FEEDING AND SWALLOWING PROCESSES AND DISORDERS
During the first 12 months, infants have a number of unique anatomic and physiologic characteristics that gradually diminish with growth and maturation (Fig. 4.7) (45). For example, the larynx in infants is positioned higher in the neck than in older children and adults, with close approximation of the epiglottis and soft palate, resulting in added airway protection, as well as obligate nasal breathing (Fig.
4.7A, 4.7B) (46,47). This is important in promoting the suck-swal- low-breathe sequence, the most complex sensorimotor process undertaken by the newborn infant. Structural or functional abnormalities in the upper airway of infants put them at greater risk for feeding difficulties. Other unique features of infants include sucking pads in the cheeks to provide additional stability during sucking and a significantly larger tongue with respect to the oral cavity, which restricts tongue movement to the anterior-posterior direction characteristic of suckling.Infants also exhibit a number of unique physiological aspects that are important for successful feeding and swallowing. These include reflexes that assist with development of feeding, such as the suck-swallow reflex, the rooting reflex, and the phasic bite reflex. As cortical development advances, these automatic reflexes
id="Picutre 14" class="lazyload" data-src="/files/uch_group75/uch_pgroup296/uch_uch7172/image/image014.jpg">
Figure 4.7A The pharynx: infant.
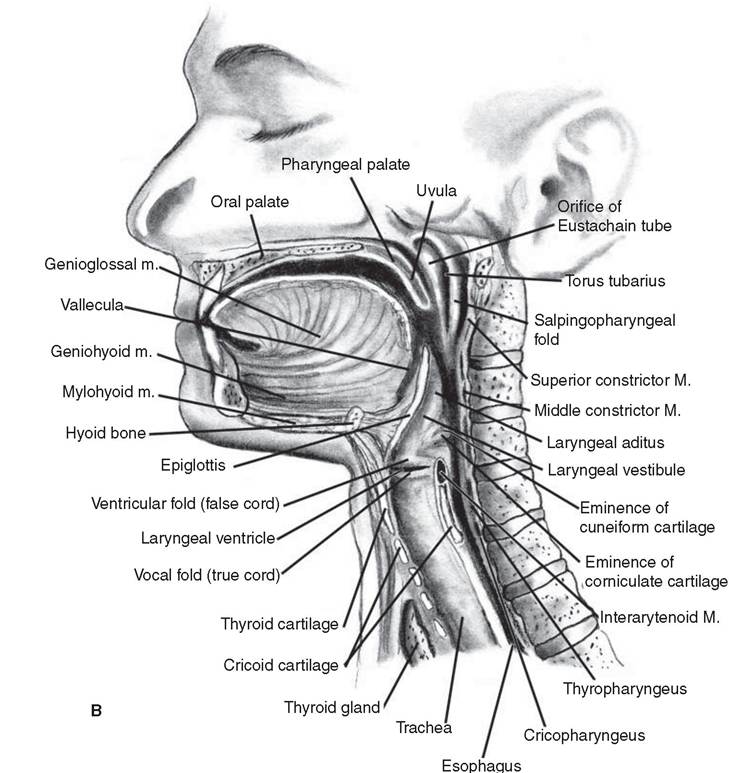
Figure 4.7B The pharynx: adult.
gradually evolve into more volitional actions, beginning during the period from 4 to 6 months of age. For example, at about 6 months of age, the transition from suckling to sucking begins to occur, with anatomic and neurologic maturation resulting in gradual lowering of the jaw, allowing more space for tongue movement, and gradual increase in volitional control permitting increased refinement and control of movements.
The development of motor milestones in infants and toddlers is accompanied by attainment of feeding and swallowing skills, as outlined in Table 4.12 (45,48).Critical periods are believed to exist in the development of normal feeding behavior. This can sometimes become problematic when caregivers are not sensitive to these critical stages. For example, caregivers may choose to maintain children on pureed foods due to apprehension regarding readiness to handle solid, chewable foods. However, research shows that delaying introduction of solid foods can result in food refusal and sometimes the development of food aversions (49). By the time children reach the age of 3 years, their ability to chew and swallow has matured and, with the exception of laryngeal position, their anatomy and physiology closely approximate those of the adult.
Infants with anatomical or physiologic abnormalities are at even greater risk for developing significant difficulty with establishing and maintaining oral feeding due to inability to initiate oral feedings within age- appropriate time frames. It is crucial for clinicians to have a thorough understanding of normal anatomical and physiologic development for feeding and swallowing in order to understand the implications of disorders.
