PREMATURITY (PRETERM-LBW)
Prematurity is defined as a live birth before the completion of 37th week of gestation (up to 36 weeks and 6 days). Live births before 28th week are generally referred as extreme prematurity.
Causes: Preterm labor may be spontaneous due to various maternal and fetal factors or induced on medical grounds (Table 12.21). Many spontaneous preterm labors are preventable by timely medical care.
TABLE 12.21: Causes of prematurity
• Maternal ill health
- Chronic systemic diseases
- Severe anemia
- Infections of genitourinary tract
• Uterine abnormality
- Incompetent cervix
- Bi-cornuate uterus
• Obstetric complications
- Twin pregnancy
- Antepartum hemorrhage, placenta previa
- PolyVoligohydramnios
- Premature rupture of membranes
• Fetal factors
- Fetal hypoxia and distress
- Hydrops fetalis
- Serious congenital malformations
• Idiopathic
Fig. 12.10: Fetal Growth Chart: Estimated fetal weight percentiles at different gestational ages (WHO).

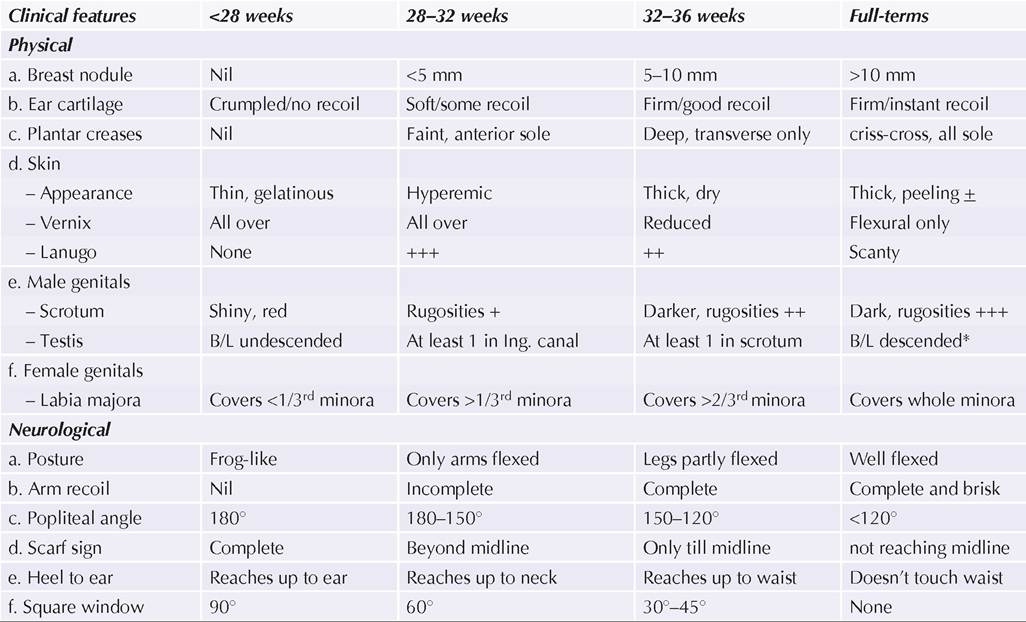
TABLE 12.22: Common clinical and neurological features at different gestational ages

Clinical attributes of prematurity vary with gestational age (Table 12.22), though some important indicators are as follows:
• Physical features in preterms include:
- Skin is shiny, hyperemic, covered with plenty of vernix caseosa (a whitish greasy substance to prevent hypothermia) and Lanugo (soft-fuzzy hair on back and limbs). Pedal edema is common in extreme preterms.
- Sole creases are absent or poorly developed, seen in only some parts of soles.
- Ear cartilage is poorly formed and shows slower recoil, when crumpled. Eyes are tightly closed in extreme preterms.
- Breast nodule, felt as an induration by rolling-over between fingers, is poorly developed.
- Genitals: In male preterms, scrotum is shiny and less pigmented with poorly developed scrotal rugosities and undescended or partially descended testis. In female preterms, labia majora is widely separated to covers only a part of labia minora. In fullterms, labia minora is almost invisible.
• Neurological features in preterms include:
- Posture: Preterms have a prominent head lag and stay in a pithed-frog posture with extended limbs due to marked hypotonia, as against the fully-flexed fetal posture in fullterm.
