Idiopathic Scoliosis
More than 80 percent of scoliosis cases belong in the idiopathic category, which is subgrouped into three types defined by age of onset (Table 14.6). All differ significantly in demographic distribution, progression, and treatment type.
Infantile
Infantile scoliosis is rare and is not related to a vertebral defect, but has an unknown etiology. It occurs within the first three years of life and often spontaneously resolves.
Left thoracic curves are common in infantile scoliosis, and boys are predominantly affected. Plagiocephaly, developmental dysplasia of the hip, and congenital muscular torticollis are often associated, so radiographs of the spine and hips and MRI of the brainstem and spinal cord should be obtained (288). Neuromuscular disease, congenital scoliosis, and intraspinal pathology (Chiari malformation, tumor) must be ruled out.
Large curves in infants over a year of age may progress and require bracing or body casting. Curves over 40 degrees require surgery to avoid cardiopulmonary compromise. VEPTR or “growing rod” technology may be used in curve management. If fusion is needed, trunk height will be lost and anterior-posterior procedures will be needed to prevent the risk of crankshaft deformity.
Juvenile
Juvenile scoliosis appears equally in males and females between the ages of 3 and 10 years, and is unfortunately aggressive, with about 70 % of children requiring treatment—either bracing (50%) or surgical intervention (50%) (282). Tumors or spinal abnormalities may be causative, and an MRI of the spine and brainstem, along with radiographs, are necessary for a thorough evaluation. Progression is related to age of onset (Fig. 14.22).
Bracing may be effective, but the social impact of long-term bracing in this age group may be significant, and surgical intervention with “growing rod” systems is recommended once the curve reaches over 40-50 degrees.
In a child older than 8 years and categorized as Risser 0, if a fusion is done, an anterior-posterior fusion will typically be performed to avoid crankshaft problems.Adolescent
Idiopathic scoliosis developing after age 10 is the most common form of scoliosis, and occurs in about 25/1,000 adolescents. The incidence is greater in females, as is the tendency to progress with a right thoracic curve.
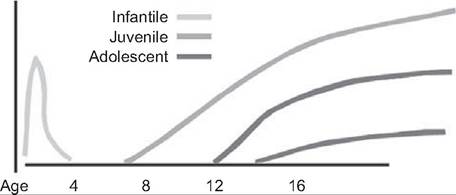
Figure 14.22 Natural history of idiopathic scoliosis. Progression is related to the age of onset of the scoliosis. (Adapted from Ref. 284.)
A left thoracic curve in an adolescent male is suspect, and causality should be further investigated. The exact etiology of idiopathic scoliosis is unknown, but genetics play a role, as about 30% of patients have a positive family history, and there is 50% concordance among twins (282,285/. A multifactorial etiology related to growth hormone and melatonin production, connective tissue and muscle structure, and platelet function have all been postulated, but research is inconclusive (290). Fortunately, most curves are fairly benign and only about 10 % require treatment other than observation (288). More than 90% can be controlled effectively with bracing for curves between 20 and 40 degrees. Effective control means no progression of curve beyond 5 to 7 degrees after onset of bracing (285). Progression also relates to age of onset (see Fig. 14.22).
Curve Progression. Curve progression depends on several factors, including age of onset, curve size, and level of skeletal maturity. Young (20 degrees) are most at risk. In the past, spinal and abdominal exercises were recommended to help reduce curve progression, but while these help maintain range of motion and fitness, there is no evidence that they prevent scoliosis (291).
Curves less than 25-30 degrees that are not progressing can be observed serially, especially if the child is approaching skeletal maturity.
Brace wear, while difficult in adolescence, is still a standard of care for reducing curve progression, although there is no level 1 evidence in favor of bracing. A randomized, controlled, multicenter, National Institutes of Health (NIH) study is currently underway. Bracing is recommended for curves over 20 degrees in a skeletally immature patient in whom only 5-10 degrees of progression has been noted over a six-month period. Wearing the orthosis 16-24 hours a day is suggested until skeletal maturity is reached, at either Risser stage 4 in girls or stage 5 in boys, or two years postmenarche (292). Brace wear is discontinued in lieu of surgical intervention generally if the curve exceeds 40 degrees or more rapid progression is noted.Treatment in adolescence is important because psychological distress and social limitations have been noted in adult females who have disfiguring curves greater than 40 degrees (281). Curves less than 40 degrees at skeletal maturity do not tend to progress in adulthood, but curves over 50 degrees, especially in the thoracic area, can. Progression of just 1 degree per year in adulthood can lead to degenerative changes that may become painful, and rigid curves in osteopenic adults are difficult to treat surgically.
Surgical Intervention. Operative interventions vary with the number, location, and size of curves and the child's
skeletal maturity. For the typical right thoracic curve of 40-50 degrees in a skeletally immature female, a posterior spine fusion often is recommended. For thoracolumbar or lumbar curves, anterior fusion may offer an advantage of reducing the number of levels fused.
Anterior-posterior fusions are often needed for severe curves over 60-70 degrees, for rigid curves (do not improve to less than 50 degrees in bending), and for skeletally immature children who are at risk for crankshaft deformity (282). However, the use of new and stronger pedicle screws may allow the anterior portion of the fusion to be deferred.