Feeding and swallowing abilities involve multiple, interrelated anatomical and physiologic components within the body (eg, oral motor, pharyngeal, esophageal, respiratory, gastrointestinal). For this reason, effective management of children with feeding and swallowing disorders typically requires input from many specialists. These specialists may work separately or ideally may work within an interdisciplinary feeding
4.12
Attainment of Feeding and Swallowing Milestones
| AGE (MONTHS) | DEVELOPMENT/POSTURE | FEEDING/ORAL SENSORIMOTOR |
| Birth to 4-6 | Neck and trunk with balanced flexor and extensor tone Visual fixation and tracking Learning to control body against gravity Sitting with support near 6 months Rolling over Brings hands to mouth | Nipple feeding, breast, or bottle Hand on bottle during feeding (2-4 months) Maintains semiflexed posture during feeding Promotion of infant-parent interaction |
| 6-9 (transition feeding) | Sitting independently for short time Self-oral stimulation (mouthing hands and toys) Extended reach with pincer grasp Visual interest in small objects Object permanence Stranger anxiety Crawling on belly, creeping on all fours | Feeding more upright position Spoon feeding for thin, smooth puree Suckle pattern initially suckle→suck Both hands to hold bottle Finger feeding introduced Vertical munching of easily dissolvable solids Preference for parents to feed |
| 9-12 | Pulling to stand Cruising along furniture First steps by 12 months Assisting with spoon; some become independent Refining pincer grasp | Cup drinking Eats lumpy, mashed food Finger feeding for easily dissolvable solids Chewing includes rotary jaw action |
| 12-18 | Refining all gross and fine motor skills Walking independently Climbing stairs Running Grasping and releasing with precision | Self-feeding: grasps spoon with whole hand Holding cup with 2 hands Drinking with 4-5 consecutive swallows Holding and tipping bottle |
| 18-24 | Improving equilibrium with refinement of upper extremity coordination Increasing attention and persistence in play activities Parallel or imitative play Independence from parents Using tools | Swallowing with lip closure Self-feeding predominates Chewing broad range of food Up-down tongue movements precise |
| 24-36 | Refining skills Jumping in place Pedaling tricycle Using scissors | Circulatory jaw rotations Chewing with lips closed One-handed cup holding and open cup drinking with no spilling Using fingers to fill spoon Eating wide range of solid food Total self-feeding, using fork |
| Source: From Refs. 45,48. |
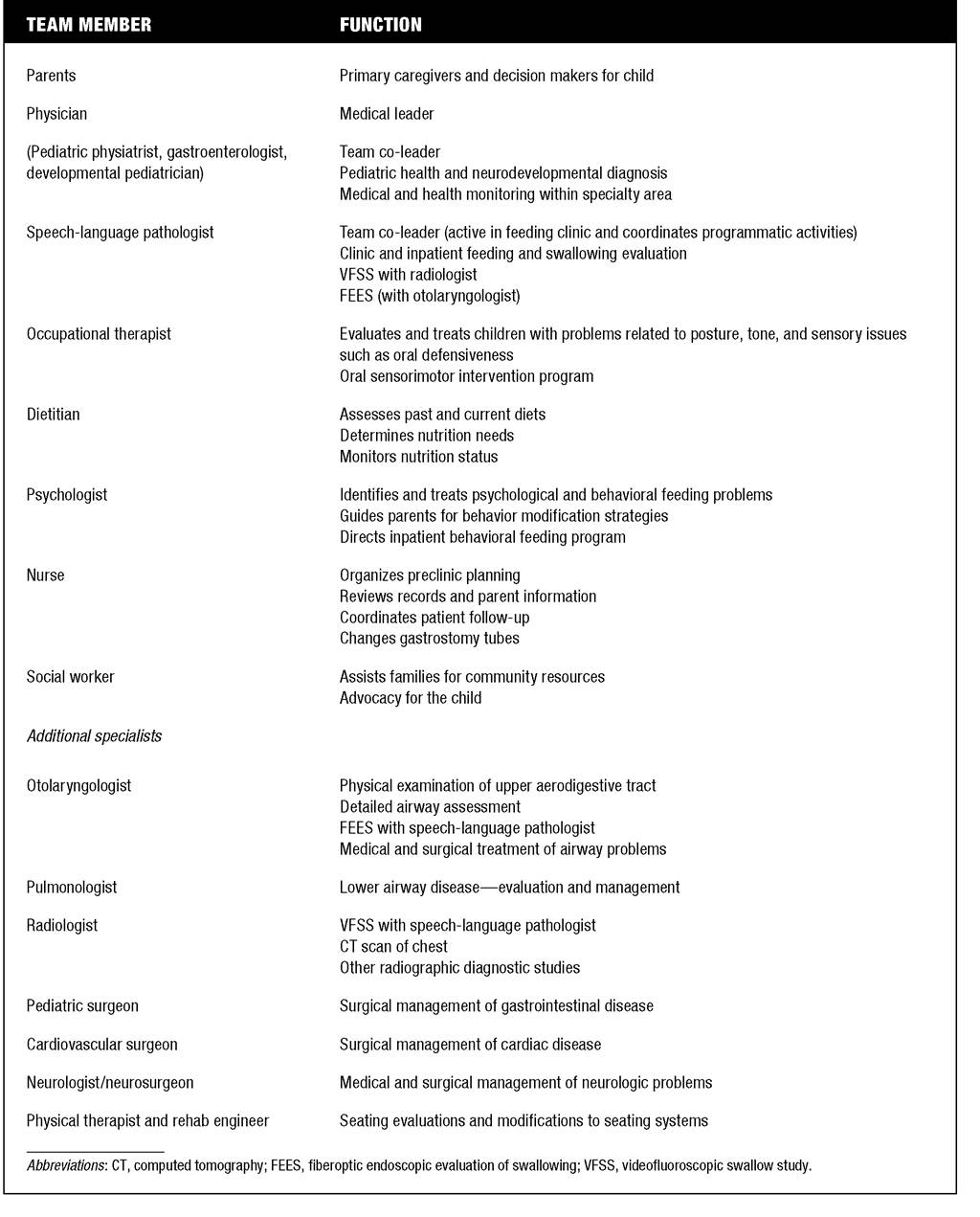
and swallowing team, providing the added benefit of coordinated care. An interdisciplinary approach is recommended at institutions where professionals evaluate and treat children with complex feeding and swallowing problems. Table 4.13 describes the members and functions of a comprehensive feeding and swallowing team.
