GIARDIASIS
Giardiasis is a common cause of chronic diarrhea or malabsorption in children, especially those with poor sanitation, malnutrition, immunodeficiency states and institutionalization, e.g.
daycare centers or orphanages. Epidemiology: Giardia lamblia exists in two stages— cysts in the environment and trophozoites in intestinal lumen. Infection is acquired feco-orally, after ingestion of contaminated water.After ingestion, each cyst liberates 2-4 trophozoites, which colonize the duodenum and proximal jejunum (site of infestation) by attaching themselves to brush borders with their powerful sucking discs. Later, some detached trophozoites pass-down and encyst again, to appear in stools for further transmission.
Malabsorption in Giardia-infested children is attributed to—(a) mechanical damage to microvilli by trophozoite discs, causing disaccharidase deficiency,
(b) pancreatic injury with reduced tryptic activity and
(c) bacterial overgrowth in duodenum, causing bile-salt deconjugation.
Clinical manifestations: After incubation period of 1-2 weeks, giardiasis may manifest as:
• Asymptomatic excretion of cysts (carriers),
• Acute, explosive, watery, foul-smelling diarrhea, lasting for 3-4 days,
• Chronic malabsorption with intermittent diarrhea, steatorrhea, flatulence and failure to thrive.
Diagnosis requires demonstration of cysts or trophozoites in stools or duodenal aspirate/biopsy, later being the best specimen to detect asymptomatic infestation. At least 3 fresh stool samples should be examined for giardia, collected on alternate day after discontinuation of anti-parasite drugs (Fig. 14.2).
Serodiagnosis of giardia antigen in stools, using monoclonal antibodies is possible, but rarely used.
Management: All cases including asymptomatic carriers need treatment with:
• PO Metronidazole (15 mg/kg/day q8hr) for 5 days, or
• PO Tinidazole (50 mg/kg single dose above 3 years), or
• PO Nitazoxanide (100 mg 1-3 yr, 200 mg 3-12 yr, 500 mg gt;12 yr per dose, BD ? 3 days), or
• PO Albendazole (400 mg OD ? 5 days, above 6 years)
Repeat stool exam is necessary to ensure eradication of infection.
Persistence of infection despite repeated therapy indicates possible immunodeficiency state.Prevention depends on improved sanitation and safe water supply. Micropore filtration (lt;5 mm) or boiling of drinking water is effective to eliminate/kill the cysts, but chlorination in usual doses or ultraviolet radiation is ineffective.
10.36 INTESTINAL WORM INFESTATIONS
Intestinal worm infestations are estimated to be present in ~20% of under-five children in India and WHO classifies India as a moderated-risk country for worm infestations. Some important worm infestations in children are as follows.
Ascariasis: Ascariasis (round worm) is the ubiquitous worm infestation of mainly pre-school and early- schoolchildren, specially in low-hygiene population.

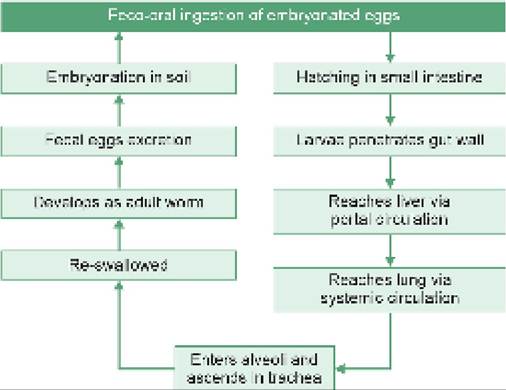
Fig. 10.22: Life cycle of Ascaris Iumbricoidus.
Life-cycle: Heterosexual adult worm (A. lumbricoidus) lives in small intestine, with a lifespan of 1-2 years. Female worms are longer (20-30 cm) than males (12-20 cm) and lay up to 2 lac eggs/day, which are excreted in feces. These eggs embryonate in soil and turn infective after 2-3 weeks.
