalin inactivated and a live attenuated vaccine is in experimental stage.
Kyasanur forest disease is currently prevalent in Mysore region (Karnataka), transmitted by ticks. Monkeys or forest-rodents act as amplifying reservoirs of infection apart from human host. It mainly occurs in adults, exposed during forest-visits and presents with high fever, severe myalgia, prostration, pneumonia and bleeding. Renal/hepatic failure and meningoencephalitis may develop after a latent phase in some cases (biphasic illness). Diagnosis rests on serology and treatment is supportive.
10.24
More on the topic DENGUE:
- Dengue
- ACUTE KIDNEY INJURY
- HEMORRHAGIC FEVERS (Fever with Petechiae/Purpura)
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Macrovascular Complications of Diabetes Mellitus