Primary components of clinical assessment of pediatric feeding and swallowing skills include a thorough history, a prefeeding evaluation, and a feeding observation or trial feeding. If aspiration is suspected or risk of aspiration is a factor, instrumental assessments of swallowing, such as videofluoroscopic swallowing assessment (VFSS) or fiber-optic endoscopic evaluation of swallowing (FEES) may also be necessary following the clinical evaluation.
Feeding and swallowing difficulties can occur within a broad range of disorders, including anatomical or structural defects, neurologic deficits, systemic conditions, or complex medical conditions. Congenital
4.13
Feeding and Swallowing Team Members
anatomical or structural defects commonly affecting swallowing include tracheo-esophageal fistula (TEF), choanal atresia, and cleft palate. Acquired anatomical defects include laryngeal trauma. Neurologic deficits commonly affecting feeding and swallowing include cerebral palsy, traumatic brain injury, genetic syndromes, hypoxic/ischemic encephalopathy, meningitis, and Arnold-Chiari malformation. Systemic conditions typically associated with feeding and swallowing disorders include respiratory disease such as bronchopulmonary dysplasia (BPD) and Reactive Airway Disease (RAD), and gastrointestinal disorders such as gastroesophageal reflux (GER). Complex medical conditions resulting in swallowing disorders include prematurity and cardiac abnormalities. Given the interrelated nature of systems contributing to swallowing function, abnormalities (congenital or acquired) in any one of these systems can result in a feeding or swallowing disorder.
For example, premature infants or infants with cardiac abnormalities often have abnormally high respiratory rates. If respiratory rates are above 60 breaths per minute, successful feeding is often not possible because energy expended for breathing leaves no energy for feeding, resulting in breakdown in coordination and increased risk for aspiration (50). Infants and children with reflux are at increased risk for feeding difficulties, as reflux contributes to negative experiences associated with feeding (gastroesophageal pain/discomfort, aspiration), and subsequent feeding aversion may develop. Structural defects such as vocal fold paralysis, laryngeal cleft, tracheoesophageal fistula, glossoptosis, or choanal atresia can result in difficulty protecting the airway, resulting in aspiration. Thus, obtaining a thorough medical history is crucial to understanding the etiology of a child's swallowing disorder.In addition to medical history, a feeding history is important to obtain, as this will determine how to approach feeding assessment. If a child has been eating but his or her diet has been restricted to specific consistencies secondary to swallowing difficulties, this will be important to know. If a child has never been an oral eater, this is also critical information in subsequent clinical assessment decisions. Also, if a child has specific feeding utensils that he or she is accustomed to using, these should be used during the clinical assessment.
