DIAGNOSTIC APPROACH IN CHD
Presence of a murmur, by itself, does not necessarily indicate heart disease in children, as ~15-20% infants have functional murmurs due to relatively high blood volume, hyperdynamic blood flow and smaller size of valves.
Diagnostic approach towards a child or infant with murmur revolves around following questions:
a. Whether a heart disease is present?
b. If yes, whether it is congenital or rheumatic?
c. If congenital, whether it is acyanotic or cyanotic?
d. Whether it is associated with increased PBF or decreased/normal PBF?
e. Whether it is associated with RVH or LVH?
f. Whether any complications, e.g. CCF, infective endocarditis or arrhythmia are present?
TABLE 17.23: D/D between LVH and RVH
Step I. Whether a heart disease is present?
Nadas criteria (Table 17.21) is very useful to answer this question in young children. Presence of any one major or two minor criteria strongly indicate presence of organic heart disease. Functional murmurs are common in infancy as well as in older children with hyperdynamic flow, i.e. severe anemia, thyrotoxicosis, beriberi, and large A-V fistula.
Step II. Whether it is congenital or rheumatic HD?
Important differences between CHD and RHD are shown in Table 17.22, most important being the age of presentation. While ~75% of CHDs manifest by the end of infancy, RHDs are extremely rare before 5 years. However, ASDs, small VSDs and mild congenital valvular lesions, e.g. MR, PS, AS or mitral valve prolapse may be easily missed in early life.
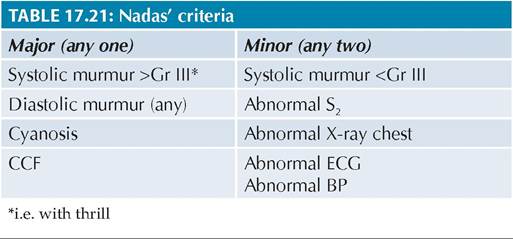
Fig.
17.19: Diagnostic algorithm for CHDs.LVH/RVH/BVH: Left/Right/Bi-ventricular hypertrophy; PBF: Pulmonary blood flow; VSD: Ventricular septal defect; PDA: Patent ductus arteriosus; ASD: Atrial septal defect; PS: Pulmonary stenosis; TGA: Transposition of great arteries; TrA: Truncus arteriosus; TAPVC: Total anomalous pulmonary venous drainage; SV: Single ventricle; DORV: Double outlet right ventricle; LHHS: Left hypoplastic heart syndrome; TA: Tricuspid atresia; PA: Pulmonary atresia; RHH: Right hypoplastic heart syndrome.
Step III. Whether it is acyanotic or cyanotic?
Presence of cyanosis differentiates Rt gt; Lt shunts from Lt gt; Rt shunts or simple obstructive lesions. However, it is important to note that:
• Cyanosis is often absent at birth in Rt gt; Lt shunts due to high pulmonary arterial pressure in relatively unexpanded lungs and appear after variable duration, depending on the severity of shunt and pressure gradients. Thus, absence of cyanosis at birth does not exclude cyanotic CHDs.
• Mild duskiness may develop in severe Lt gt; Rt shunts or obstructive lesions during excessive crying or heavy exercise due to compromised pulmonary blood flow. However, unlike cyanotic CHDs, it is easily relieved on rest or oxygen therapy (Hyperoxia test, see Chapter 17.2).
• Presence of clubbing, cyanotic spells, squatting posture and failure to thrive (without CCF) strongly indicates cyanotic CHD.
Step IV. Whether pulmonary blood flow is increased, decreased or normal?
• Increased pulmonary blood flow is indicated by—(a) recurrent chest infections, (b) breastfeeding difficulties (suck-rest-suck cycle), (c) plethoric lung fields on chest X-ray, and (d) Loud P2.
• Absence of these features or absent P2 indicates normal/decreased pulmonary blood flow.
Presence of cyanosis or dyspnea alone, is not a reliable indicators of pulmonary blood flow.
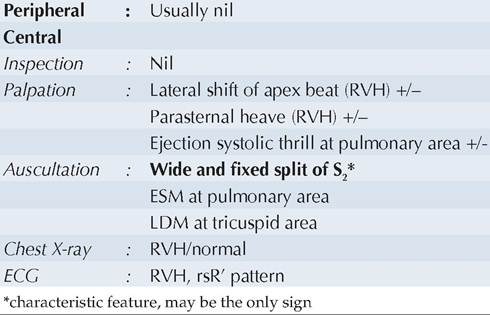
Step V. Whether it is with RVH or LVH?
Important diagnostic differences between RVH and LVH are shown in Table 17.23.
Step VI. Whether complications, e.g. CCF, infective endocarditis or arrhythmia are present?
Clinical features of these complicating events have been discussed in respective chapters.
A diagnostic algorithm for common CHDs, based on above observations is presented in Fig. 17.19.
17.6