DIAGNOSTIC ASSESSMENT
Assessment of a child with undernutrition involves: (I) assessment of dietary intake, (II) assessment of nutritional status, (III) classification of severity, and (IV) identification of complications.
I. Assessment of dietary intake is the first step in screening for undernutrtion, already discussed in chapter on nutritional assessment (Ch 5.9). It includes history of age- related infant and young child feeding (IYCF) practices, e.g. breastfeeding and complementary feeding as well as assessment of the actual dietary intake before the onset of presenting illness, usually by dietary recall method.
II. Assessment of nutritional status on the basis of anthropometric, clinical and biochemical parameters, as follows:
• Anthropometric parameters may be broadly divided into: (i) age-dependent parameters or (ii) ageindependent parameters.
Age-dependent parameters, e.g. weight and height are two most commonly used anthropometric indicators of undernutrition. Weight is the first anthropometric parameter to decrease in undernutrition and hence, considered as an indicator of acute malnutrition. Height is affected only after many months of undernutrition and hence, considered as indicator of the chronic undernutrition.
Age-independent parameters are useful when the exact chronological age of child is in doubt and are derived by comparing the relationship between two age-related parameters-one early indicator, e.g. weight and other late indicator, e.g. height. Weight for height is the most commonly used age-independent anthropometric parameter in assessment of undernutrition. However, it may be misleading in chronic cases due to proportionate fall in weight as well as height. Other rarely used age-independent indicators include: mid upper arm circumference or MUAC (for children aged 1-5 years only), Kanawati Index (MUAC/head circumference) and skin fold thickness.
Screening parameters are simple, inexpensive tools for mass nutritional surveillance of preschool children including Shakir's tape or Bangle test (Ch 5.9).
• Clinical diagnosis depends on the features discussed earlier in Ch 6.1.2, though with following caveats:
Edema shall be considered as a clinical sign of undernutrition only if it is bilateral and has no other known etiology, e.g. nephrotic syndrome.
Wasting as an indicator of growth failure is a subjective sign and should be used only if anthropometric parameters are no available or feasible. It may be masked in children with edema (kwashiorkor) or may be more marked in those with associated severe dehydration.
• Biochemical parameters are rarely used in clinical practice, mainly useful to detect early sub-clinical cases of undernutrition. Earliest biochemical change in undernutrition is the decrease in essential amino acid (EAA) levels—which cannot be synthesized endogenously, leading to altered EAA/ non-EAA ratio in plasma. Subsequently, plasma albumin levels fall, though the edema appears only when plasma albumin levels drop lt; 2.5 gm/dl.
III. Classification of severity: Various classifications systems were in vogue earlier, to denote severity and duration of PEM, as follows:
Weightfor age (WFA) based classifications, are simple and commonly used in practice, though do not indicate the duration of malnutrition and include Indian Academy of Pediatrics classification (Table 6.2), Gomez classification, Jellife's classification, etc.
Height/length-for-age (HFA) based classifications are rarely used in practice and included Waterloo's classification or McLaren's classification, etc.
TABLE 6.3: Welcome-trust classification
| Weight for age* | Edema | Type of PEM |
| 80-60% | Absent | Undernutrition |
| Present | Kwashiorkor | |
| lt;60% | Absent | Marasmus |
| Present | Marasmic kwashiorkor |
*As compared to 50th percentile of normal
| TABLE 6.2: Indian Academy of Pediatrics (IAP) classification | |
| Weight for age* | Nutritional status* |
| gt;80% | Normal |
| 71%-80% | Grade I PEM |
| 61%-80% | Grade II PEM |
| 51%-60% | Grade III PEM |
| lt;50% | Grade IV PEM |
*As compared to 50th percentile of normal
*or SD score
• Composite classifications, based on anthropometric as well as clinical criteria, are most informative and include Welcome-trust classification (Table 6.3), Waterlow's classification, WHO classification, IMNCI classification, etc.
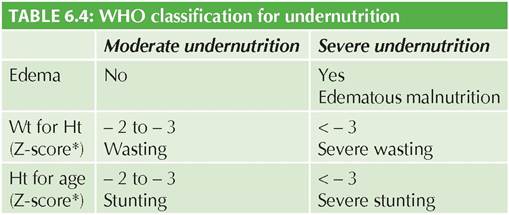
WHO classification, most widely used classification for epidemiological purpose rests on two anthropometric parameters: (a) weight for height (WFH) as a measure of acute malnutrition, and (b) height for age (HFA) as a measure of chronic malnutrition, along with one clinical parameter, i.e.
presence of symmetrical edema. It classifies all undernourished children in two major categories - moderate malnutrition and severe malnutrition, with each category further sub-divided as wasted and stunted (if WFH and HFA is between 2-3 SD respectively) or severely wasted or severely stunted (if WFA and HFA are lt; 3SD respectively). All cases with edema are considered as having severe malnutrition (Table 6.4).IMNCI classify nutritional status in children from 2 months to 5 years of age as: (a) severe acute malnutrition with complications, (b) severe acute malnutrition without complications, (c) moderate acute malnutrition, and (d) no acute malnutrition (Table 6.5).
IV. Assessment of complications: Malnutrition is rarely a primary cause of hospital visit, often presenting with complications (Table 6.6) with significant impact on the morbidity and mortality. Identification of these complications is also important to decide the need of hospitalization and strategies of management.
V. Investigations: Although PEM is a clinical diagnosis, following investigations are required on admission (initial assessment), to exclude or identify complications. • Complete hemogram including peripheral smear for anemia and infections (malaria).
TABLE 6.5: IMNCI classification for malnutrition
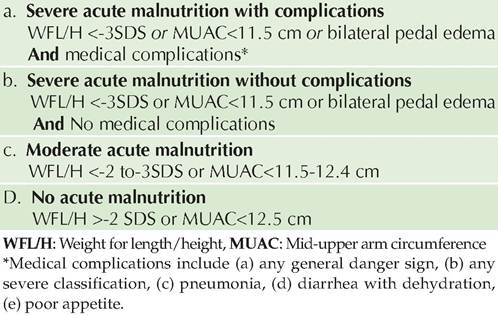
TABLE 6.6: Complications of PEM
Early (presenting) complications
a. Infections
Common : ARI, diarrhea, TB, helminthiasis
Severe : Gram -ve sepsis, septic shock, DIC
Opportunistic : Candidiasis
b. Hypothermia
c. Metabolic
Hypoglycemia
Hypocalcaemia
Hypomagnesemia
d. Fluid and electrolyte imbalance
Dehydration
Hypokalemia
Hypernatremia
e. Lactose intolerance
f. Severe anemia and other nutrient deficiencies
g. Congestive cardiac failure
Late (recovery) complications
a. Diarrhea (lactose intolerance)
b. CCF (high protein and solute diet)
c. Unmasking of subclinical vitamin/mineral deficiencies
d. Recovery syndromes (see text)
Long-term effects
a. Growth retardation
b. Cognitive and learning disabilities
• Urine examination, specially for pus cells (UTI),
• Stool examination, specially for fat globules (mal- absorption),reducing sugars (lactose intolerance) and microscopic ova/cysts,
• Chest skiagram for tuberculosis, respiratory infections,
• Tuberculin test, which may be false negative in severe PEM due to impaired cell mediated immunity.
• Biochemical tests, specially: S. albumin (hypoproteinemia) blood sugar (hypoglycemia) S. electrolytes (Na+, K+, Ca++ and Mg++) and liver/renal function tests,
• Microbial cultures (blood, urine, others),
• Other relevant investigations.
6.1.4