In addition to indirect assessment through parent interview and thorough review of medical records, direct observation of the child prior to introducing food should address alertness, ability to tolerate oral stimulation, and presence of a non-nutritive suck or ability to manipulate a bolus. Oxygen saturation and respiratory rate during these activities may need to be monitored. Positioning restrictions secondary to physical limitations or medical interventions should also be identified, as these may have an impact on the child's ability to feed.
A complete oral motor examination should also be completed to determine the presence of any structural or functional abnormalities of the oral musculature. Presence/absence of swallow response, laryngeal elevation, and vocal fold function should all be screened prior to introduction of food.With regard to level of alertness, children with TBI and associated cognitive impairment are at increased risk for aspiration related to decreases in cognitive level. A retrospective study completed by the authors found a significant correlation between Rancho Los Amigos Level of Cognitive Functioning and swallowing ability (51).
Regarding oral presentation of materials, there are a number of aspects to consider. Until recently, the Evan's Blue Dye Test or modified Evan's Blue Dye Test (MEBD) was commonly used to detect aspiration at the bedside. Its use has recently become somewhat more controversial. A recent report in the literature of a retrospective study comparing results from the use of MEBD, FEES, and VFSS documents low sensitivity of this measure to aspiration and cautions the clinician regarding false negative results (52). Another study, reported by Tippett and Siemens in 1996, notes 90% sensitivity of the MEBD in detecting aspiration of dyed foods for a group of 34 consecutive patients with tracheostomies (53). Thus, although the validity of the study for determining aspiration remains controversial and requires further objective study, it remains a useful component of the bedside swallowing assessment for some children in determining safety for oral intake.