In symptomatic adults with untreated idiopathic scoliosis, anterior-posterior fusions can be required for correction, with possible spinal cord decompression taking place as well.Neuromuscular Scoliosis
Curve Types. Scoliosis in neuromuscular disease is common. These curves occur with quadraplegic cerebral palsy (up to 70%), muscular dystrophy, or quadraplegic spinal cord injury (up to 90%); are long and sweeping; begin early; and progress quickly, affecting pelvic symmetry. They are fairly unresponsive to bracing, and may require extensive fusions to slow progression (282,293). Young, nonambulatory patients with thoracolumbar curves are at greatest risk for curve progression. A comparison of the surgical hospitalizations of children with neuromuscular scoliosis to those with idiopathic curves shows their stays to be longer, more complicated, and more costly (294). These children often have neurological, pulmonary, cardiac, or gastrointestinal comorbidities that affect their ability to wear spinal orthosis or undergo surgery, so careful surveillance of curve progression is important.
In children with myelomeingocoele, rapid progression of scoliosis may be indicative of a tethered cord, worsening hydrocephalus, or hydromyelia. In children with neurofibromatosis, intraspinal tumors may have developed. In both instance, MRI versus radiographs should be obtained.
Nonsurgical Management. Orthosis are often utilized in idiopathic curves of less than 40 degrees to delay progression. However, in neuromuscular scoliosis, while orthoses may improve trunk control and sitting posture, they less often slow curve progression and do not prevent the need for surgical intervention (293). Medical conditions such as rib cage deformity, pulmonary disease, gastroesophageal reflux, or insensate skin may make brace wear difficult, and the presence of coexisting feeding tubes, intrathecal baclofen pumps, or vagal nerve stimulators may complicate fit even further.
Orthotic wear is often abandoned unless it is useful for sitting support, for improving head position, or for stabilizing a flexible thoracic kyphosis. Often, a soft foam orthosis rather than one of rigid orthoplast, will be more tolerable to the patient, have less adverse impact on pulmonary function, and yet still provide adequate positioning support (295,296). The benefits versus disadvantages need to be fully explained to families before these expensive custom braces are fabricated.
Spasticity is a common issue in many children with cerebral palsy and neurologic impairment, and the use of peripheral botulinum toxin injections and intrathecal baclofen are fairly commonplace for its treatment. For scoliosis, botulinum toxin injections in the concave-side paraspinals for counterparalysis in progressing curves have been reported (297). It may provide some short-term benefit in patients who are progressing rapidly and in whom surgery must be delayed for medical reasons, especially if bracing is done concurrently. Intrathecal baclofen therapy has not been noted to have a significant impact, either positively or negatively, on curve progression (298). Due to the entrance of the intrathecal catheter at the thoracolumbar junction, care needs to be taken when fusing the spine post-pump placement, or when inserting the intrathecal catheter after a fusion, to avoid complications such as disruption of the catheter, infection, or a dural leak (299).
Surgical Intervention. Surgical interventions for neuromuscular curves differ from those of idiopathic curves due to their continued progression after maturity, the likelihood of concurrent pelvic obliquity, the osteopenic bone that must support instrumentation, and the length of the curves that are often present. Sublaminar wires, pedicle screws, and hooks are often used to provide segmentally stability, although Luque- Galvaston rods may be used for large curves or when pelvic obliquity is present (288,300). Lengthier fusions that extend from T2 to the pelvis are common in nonambulatory patients, although pelvic stabilization is avoided if possible in ambulators to reduce problems related to limiting lordosis.
Posterior fusions are preferred, as this bone is more stable and there is more difficulty accessing the anterior spine because of the diaphragm. Anterior fusions also produce sympathectomies and are associated with superior mesenteric artery syndrome (285). Anterior-posterior fusions are often done for severe curves (>60 degrees), although this may involve a two-stage procedure and may not improve correction that significantly. While safe, effective, and at times necessary due to a patient's medical stability or surgeon's skill, staging can increase cost and length of hospital stay (301).As neuromuscular curves over 50 degrees may continue to progress at a rate of 1.5 degrees per year even after maturity, the long-term advantages of early surgical intervention need to be discussed so that valid anticipatory guidance can be given (282). Advancing age, reduced bone quality, more rigid curve, limited respiratory reserve, and impaired skin integrity can adversely affect outcome. Functional goals of maintaining sitting tolerance, cosmesis, transfer capabilities, pulmonary and gastrointestinal function, and skin integrity are typical long-term concerns that should be considered.
In children with spina bifida, partial or complete vertebral body resections or fusions may be necessary to achieve stability (282). Children with Marfan's syndrome and Freidrich's ataxia, often have curves that are shorter and can be treated as though they were idiopathic curves (282). Achondroplasia may result in thoracolumbar kyphosis, lumbar stenosis, and lordosis. When these children experience pain or neurologic deficit, decompression and fusion is often necessary (282).
In children with Duchenne's muscular dystrophy, scoliosis is often relentless and progresses at up to 8 degrees per year. The use of oral steroids such as deflazacort to slow the decline in muscle strength and delay nonambulatory status can significantly attenuate the development of scoliosis and need for spinal surgery (300). Surgical intervention needs to be timed to maximize pulmonary status (FVC >35%) and curves of 20-30 degrees are often corrected in order to improve seating and respiratory function early on (282,302). The increased risk of anesthesia-induced malignant hyperthermia needs to be recognized in this population.
Preoperative nutritional and health optimization and perioperative infection and pain control are important to successful spinal surgery. Postoperative nutritional supplementation, pressure sore vigilance, pulmonary toilet, gastrointestinal motility, aspiration prevention, and rapid upright sitting posture and mobility to prevent deep venous thrombosis are needed. These issues as well as adequate discharge planning need to be addressed proactively by both the physiatrist and the surgeon in order to achieve best outcomes.
Despite the challenges of surgical correction in children with neuromuscular scoliosis, studies show that curve degree, lung function, seating position, and activities of daily living may all improve postopera- tively, potentially improving quality of life and caregiving abilities (280).