Infective (larva-containing) eggs are feco-orally transmitted to another host via soil-contaminated fingers or uncooked food items. Promiscuous defecation and use of human feces as manure are two important risk factors in transmission.
On ingestion, eggs hatch in small intestine and larva penetrate the gut wall to reach the liver and then the lungs via blood stream. In lungs, they mould twice before breaking alveolar walls to enter bronchioles, ascend to trachea and re-swallowed. On reaching the intestine second-time, these larvae develop into mature worms, lay eggs and continue the cycle (Fig. 10.22).
Clinically, ascariasis is asymptomatic or present with:
• Vague features, e.g. abdominal discomfort, malabsorption and undernutrition in heavy infestation.
• Mechanical obstruction, e.g.
airway obstruction during larval migration, intestinal obstruction due to mass of adult worms, or rarely, biliary obstruction by migrating worm with obstructive jaundice.• Immune-mediated pulmonary manifestations, e.g. Loffler-like syndrome.
• Passage of adult worms in stools/vomitus.
Diagnosis depends on: (a) history of passing worms in stools/vomitus, or (b) stool microscopy (Kato's thick smear) to demonstrate presence of fertilized/unfertilized eggs (Fig. 14.2). Presence of fertilized eggs in stool indicates bi-sexual infestation.
Treatment of choice is single oral dose of Albendazole 400 mg (200 mg lt; 2 yrs). Alternatives include other oral wormicidal drugs, e.g. Mebendazole (100 mg BD x 3 days)
or Ivermectin (150-200 #956;g#8725;kg once). Nitazoxanide, a broad-spectrum drug may also be used orally as 100 mg BD x 3 days (400 mg BD in 4-12 years age group and 500 mg BD in adolescents).
In cases with intestinal or biliary obstruction, Piperazine citrate is preferred due to its neuroparalytic reaction on worms, which facilitates their expulsion. Surgical intervention may be needed in cases with severe obstruction.
Prevention: Community load of round worm may be reduced by: (a) mass deworming of pre-school children every 3-6 months, (b) hygienic sanitary/excreta-disposal practices, and (c) reduced use of human feces as manure. Toxocariasis (visceral or ocular larva migrans) is an accidental human infestation by primarily zoonotic ascarids, i.e. T. canis (dogs) or T. catis (cats).
Life-cycle involves excretion of eggs in animal excreta gt; accidental feco-oral infection of children via contaminated fingers or food gt; hatching and larval release gt; gut penetration gt; migration to different tissues, e.g. lungs, liver, eyes, brain, etc. Toxocara larva do not develop beyond this stage in human host (no adult worms).
Clinically, these cases may present with: (a) immunological reactions, e.g. fever, hepatomegaly, urticaria, Loffler syndrome, or (b) mechanical damage due to migrating larvae, e.g.
sudden decrease in visual acuity or blindness (ocular larva migrans).Diagnosis rests on visualization of larvae in the tissues or an antibody-ELISA test (rarely available). History of frequent dog/cat exposure and eosinophilia is common. Treatment is non-specific, including steroids for allergic manifestations, e.g. urticaria or Loffler syndrome. Antihelminthic therapy (PO Albendazole 400 mg BD ? 5 days) is indicated only in symptomatic cases, along with steroids to reduce inflammatory response to antigens released from dying parasites. Longer therapy for 3-4 weeks is needed in ocular or neurological disease.
Enterobiasis: Enterobiasis (Threadworm or Pinworm) is the commonest worm infestation in pre-school children, which is essentially harmless except inconvenient perianal itching.
Life-cycle: Causative adult worm E. vermicularis is ~0.5-1 cm in size and lives in caecal region of infested human host. Gravid female migrates externally through the anus during night, to lay eggs over perianal area. These eggs mature here as infecting larvae in 6 hours and remain viable for next 20 hours.
