CLINICAL SPECTRUM
Clinical spectrum of undernutrition is a continuum, ranging from borderline growth delay to well-defined syndromes of marasmus or kwashiorkor. Within this spectrum, many other terms are also used to denote clinical variations, e.g.
pre-kwashiorkor, marasmic kwashiorkor, nutritional dwarfism, etc.Kwashiorkor, a term coined by Prof. Cicely Williams, denotes acute PEM due to either sudden nutritional deprivation, e.g. abrupt cessation of breastfeeding
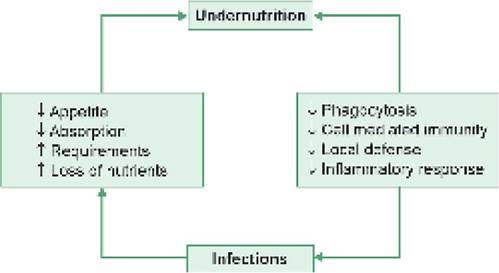
Fig. 6.1: Undernutrition and infection interaction.
(deposed child) or sudden increase in nutritional requirements due to infection, diarrhea, etc. Moderate weight loss (61-80%), edema and mental changes are three cardinal features of kwashiorkor, usually but not invariably, associated with hepatomegaly, skin/hair changes, vitamin deficiencies, etc.
Marasmus, a term derived from Greek word marasmos (wasting), is a state of chronic and severe undernutrition due to gradual nutritional deprivation, e.g. delayed complementary feeding with widening gap between nutritional requirements and breast milk output. Severe weight loss (lt;60%), wasting of muscles and subcutaneous tissue and absence of edema are hallmark of marasmus.
Some important clinical features of undernutrition with differences between kwashiorkor and marasmus are as follows (Table 6.1):
• Growth failure: Wasting is the essential feature in all malnourished children with/without stunting, more obvious in marasmus due to absence of edema. A marasmic child has typical shriveled (monkey like) look with gross emaciation, relatively larger head, staring eyes, prominent ribs, wrinkled skin and loose skin-folds over buttocks, inner thighs, axilla and chest. Buccal pad of fat is usually preserved except in severe marasmus (Fig. 6.2).
Bone age and dentition may also be marginally delayed.• Edema is the sine qua non of kwashiorkor, due to hypoproteinemia and consequent fluid retention (Fig. 6.3), though severity may vary from mild pitting edema over dependent parts, e.g. legs or sacrum, to generalized anasarca (Fig. 6.4). Severe edema may mask underlying wasting, weight loss and dehydration.
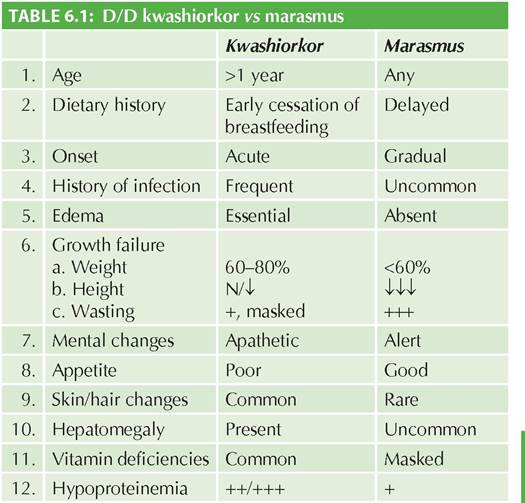
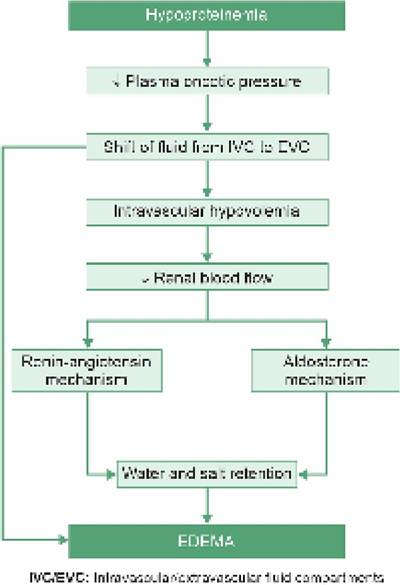
Fig. 6.3: Pathogenesis of edema in kwashiorkor.

