EPIDEMIOLOGY AND RISK FACTORS
CP is the most common motor disability of childhood, affecting approximately 3.6 per 1,000 school-age children (2) with at least 8,000 new cases each year in the United States (3).
The population of children with CP may be increasing due to premature infants who are surviving in greater numbers (4), higher incidence in normal-weight term infants (3), and longer survival overall. The proportion of CP that is most severe is also increasing, with as much as a third of all children with CP having both severe motor impairments and mental retardation (5).The etiology of CP is often not well understood. The majority of cases in term infants do not have an identifiable etiology (6). Factors that may contribute to brain injury and CP include prematurity, infection, inflammation, and coagulopathy (7). There is also considerable interest in the contributory roles of various biomolecules and cytokines that accompany infectious or inflammatory processes (8).
The greatest risk factor for the development of CP is prematurity. Premature infants (born earlier than 37 weeks gestation) are much more likely to develop the condition than term infants, and incidence rates are highest in the very earliest infants (9,10). Rates of CP in premature and low birth-weight infants vary from 40 to 150 per 1,000 live births (11), with some reports suggesting increasing (4) or decreasing rates (11,12) in the last decade or more. Figure 8.1 (5) demonstrates the role of prematurity in CP. The vertical bars represent raw numbers of children with CP and demonstrate that the largest numbers of children with CP were born at term. The horizontal lines represent the rates of development of CP at roughly 2/1,000 live births for term infants, 5/1,000 for infants born at 33-36 weeks gestation, and 30/1,000 live births for infants born prior to 28 weeks gestation. These rates demonstrate the profound effect of prematurity as a risk factor for CP.
Prenatal risk factors for CP include being small for gestational age (13), being of low or very low birth weight (14), developing infection (especially chorioam- nionitis and cytomegalovirus) (15), having evidence of stroke (16), or having neonatal encephalopathy (17).
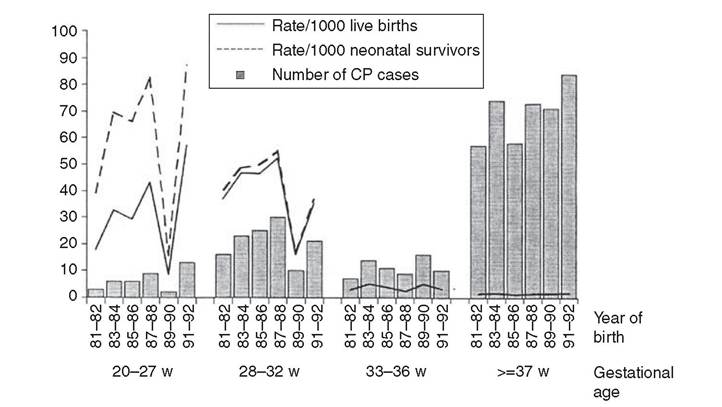
Figure 8.1 Cerebral palsy numbers and rates (excluding cases due to postneonatal causes) by gestational age in western Australia, 1981-1992. (Reprinted with permission from: Cerebral Palsies: Epidemiology and Causal Pathways. London: MacKeith Press; 2000; 151:26.)
Maternal risk factors for CP include Chorioamnionitis (18,19) or fever during labor, coagulopathy or bleeding (20), placental infarction, and thyroid disease (21). Postnatal risk factors for CP are often related to social disadvantage, and include trauma in developed nations (22) and infection in developing nations (23). Additional risk factors for CP include kernicterus (24), methyl mercury exposure (25), and genetic causes (26).
Severe birth asphyxia in term infants is not a major cause of CP. Less than 10% of children with the condition had asphyxia, in contrast to prematurity, which is associated with up to half of all cases of CP. Nonetheless, for children who have true birth asphyxia, the risk of CP is increased (27). Fetal monitoring in the United States has probably increased the rate of cesarean section deliveries, but has not been associated with any decline in rates of CP (28). Term infants described as having birth asphyxia often manifest certain signs, including acidosis, bradycardia, or neonatal encephalopathy. Intrauterine exposure to infection or a coagulation disorder can cause a similar clinical picture at birth and may be mistaken for complications of birth asphyxia. Birth asphyxia by itself accounts for a small minority of cases of CP (29). Neonatal encephalopathy generally is diagnosed in neonates with significant neurologic dysfunction, including respiratory difficulties, altered tone, low consciousness, or seizure activity. It is the best predictor of CP in term infants, regardless of the cause of the encephalopathy.