While a new host is infected feco-orally, same host may also be re-infected by auto-inoculation of eggs, carried under fingernails after perianal scratching. On ingestion, these eggs hatch in stomach, larvae migrate to caecal
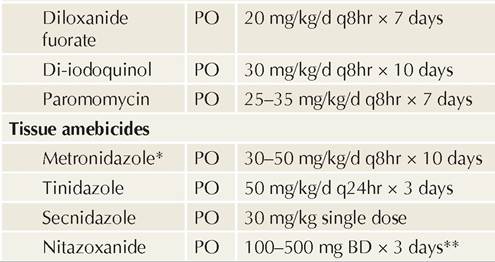
Fig. 10.23: Life cycle of E. vermicularis.
region and mature as adult worms to continue the cycle (Fig. 10.23).
Clinically, nocturnal perianal pruritis is the commonest manifestation of enterobiasis, leading to disturbed sleep. Very rarely, perianal granuloma containing live/dead worms or eggs have been reported.
Diagnosis: As eggs are generally not passed in stools, definitive diagnosis depends on demonstration of eggs (Fig. 14.2) in perianal region or adult worms in stools or at perineal region.
Best method to demonstrate enterobius eggs is to stick an adhesive cellophane tape against perianal region in early morning and examine under microscope.
Treatment of choice is single oral dose of Albendazole 400 mg (200 mg lt; 2 years), though alternatives include other wormicidals, e.g. Mebendazole (100 mg once) or Pyrantel Pamoate (11 mg/kg base TDS x 1 day). It is to be noted that:
• Treatment should be repeated after 2 weeks in all cases, to eradicate residual infestation, and
• All family members should be treated simultaneously, to prevent cross-infection.
Soothing creams, e.g. crotamitone, may be applied to relieve perianal itching and prevent auto-inoculation. Prevention: Personal cleanliness with regular trimming of nails and periodic de-worming of susceptible population are important measures to prevent threadworm infestations.
Trichuriasis (Whipworm) is a common infestation in children, though rarely diagnosed due to lack of symptoms.
Life cycle: Adult worm T. trichuria (~ 3-4 cm) lives in cecum and ascending colon, firmly anchored to mucosa to suck ~ 0.005 ml blood/day. Infection is transmitted feco-orally, on ingestion of embryonated eggs in contaminated hands, food or water.
Clinical manifestations are rare and include: (a) vague abdominal discomfort, e.g. colic or distension, or (b) mild anemia, bloody diarrhea or rarely rectal prolapse in heavily parasitized host.
Diagnosis depends on stool examination for typical eggs (Fig. 14.2).
Treatment of choice is PO Albendazole 400 mg x 3 days (200 mg lt; 2 years), though alternatives include PO Mebendazole 100 mg BD or Ivermectin 200 pg/kg/d, both for 3 days.
Ankylostomiasis: Ankylostomiasis (Hookworm infestation) is an important cause of iron deficiency anemia in Indian children, usually caused by Ancylostoma duodenale, and occasionally by Necator amaricanus.
Life cycle: Hetrosexual adult worm (5-13 mm) lives in small intestine, firmly attached to the gut mucosa with their typical hooks or teeth. Female worms produce up to 30,000 eggs/day, which are excreted in stools to develop as infective larvae in warm and damp soil.
Infection is usually acquired via cutaneous penetration over feet, especially in bare-foot walkers (rarely feco- oral). After skin-penetration, larvae enter the venous circulation to reach lungs, where it comes out of the vascular bed to enter in alveoli, ascend into airways and get swallowed. On reaching the small intestine, it develops into adult worms, attaches itself to intestinal walls and starts oviposition (Fig. 10.24).
Bare-foot walking on infested soil, poor sanitary conditions and use of human feces as manure, are the main risk factors for hookworm infestation, which is common in rural and slum population.
Clinically, anemia due to intestinal blood loss by hooked attachment of adult worms is the most important manifestation of ankylostomiasis and its severity depends on worm-load. Each adult worm is responsible for ~ 0.2-0.3 ml of blood loss per day.
Other manifestations include: (a) non-specific GIT problems, e.g. abdominal pain, anorexia, diarrhea, and melena; (b) localized itching (ground-itch) at the site of skin entry*, and rarely, (c) transient stridor or pharyngitis, during airway migration of larvae.