- Hypotonia is a prominent feature in preterms, as evident by their posture as well as when tested for active tone (poor arm recoil) and passive tone (popliteal angle, Scarf sign or heel to ear maneuver).
#9632; Popliteal angle is measured behind the knee on complete flexion at hip and maximum extension at knee.
#9632; Scarf sign is tested by adducting one upper arm towards opposite shoulder and checking the position of elbow on full adduction.
#9632; Heel to ear maneuver involves an attempt to touch the ear with baby's heel and see its maximum possible reach.
- Immature joint mobility, as indicated by Square window sign. Square window is the angle formed at wrist after complete flexion to touch the forearm with fingers.
- Immature neonatal reflexes, which appear gradually with advancing gestation (Table 12.12).
Assessment of gestation age depends on—(a) date of last menstrual period, (b) antenatal records, e.g. fundal height and USG, and (c) physical and neurological features of newborn. Birth weight is not a reliable criteria for diagnosis of prematurity, as it does not exclude SFD/ IUGR babies.
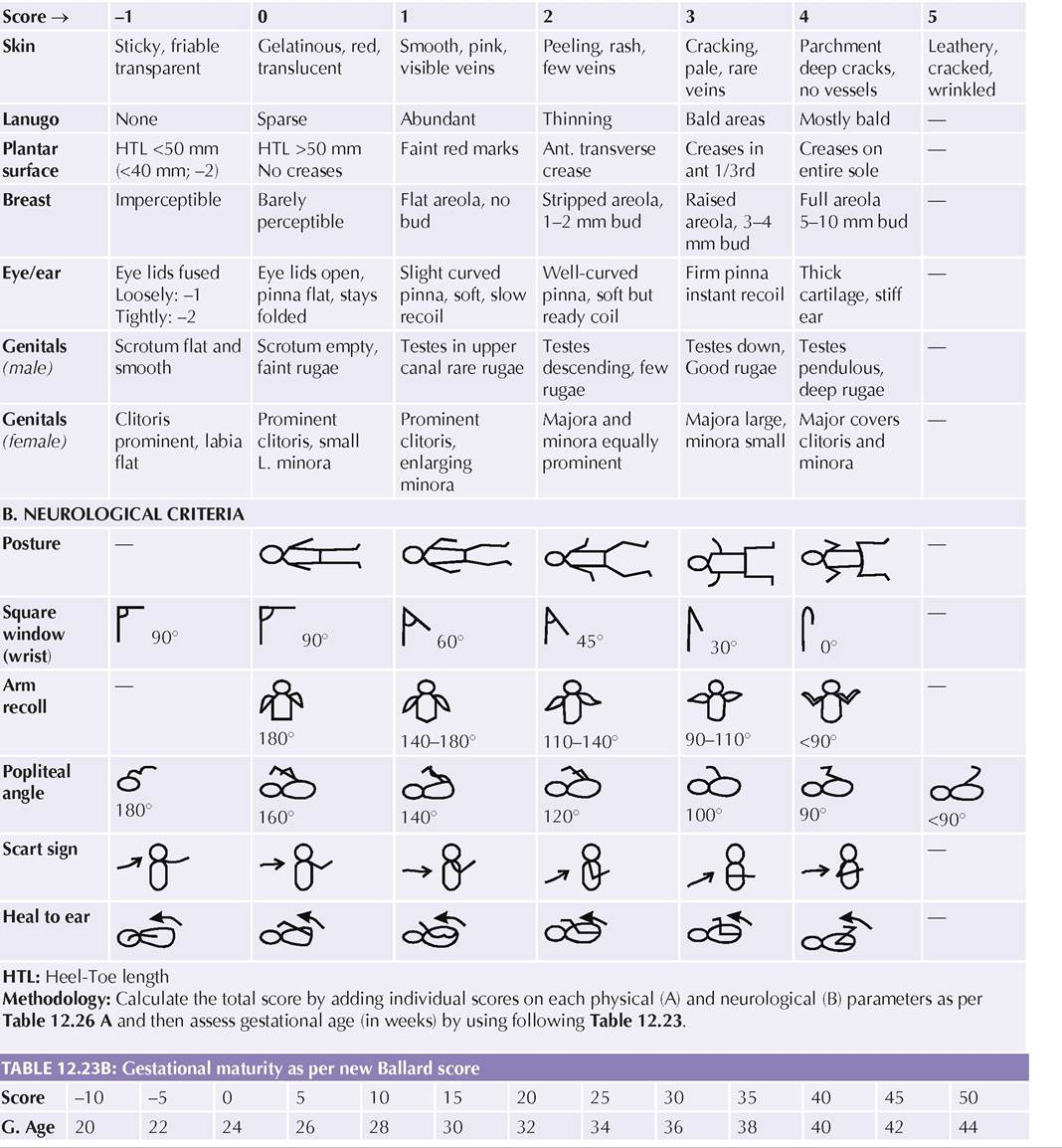
Various scoring systems, based on physical and neurological features, e.g. Dubowitz criteria or Ballard scoring (Table 12.23) are available for precise postnatal assessment of gestation age.
