INTRAUTERINE GROWTH RETARDATION
The term intrauterine growth retardation (IUGR) or small for date (SFD) or Small for gestational age (SGA) is reserved for those LBW babies, who are born fullterm
TABLE 12.28: Causes of IUGR (small for date LBW)
• Maternal factors (poor nutrition/chronic hypoxia)
- Age lt;20 or gt;35 years
- Parity: Primipara or grand-multipara
- Undernutrition or poor weight gain in pregnancy
- Anemia
- Chronic cardiac or pulmonary disease
- Abuse: Drugs, alcohol, smoking
• Placental factors (F uteroplacental blood flow)
- Structural abnormalities
- Abruptio placentae
- Vascular infarcts: Hypertension, pre-eclampsia
- Multiple gestations (twin-twin transfusion)
• Fetal factors (F growth potential)
- Chromosomal/genetic disorders, e.g.
trisomies- Dysmorphic syndromes/congenital anomalies
- Intrauterine infections
- Metabolic: Insulin/insulin-like growth factor deficiency
• Idiopathic
or preterm, with birth weight 2 SD or 10th percentile for their gestation, thus excluding preterm-AGA.
Causes: Fetal growth depends on adequate transplacental supply of nutrients and oxygen from mother as well as on its inherent growth potential. Consequently, IUGR may be caused by:
• Maternal malnutrition or chronic hypoxic states, e.g. anemia, cardiopulmonary diseases, etc.
• Decreased placental blood flow due to placental abnormalities, or
• Decreased fetal growth potential, e.g. intrauterine infections or chromosomal disorders.
Maternal malnutrition, anemia and intrauterine infections are three leading causes of IUGR in India (Table 12.28).
Clinical features: Clinical features of IUGR babies vary according to the timing of intrauterine insult and may be divided into 3 categories:
a. Symmetrical IUGR (hypoplastic SFD), due to fetal insult in first trimester, before organogenesis is complete.
All growth parameters, e.g. weight, length and head circumference are proportionately affected in these babies, giving them a tiny appearance and high ponderal index gt;2. For ponderal index calculation, see footnote of Table 12.33.b. Asymmetrical IUGR (malnourished SFD), due to fetal insult in late gestation. As fetal weight is disproportionately more affected than length or head circumference, these babies have a marasmic appearance with low ponderal index lt;2.
c. Mixed SFD, with adverse intrauterine factors operative throughout the gestation.
Diagnosis of IUGR may be suspected antenatally on the basis of: (a) discrepancy between gestational age by history and fundal height, and (b) USG findings, e.g. low
TABLE 12.29: D/D asymmetrical vs symmetrical IUGR
*Ponderal Index: Weight in gm/length in cm3 ? 100
BPD for gestation (lt;8.5 cm at 37 weeks), or fetal headthorax or head-abdomen ratio. Important differences between asymmetric and symmetric IUGR are given in Table 12.29.
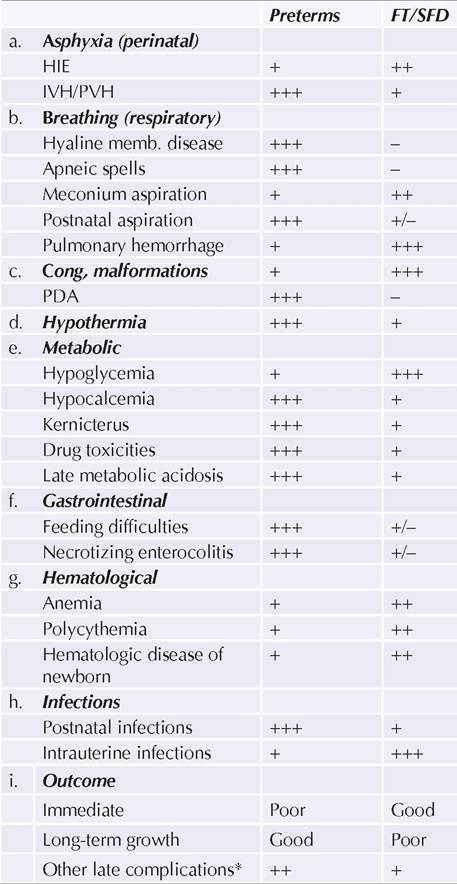
Complications: FT/SFD are physiologically as mature as normal term newborns and complications related to prematurity are uncommon despite low birth weight. However, these babies are more prone for (a) perinatal asphyxia due to placental dysfunction, (b) hypoglycemia due to poor stores, (c) congenital malformations due to intrauterine infections, (d) hypothermia due to scanty body fat, (e) poor growth potential in long-term.
PT-SFDs have additional risk of complications related to prematurity as enumerated in Table 12.27, which also summarizes important difference between complications in fullterm and preterm LBWs.
Management of IUGR is similar to that of preterms, as discussed in previous chapter, with following special considerations:
• Delivery room care—as IUGR babies are more prone for intrauterine asphyxia, regular fetal monitoring with emergency LSCS facility and neonatal resuscitation should be available.
• As these babies are prone for hypoglycemia, early breastfeeding should be ensured, with periodic glucose monitoring.
• Congenital malformations and stigmata of intrauterine infections should be carefully looked in FT-SFD cases.
• Polycythemia, if symptomatic, should be managed by partial exchange with plasma.
Outcome: Chances of immediate survival are better in FT-SFD babies than in preterms. However, growth potential is often reduced in them and unlike preterms, SFDs do not show catch-up growth, ultimately ending with short-stature.
12.11.3