*Typical cutaneous larva migrans is seen only with some zoonotic worms, e.g. A. braziliense.
Diagnosis should be suspected in cases with unexplained anemia and occult blood in stools, confirmed on stool examination for eggs (Fig. 14.2).
Treatment of choice includes single oral dose of Albendazole 400 mg (200 mg lt; 2 years), though alternatives include other oral wormicidal agents, e.g. Mebendazole 100 mg BD x 3 days or Pyrantal pamoate 11mg#8725;kg/ day OD for 3 days. Repeated doses may be required for complete eradication.
In addition, these patients also need correction of anemia by oral iron therapy or rarely blood transfusions. Prevention depends on community measures, e.g. (a) periodic deworming, (b) avoidance of bare-foot walking,
(c) improvement of sanitation and excreta disposal, and
(d) reduced use of fecal manure.
Strongyloidosis (S. stercolaris) is an uncommon infestation, acquired via skin penetration by infective larvae in feces-contaminated soil.
Life-cycle is similar to hookworm, except that eggs often hatch in vivo during intestinal passage and infective larvae re-enters the circulation by penetrating intestine walls or perianal skin (auto-inoculation).
Clinically, it is asymptomatic or present with: (a) perianal itching due to auto-inoculation (larva currens), (b) Loeffler's-like syndrome with eosionophilia due to larval migration through lungs, (c) malabsorption syndrome in heavy infestations, and (d) rarely, disseminated Strongyloidosis—a septicemia-like illness in severely malnourished or immunocompromised children.
Diagnosis depends on examination of stools or duodenal aspirate for characteristic larvae.
Treatment: PO Ivermectin (200 #956;g#8725;kg#8725;d) for 1-2 days is the drug of choice. PO Thiabendazole 50 mg/kg/d q12hr is an alternative, specially in disseminated disease. Cestodal (Tapeworm) infestations: Human cestodal (tapeworm) infestations present in two forms—(a) intestinal infestation by adult worms, and (b) tissue infestations by invasive stages, e.g. hydatid cyst and neurocysticercosis.
a. Intestinal tapeworm infestations are less common in children than in adults, caused by Taenia solium (Pork tapeworm), T. saginata (Beef tapeworm), Diphyllobothrium latum (Fish tapeworm) and Hymenolepis nana (Dwarf tapeworm).
Life-cycle: These infestations are acquired by ingestion of—(a) parasitic eggs, present in contaminated soil/ water or over the body of intermediate hosts; or (b) uncooked beef, pork or fish, containing invasive stages of parasite.
Adult tapeworms are present only in human intestines and have long, segmented (proglottids) bodies of variable length (fish tapeworm is longest, 10-20 meters). On maturation, caudal gravid segments detach intermittently to pass in stools and release eggs in the soil.
Although entire life-cycle may be completed in humans alone (except D. latum*), animals, e.g. dogs, pigs, cattle, etc. are frequently infected by ingestion of egg-contaminated soil or invasive-stage-contaminated flesh of infected animals, to contribute in propagation of disease (Co-hosts).
*D. latum requires hatching of eggs in fresh water and subsequent passage of embryo through two intermediate hosts,
i. e. copepods—small crustaceans, which swallow the eggs/ larvae and fishes that eat these crustaceans, before re-infecting humans on ingestion of uncooked fish.
Clinically, intestinal tapeworm infestation is asymptomatic or presents with vague abdominal complaints, except D. latum infestation, which may cause megaloblastic anemia by inhibiting vitamin B12 absorption and utilizing it for own metabolism.
Diagnosis depends on presence of proglottids (on naked eye) or eggs (on microscopy), in stools or rectal swabs.
Treatment of choice for all intestinal tapeworms is single oral dose of Praziquantel (25 mg/kg) or Niclosamide (50 mg/kg). PO Nitazoxanide 100 mg BD x 3 d (400 mg BD in 4-12 years age group and 500 mg BD in adolescent and adults) may also be used. Simultaneous treatment with polyethylene glycol can increase fecal yield of scolices.