When using foods during the bedside assessment, a number of variables can be manipulated, including the presenter, the consistency, the mode of presentation, and the bolus size (54). Food can be presented by the clinician, the parent, or the child, depending on the readiness and medical stability of the child and the availability and willingness of the parent. The child's age, current oral motor status, and premorbid feeding abilities will all affect decisions regarding consistency, mode of presentation, and bolus size.
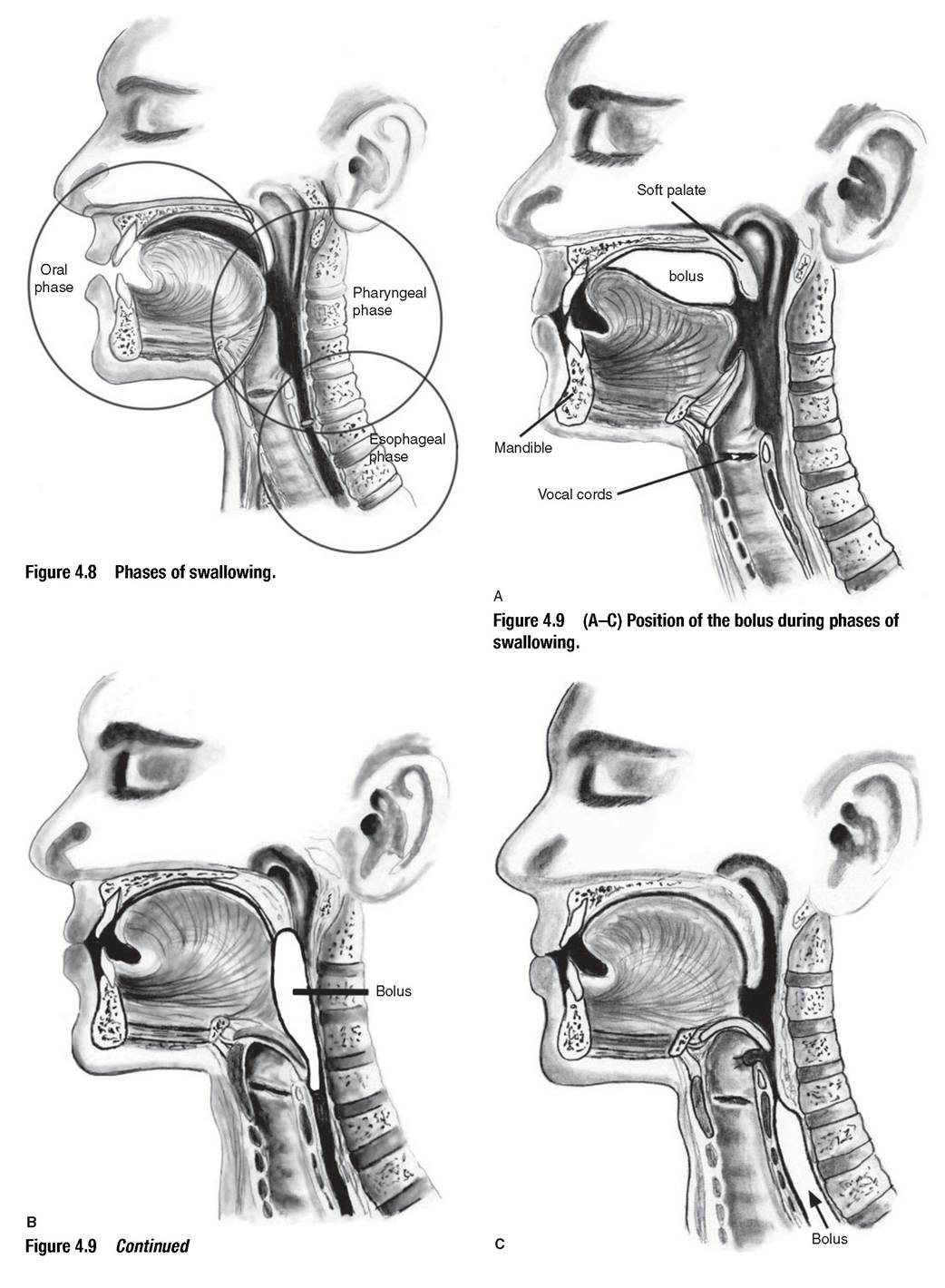
If aspiration is suspected during the bedside assessment (coughing/choking, drop in oxygen saturation, wet vocal quality), further instrumental assessment such as a VFSS is generally indicated. Instrumental studies will assist in providing more detailed information, such as when the aspiration occurs (eg, before, during, after the swallow), what factors caused the aspiration (eg, premature spillage, unprotected airway, cricopharyngeal dysfunction), and what compensations, if any (eg, food consistency, positioning, presentation), may improve the swallow. The VFSS assesses three phases of swallowing: oral, pharyngeal, and esophageal (Fig. 4.8) (55). Figure 4.9 illustrates the position of the bolus during each of the three phases.
If there is no evidence of aspiration during the bedside assessment, recommendations are made for oral feeding based on the results of the trial feeding, the child's level of ability to feed orally, and the child's nutritional needs.
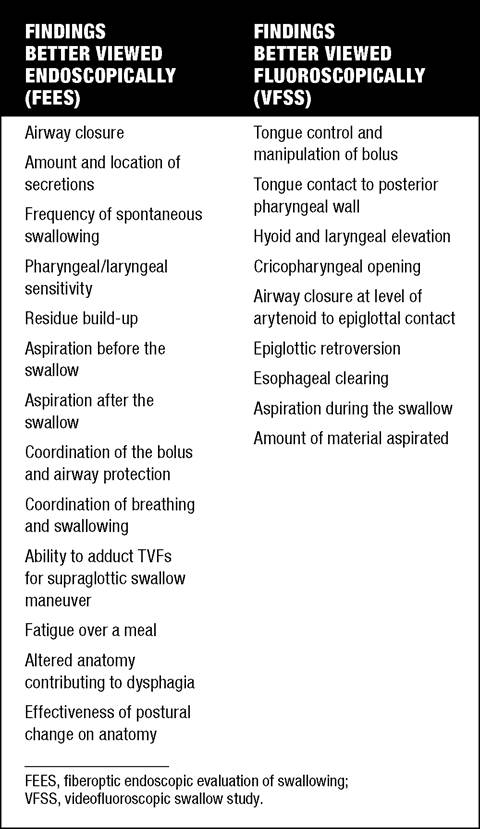
An alternative procedure, fiber-optic endoscopic evaluation of swallowing (FEES), is sometimes recommended instead of VFSS (56). It involves passage of a flexible fiber-optic endoscope transnasally to the area of the nasopharynx superior to the epiglottis, allowing observation of the swallowing mechanism from the base of the tongue downward. Use of FEES in the pediatric population has been established in the literature as a “practical and effective means of evaluating swallowing in children of all ages” (57,58). An advantage of VFSS is the ability to observe the actual aspiration event and to visualize the aspirated material in the airway. An advantage of FEES is the ability to observe amount and location of secretions and residue.
