Functional Prerequisites for Walking
In their landmark paper published in 1953, Saunders, Inman, and Eberhart (27) described six gait subdivisions that they referred to as the “determinants” of normal
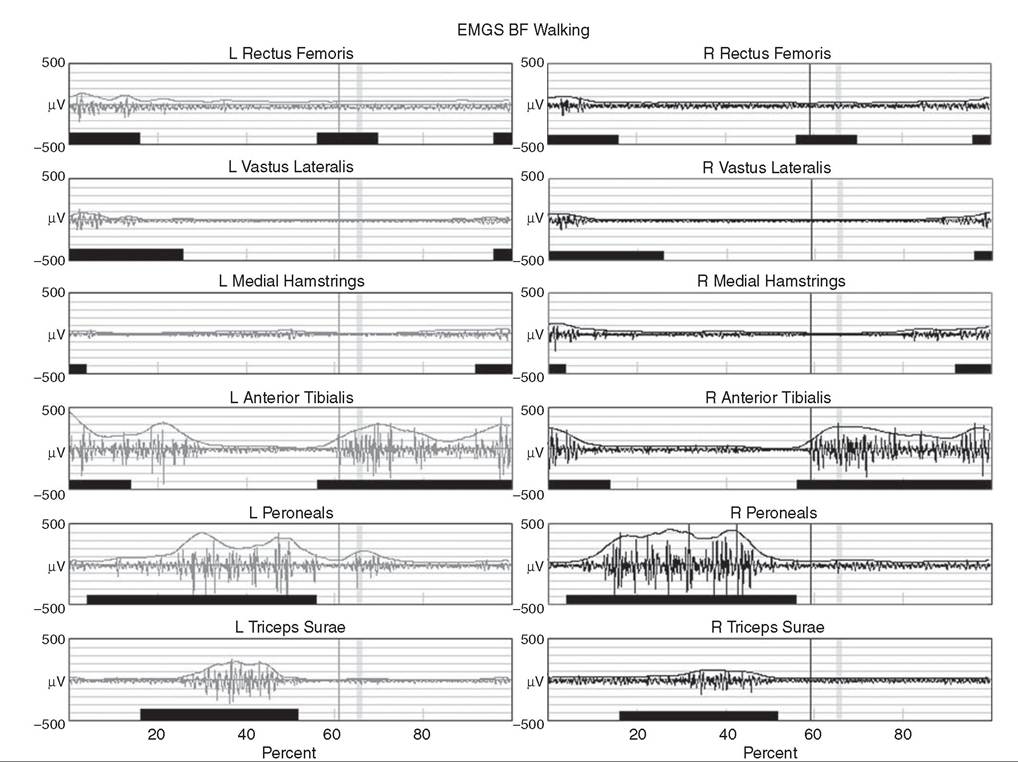
[Left BF I Avg EMG Control ∣ ∣~Right BF ∣
Figure 16.11 Filtered and time normalized EMG for 12 muscles of the lower extremity from a typically developing 15-year-old subject.
The black bars at the bottom of each graph are constructed from published normal EMG activations and are used as reference values. The smooth curve above the EMG activation is a processed EMG signal obtained by rectifying and integrating the raw EMG. Notice that each EMG activation pattern above a baseline level is contained within the reference bar indicating a normal EMG pattern. In this typically developing subject, there is very little EMG activity from the rectus femoris during initial swing.gait. This treatise was significant in that it was perhaps the first formalized delineation of the gait cycle that explained how coordinated movements of the hip, knee, and ankle at specific points in the cycle led to efficient forward progression. Each determinant’s influence on the three-dimensional path of the whole body center of mass (COM) was described using simple theoretical models, and the cumulative effect of all six determinants led to a smooth, low-amplitude trajectory that was assumed to be consistent with optimal, efficient locomotion. Specifically, Inman and colleagues believed that minimizing vertical and horizontal motion of the COM would maximize walking efficiency, since unnecessarily raising and lowering the COM would be wasteful from a potential energy perspective. By changing functional limb length with the addition of joints to an initially jointless model of the lower extremities and pelvis, each determinant served to smooth different portions of the COM trajectory, effectively raising the COM during double support and lowering it during single support.
While it is true that unnecessarily large and abrupt movements of the COM reduce gait efficiency, some of the specific determinants identified by Inman and colleagues have now been discredited (28,29,30). The improved accuracy and temporal resolution of kinematic measurement instruments over the last 50 years have uncovered problems with the timing of some of the theoretical mechanisms described in the original paper, and in the case of longer step lengths, larger COM displacements are not necessarily associated with decreased gait efficiency.While the relevance of specific determinants may now be in dispute, the real impact of this work is that it inspired generations of investigators to consider biomechanical explanations for gait dysfunction and led a few students of Dr. Inman's to develop clinically applicable gait cycle decompositions derived from the functional requirements of walking. In a later monograph, Inman described two basic functional requisites of walking that he deemed necessary for any form of bipedal gait, no matter how distorted by physical disability or assisted by prosthetic or orthotic devices (3): continuing ground reaction forces that support the body and periodic forward movement of each foot from one position of support to the next.