Prevention involves adequate sanitation, proper excreta disposal and avoidance of eating uncooked meat/fish.
b. Hydatid cyst is caused by intermediate (invasive) form of Echinococcus granulosus-a zoonotic tapeworm in dogs or other canines.
Pathogenesis: Humans are accidentally infected by ingestion of the intermediate forms of parasite, present in contaminated water/food or over fecal- contaminated body of infected dogs. Ingested intermediate forms penetrate the gut-wall, carried via lymphatics/blood to liver, lung, bones, etc., and develop into gradually enlarging cysts.
Structurally, these cysts are surrounded by a tough fibrous capsule of host tissue, lined by inner layers of parasitic origin and contain thousands of parasites (protoscolices) along with cystic fluid.
Clinically, lung cysts are more common in children, while liver cysts are commoner in adults. Hydatid cysts may be asymptomatic or present with mass effect, i.e. (a) hepatomegaly with palpable mass and pain in liver cysts, (b) cough, hemoptysis and chest pain in lung cysts, and (c) pathological fractures in bone cysts.
Complications include: (a) cyst rupture (spontaneous or during surgery) which may lead to sudden anaphylaxis and/or formation of secondary cysts, and (b) pressure on other structures, e.g. biliary tree with obstructive jaundice.
Diagnosis depends on: (a) ultrasonography, i.e. cystic lesion with internal membranes and floating echogenic cyst material (Hydatid sand), and (b) Casoni's skin test, to detect hypersensitivity against crude or partially purified antigen. It may be false-negative in 50% cases and false-positive in other tissue helminthes, e.g. neurocysticercosis or schistosomiasis.
Treatment depends on the size and site of cyst and includes:
± Conventional surgical removal of cyst as a whole (except outer fibrous wall) for large and complicated cysts,
± PAIR technique, i.e. USG or CT guided percutaneous aspiration gt; instillation of hypertonic saline or other scolicidal agent gt; re-aspiration after 15 minutes. PAIR is contraindicated in pregnancy or bile containing cysts.
± Medical therapy for multiple, small, deep-seated cysts, with albendazole (PO 7.5 mg/kg BD) for 1-6 months. Medical therapy is also indicated when surgery is contraindicated or one week before and one month after PAIR.
c. Neurocysticercosis (NCC) is the commonest parasitic infection of CNS, caused by the invasive intermediate stage of T. solium (pork tapeworm), with formation of asymptomatic or symptomatic cysts in the brain (see Ch 18.12.9 for details).
Trematodal (Fluke) infestations are uncommon in Indian children and characterized by their typical lifecycle involving two hosts-man for sexual phase and snails for asexual phase.
According to preferential tissue-habitat, trematodal infestations are also termed Blood flukes, (Schistosoma hematobium) Liver flukes (Fasciola hepatica, Clonorchis sinensis) and Lung flukes (Paragonimus westermani).
Schistosomiasis is the commonest trematodal infestation, acquired via cutaneous penetration by the infective larvae, i.e. cercariae, present in contaminated water bodies and on aquatic plants. Post-entry, cercariae migrates via subcutaneous tissue, lungs and liver; and develops as adult worms (sexual stage) that reside in the venous plexus surrounding ureters and urinary bladder.
Oviposition occurs intravascularly and eggs are intermittently excreted in urine, after rupture of invaded capillaries. Further development from egg to infective larvae (asexual stage) occurs only in fresh-water snails (intermediate host), to continue the cycle.
Clinically, these cases present with—(a) local pruritic rash at the portal of entry (Swimmer's itch), (b) acute febrile illness with eosinophilia after 4-8 weeks of infection (Katayama fever), or (c) chronic granulomatous injury at the site of parasitic deposition, e.g. periureteic/ perivesicular venous plexus, leading to hematuria.
Diagnosis depends on urine examination for schistosome eggs.
Treatment of choice is PO Praziquantel 20 mg/kg, total two doses at 12-hour interval.
10.37