TABLE 12.23A: Modified Ballard scoring system for assessment of gestational age
A.
PHYSICAL CRITERIA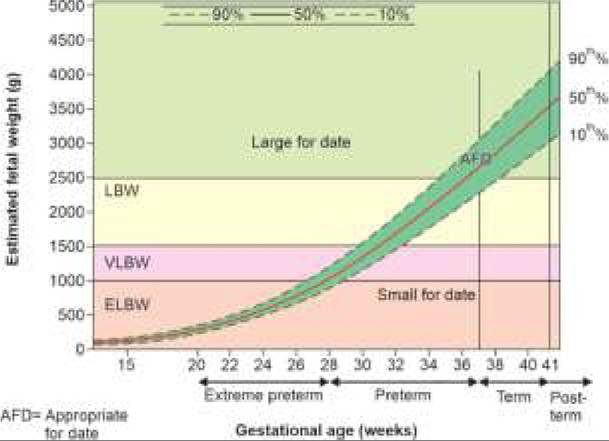
Physiological handicaps and complications: A premature child has many physiological immaturities or handicaps, rendering him susceptible for many complications in immediate postnatal or later life (Table 12.24). Important handicaps include:
Thermoregulation immaturity (hypothermia) due to-(a) excessive heat loss via larger surface area and thin skin, and (b) poor heat production due to less brown fat. Respiratory immaturity with poor-(a) central control (apneic spells), (b) cough-reflex (aspiration pneumonia),
| 324 | Textbook of Pediatrics |
TABLE 12.24: Complications of prematurity and LBW

*e.g. Cerebial palsy, mental retardation, retinopathy of prematurity, broncho-pulmonary dysplasia
IVH/PVH: IntraventricularZperiventricular hemorrhage,
HIE: Hypoxic-ischemic encephalopathy
(c) ventilatory efforts due to highly compliant chest wall, (d) alveolar expansion due to surfactant deficiency (hyaline membrane disease), (e) alveolar diffusion due to cuboidal epithelium, and (f) perfusion due to trans-PDA shunting.
• Circulatory immaturity with—(a) delayed closure of ductus arteriosus (PDA), (b) increased vascular permeability, and (c) immature autoregulation of cerebral blood flow (IVH/PVH).
• Neurological immaturity with—(a) generalized hypotonia/hyporeflexia, (b) immature germinal matrix (IVH/PVH), and (c) impaired blood-brain barrier (Kernicterus). However, hypoxia is better tolerated by preterms than term babies.
• GIT immaturity with poor—(a) sucking/swallowing reflexes (feeding difficulties), (b) palato-pharyngeal competence (recurrent aspiration), (c) esophageal sphincter competence (gastroesophageal ref lux),
(d) gastric volume (inability to tolerate large feeds),
(e) digestive enzymes, e.g.
lipase, trypsin and lactase, activity (digestive/absorptive problems), and (f) intestinal motility and stasis (gut infections).• Hepatic immaturity with poor—(a) glucuronyl transferase activity (hyperbilirubinemia), (b) nutrient metabolic activity (hypoglycemia, hypoproteinemia), and (c) drug metabolism (increased risk of toxicity).
• Renal immaturity with poor—(a) glomerular filtration rate (solute overload, drug toxicity), (b) urinary concentration (dehydration), (c) sodium conservation (hyponatremia), and (d) acidification capacity (late metabolic acidosis).
• Immunological incompetence (infections) due to—(a) low IgG levels via maternal transfer, (b) low secretary IGA, phagocytic, complement activity, and (c) impaired cell-mediated immunity.