These essential features of walking give rise to a periodic gait cycle that must always be present for continued locomotion. An orthopedic resident of Dr. Inman's, Jacquelin Perry, recognized that the physical demands of supporting the body against gravity varied, depending on whether the stance limb was accepting the initial impact or continuing to carry the weight of the body during single support. To address this, she developed the notion of three functional gait tasks (31): weight acceptance, single limb support, and swing limb advancement. Dr. Perry considers weight acceptance the most demanding of the three functional gait tasks since it requires the stance limb's musculature and bony and ligamentous structure to provide shock absorption, initial limb stability (stiffness), and maintenance of forward progression.
Preparation for the demands of weight acceptance begin late in swing period, when prepositioning of the leading limb occurs to correctly align the foot to accept weight at initial contact. The physical demands are lower for the task of single limb support, despite the fact that one leg alone has the complete responsibility for supporting body weight, maintaining whole-body stability (balance), and restraining forward momentum. This reduced physical demand during the task of single limb support is due to the inherent passive stability provided by the knee ligamentous structure and the force balance at the hip as body weight moves forward (31). An essential functional requirement for this task is strong eccentric contraction of the calf musculature to control the tibia (and subsequently the rest of the stance limb) as it rotates over the fixed base of support provided by the foot. When the task of single limb support ends and swing limb advancement begins, the physical demands increase once again, since the three goals of weight transfer, limb advancement, and foot clearance must all be accomplished. Similar to the weight acceptance task, important preparatory actions must begin before the swinging limb is lifted from the supporting surface at the end of stance period to meet the functional demands of swing limb advancement.Findings from other investigators support the existence of these three fundamental gait tasks, although each investigator has used a somewhat different terminology when describing them (Table 16.1). Winter has characterized walking as an extremely complex motor control task that requires three elements: support control to prevent collapse against gravity (32); balance control of the head, arms, and trunk (HAT) acting as an inverted pendulum (33); and safe and coordinated lower limb movement during swing for minimum foot clearance and gentle heel contact (19). Dr. Winter and colleagues have also stated that the goals of these tasks can still be accomplished after disease, injury, or loss of function because of the inherent redundancy of lower extremity musculature and rapid adaptability of the central nervous system (34).
It is interesting that Perry and Winter have identified essentially the same three gait tasks, despite approaching the study of gait from two different perspectives: clinical analysis of pathologic gait and biomechanics of human movement, respectively. This lends support to the existence of these three elements and warrants using them to understand functional deficits in subjects with gait pathology.16.1
Functional Subdivisions of the Gait Cycle Attributed to Different Investigators
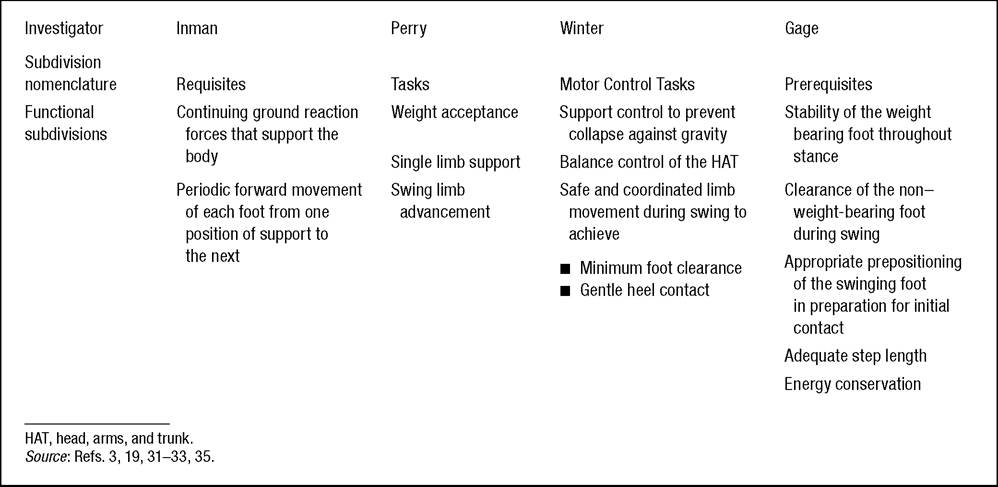
Gage has expanded on this description by identifying five elements essential to walking that he has referred to as “priorities” or “prerequisites” of normal gait (35). This functional subdivision of the gait cycle encompasses the three tasks described previously, but adds swing period elements necessary to ensure appropriate weight acceptance and the global task of energy conservation. In the order of functional priority, these are stability of the weight bearing foot throughout stance, clearance of the non-weight bearing foot during swing, appropriate prepositioning of the swinging foot in preparation for initial contact, adequate step length, and energy conservation. This prioritization is influenced by Dr. Gage's interest in the gait of children with cerebral palsy, and includes a gait efficiency task (energy conservation) to address the reduced functional capacity or endurance of many individuals with pathologic gait. He also identifies several physiologic and biomechanical mechanisms common to normal gait that can improve energy conservation. These are eccentric muscle contraction, return of “stretch energy” from prestretched muscles immediately prior to concentric contraction, bi-articulate muscles functioning as energy transfer straps, and joint passive stability from the effects of ground reaction forces whenever possible to spare muscle activation (36). While other investigators have addressed the functional prerequisites of gait (15,25,37), the contributions described previously form the basis of the strategy described in this chapter.