Fig. 6.2: Clinical appearance of PEM (Marasmus).

Fig. 6.4: Clinical appearance of PEM (Kwashiorkor).
Mental changes: Children are typically apathetic and lethargic in kwashiorkor with little interest in surroundings, probably due to impaired activity of CNS enzymes in an un-adapted child. Anorexia is also marked in these cases. In contrast, marasmic children have good appetite and are usually alert with roving eyes as if searching for food.
Skin changes are more pronounced in kwashiorkor than marasmus due to combined effect of: edema, multiple vitamin deficiencies, essential fatty acid

Fig. 6.5: (A) Crazy pavement dermatosis,
(B) Flaky-paint dermatosis.
deficiency and secondary infections. Depending on the severity, these changes include: (a) phrynoderma, i.e. generalized dryness of skin, (b) diffuse or patchy areas of hypo/hyper pigmentation, (c) thin, shiny, taut skin over edematous areas, (d) moist ulcerations over flexural areas or pressure points, (e) superadded infections, e.g. pyoderma and scabies. Following lesions are classical but uncommon except in severe kwashiorkor (Fig.
6.5A and B):± Flaky paint dermatosis, i.e. hyperpigmented and desquamating area (flakes) over raw-skin;
± Crazy pavement dermatosis, i.e. hyperkeratotic, fissured skin with alternate areas of hypo-or hyperpigmentation;
± Mosaic dermatosis with mixed lesions in mosaic form.
• Hair changes are more common in kwashiorkor with thin, dry, sparse, lusterless, hypopigmented and
easily pluckable hair. Due to intermittent periods of better nutrition, alternate bands of hypo-and normal pigmentation on hair are classically described as flag sign. In marasmus, hair are sparse and hypopigmented.
• Hepatomegaly is common in kwashiorkor due to fatty infiltration of liver, though jaundice is rare and indicates poor prognosis.
• Concomitant nutritional deficiencies like xerophthalmia, vitamin B complex deficiencies, scurvy and anemia are more obvious in kwashiorkor. Although biochemical vitamin/mineral deficiencies are common in marasmus as well, clinical signs are less prominent in them due to adaptive mechanisms and usually appear in recovery phase.
Anemia in PEM is usually dimorphic, due to: (a) reduced dietary intake of hemopoietic factors like iron, proteins and folic acid, (b) co-existing infections affecting erythropoiesis, and (c) occult blood losses due to worm infestations.
• Concomitant infections like intermittent episodes of diarrhea, respiratory infections and skin infections are common in PEM, due to impaired immune mechanisms (Fig. 6.1) and mucosal integrity. Cellular immunity and phagocytic functions are predominantly affected in PEM, while immunoglobulin levels are usually normal or high with good antibody response.
Presence of infections may be clinically masked in undernutrition due to poor inflammatory responses, e.g. fever and leukocytosis. Hypothermia is an important indicator of infection in these children. Diarrhea in PEM may also result from malabsorption due to intestinal villous atrophy and consequent lactase deficiency, as well as due to hepatic/ pancreatic dysfunction.
6.1.3
More on the topic CLINICAL SPECTRUM:
- CLINICAL SPECTRUM
- ANORECTAL MALFORMATIONS
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- NEURAL TUBE DEFECTS
- CLINICAL EVALUATION OF GIT DISEASE
- COMPLEMENTARY AND ALTERNATIVE MEDICINE ^225 ^588 ^647
- 33 Intimate Partner and Sexual Violence
- Chapter 36 Sexual Assault and Domestic Violence
- REFERENCES
- Chapter 33 Disorders of the Breast