AMEBIASIS
Amebiasis, a common waterborne illness in India, is relatively less common in children than adults.
Epidemiology: Causative protozoan Entamoeba histolytica exists in two different forms—cysts, in contaminated water/food; and trophozoites in human intestines.
Infection is acquired feco-orally on ingestion of parasitic cysts (not by trophozoites, which rapidly degenerate by gastric acid).On ingestion, each cyst liberates eight trophozoites in small intestines, which are passed further to attach and penetrate colonic mucosa. Some trophozoites encyst again, to be excreted in stools.
Invasive trophozoites may multiply locally to produce flask-shaped colonic ulcers in cecum, transverse and sigmoid colon (intestinal disease) or enter portal circulation to invade liver (extra-intestinal disease).
Minimal local inflammatory response in colonic ulcers or at the site of extraintestinal disease is pathognomonic of amebic lesions.
Clinical spectrum: 90% of amebic infections are asymptomatic except intermittent passage of cysts in the stools (carriers). Symptomatic disease may be intestinal and extra-intestinal:
• Intestinal amebiasis manifests after 2-3 weeks of infection with gradual onset of: (a) diarrhea or dysentery with blood and mucus, (b) colicky abdominal pain or sense of fullness, (c) vague tenderness over iliac region, and (d) characteristic absence of constitutional features, e.g. high fever, toxemia, etc.
Rare cases develop chronic colitis with recurrent bouts of dysentery and abdominal cramps, often confused with inflammatory bowel disease.
[*] Extraintestinal amebiasis is seen in lt;1% of infected cases, usually as hepatic abscess. Rarely, these abscesses may rupture in peritoneum, plural space or through the skin.
Amebic liver abscess usually involves the right lobe and may be single or multiple, filled with typical anchovysauce colored sterile pus. These cases present with—(a) fever with chills/rigors, (b) right hypogastric pain, and (c) tender hepatomegaly on deep palpation.
History of intestinal disease and stool examination is negative in gt;50% cases.TABLE 10.59: Common anti-amebic agents
Luminal amebicides
*or 20 mg/kg/d IV
**100 mg (1-3 yr), 200 mg (3-12 yr), 500 mg (gt;12 yr)
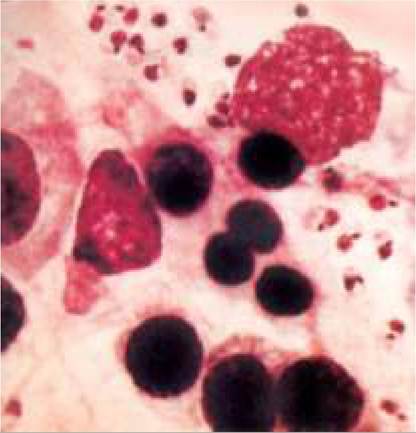
Diagnosis of intestinal amebiasis is confirmed by stool examination for cysts/trophozoites (Fig. 14.2), while extraintestinal disease may be diagnosed by—(a) USG, (b) aspiration of suspected lesion to reveal anchovysauce pus with paucity of granulocytes, (c) indirect hemagglutination test (gt;1:128) with ~ 95% sensitivity.
Management: All children with E. histolytica in stools, even if asymptomatic, need to be treated. Metronidazole is the drug of choice for intestinal as well as extraintestinal disease, while luminal amebicides are preferred in asymptomatic case to eradicate carrier stage.
• In symptomatic intestinal amebiasis, a course of tissue amebicide, e.g. Metronidazole, Tinidazole or Nitazoxanide should be followed by a course of luminal amebicide, e.g. Diloxanide, paromomycin or Di-iodoquinol to ensure complete parasitic clearance (Table 10.59).
• In extra-intestinal amebiasis, IV Metronidazole (20 mg/ kg/day q12hr) is used for first few days, followed by oral therapy. Dehydroemetine or chloroquine are very rarely used in children. Amebic abscess needs to be drained only if-(a) poor therapeutic response after one week, (b) massive abscess with impending rupture.
Prevention depends on proper sanitation measures and boiling of drinking water. Chlorination in usual doses is ineffective to destroy the parasite. Stool examination of all cases and carriers should be repeated after 2 weeks of therapy to ensure parasitic clearance.
10.36.2