Instrumental examinations can be helpful in delineating pharyngeal and esophageal physiology as it pertains to swallowing. Decisions regarding when to perform an instrumental examination are guided by a number of factors, including risk for aspiration by history and clinical observation, documented incoordination of suck-swallow-breathe sequence during infant feeding, clinical evidence of pharyngeal or upper esophageal phase-swallowing deficits, prior aspiration pneumonia or similar pulmonary problems that could be related to aspiration, or etiology suspicious for pharyngeal or laryngeal problem, such as neurologic involvement commonly associated with feeding and swallowing problems.
Factors determining which type of instrumental exam to use are outlined in Table 4.14.
Management decisions with regard to feeding may be complex, and a number of factors must be considered, including medical, nutritional, oral sensorimotor, behavioral, and psychosocial. Treatment may include direct and indirect strategies, depending on the swallowing deficit. Examples of direct strategies include use of positioning maneuvers such as chin tuck or supraglottic swallow. Examples of indirect treatment strategies include diet modifications (eg, thickening liquids), changes in feeding routine (eg, small amounts frequently throughout the day), or changes in presentation of food (eg, Sippy cup versus bottle).
Diet texture modification is a common practice in management of dysphagia. Given the wide variation across clinicians and facilities, the American Dietetic Association attempted to establish some standard terminology and practice of texture modification through creation of The National Dysphagia Diet (NDD), published in 2002. The NDD was developed through consensus by a panel that included speech pathologists, dietitians, and food scientists. It proposes a hierarchy
4.14
Instrumental Swallowing Assessment
of four diet levels of semi-solids and solids, as well as two levels for liquids (see Table 4.15) (59).
One treatment option for children that is somewhat controversial involves oral sensorimotor intervention. This treatment method is typically performed by either speech pathology or occupational therapy, and involves techniques that are directed toward improving a child's ability to accept, manipulate, and swallow foods successfully. These techniques may include work with the jaw, lips, cheeks, tongue, and palate, both with regard to desensitizing and improving function. The benefits of such treatment approaches are still inconclusive, with little evidence to date documenting efficacy, efficiency, and outcomes. Some children appear to improve oral function with variations in texture, tastes, and temperature of foods. Other children benefit from posture and positioning changes. To be
4.15
Dysphagia Diet Levels
| DYSPHAGIA DIET CONSISTENCIES | EXAMPLES | INDICATIONS FOR USE |
| Thin liquids | Water, juice, soda | Adequate strength and coordination of lip and tongue musculature |
| Thick liquids | Nectars, milkshakes, cream soups. honey | Premature spillage of thin liquids with increased risk for aspiration |
| Mashed solids/purees | Yogurt, pudding, pureed meats and vegetables, cream of wheat | Mastication not required. Child may have weak tongue/mandibular musculature or reduced mastication. |
| Semi-solid | Minced meats/fish, cottage cheese, scrambled eggs, soft mashed fruits or vegetables | Some mastication possible. Fair oral motor control, although with some degree of oral weakness. |
| Soft chunk solid | Poached or hard-boiled eggs, bananas, canned fruit, mashable vegetables, bread, cold cereal, pancakes, pasta, rice, noodles, cake, pie | Mastication necessary. Appropriate for patients with adequate oral motor control but decreased endurance. |
| Source: From Ref. 59. |
most effective, treatment of swallowing disorders in children should ensure safety while promoting a pleasurable experience. Treatment should also include the primary caregiver in every session, as well as provide home programs and suggestions for how to work with children at home on a daily basis (60-62).
In conclusion, communication and swallowing are both complex acts that require coordination of multiple systems, and disruption in a single component in any one of those systems can and most often does result in some degree of communication or swallowing impairment. Assessment and treatment of these impairments requires thorough knowledge of development and disorders of relevant pediatric anatomy and physiology, as well as an understanding of how to apply that knowledge in evaluation and treatment to ensure the best possible outcome. As our field advances, and as we advocate for the most appropriate treatment for the children we serve, reliance on evidence-based practice has become, and will continue to be, a crucial component for success.