• Hematological immaturities with—(a) poor iron stores (apnea of prematurity), (b) deficiency of clotting factors (bleeding tendencies).
• Nutritional problems due to—(a) poor stores (hypoglycemia, hypocalcemia), (b) higher requirements due to higher surface area, tissue turnover, catch-up growth, etc. and (c) poor intake.
• Endocrinal immaturity, e.g. transient hypoparathyroidism (osteopenia of prematurity).
Management of a preterm child begins before birth, including—(a) delaying elective preterm deliveries as long as possible, and (b) referral to well-equipped centers, (c) antenatal steroids, to enhance lung maturity. All preterm deliveries should be attended by trained neonatologist and delayed clamping of cord helps not only to improve iron stores but also to reduce the risk of intraventricular hemorrhage and other morbidities.
While Borderline preterms may be managed as term babies, postnatal management of a preterm baby depends on the gestational age, birth weight and presence of complications. While borderline preterms can be managed as term babies only, most babies weighing lt; 2000 gm or 34 weeks of gestation need careful consideration for physiological handicaps and potential complications.
Important steps include:a. Intensive care: All preterms lt;1500 gm, lt;32 weeks or with complications, e.g. infections or congenital malformations, need to be hospitalized in level-III NICU. More mature babies without major problems may be managed in level-II nursery, provided constant monitoring is possible.
b. Thermoregulation is the most important determinant for survival during first 24 hours. All preterm babies should be prevented from hypothermia by appropriate
measures, depending on their clinical gestation and clinical status, as follows:
- Kangaroo mother care (KMC) be initiated immediately after birth in babies in all borderline preterms/LBWs, weighing gt;1800 gm, provides they are otherwise stable and have no other complications. Proper 2-3 layer clothing including mittens and cap is required during intervening period.
- Warmer-care is usually required in babies lt; 1800 gm as well as all sick/unstable LBWs, providing a thermoneutral environment to minimize oxygen and metabolic requirements. Ideal thermoneutral environment varies with gestational age, though ~33-35°C is adequate for most preterms (Ch 12.12). However, most of them, specially those between 1200-1800 gm can also be shifted to KMC after few days of observation and stabilization.
- Temperature control is also necessary during transfer of these babies from delivery room to NICU as well as during investigations and blood sample collections.
- Body temperature must be monitored frequently in all preterms, using an axillary digital thermometer, at least 2-4 hourly on the first day of life.
- Relative humidity must be maintained at 40-60% to prevent drying of airways, thickening of secretions and insensible water loss from the lungs.
c. Nursing position: It is preferable to keep these babies in prone position (except immediately after feeding and when sick) to facilitate drainage of oropharyngeal secretions (prevents aspiration), passage of flatus (less abdominal distension) and lesser effort for ventilation.
However, many workers advise supine position for ease of clinical supervision.d. Nutrition: Quantity and mode of feeding is an important issue in preterm care due to—(a) higher nutritional requirements, and (b) physiological immaturity in sucking, swallowing, digestion and absorption of feeds.
Nutritional requirements of these babies vary with gestation, weight, nursing environment and associated complications, as follows:
- Higher fluid requirements (Table 12.25) due to high basal metabolic rate well as excessive losses via
TABLE 12.25: Fluids requirement (ml/kg) in preterm/LBW
Day of life gt;1500 1000-1500 lt;1000
| 1st | 60 | 80 | 100 |
| 3rd | 90 | 110 | 130 |
| 5th | 120 | 140 | 160 |
| 7th | 150 | 170 | 190 |
Simple thumb rules:
• Fluid needs in 3 weight categories differ by 20 ml.
• Daily requirements in each category increase by 15 ml/day
Add 20 and 40 ml/kg for babies under phototherapy and warmers respectively
kidney (physiological diuresis), GIT (physiological diarrhea), lungs (physiological tachypnea) and skin (large surface area).
- Higher energy requirements coupled with inability to accept large volume feeds. Preterm feeds should provide ~130 cal/kg with higher caloric density of ~70 cal/100 ml.
- Higher protein requirements due to increased tissue synthesis and immature metabolism of essential amino acids. Consequently, preterm-feeds should provide ~ 2.5-3.0 gm/kg proteins, with whey:casein ratio of 60:40 (as in breast milk), and all essential amino acids in appropriate amounts.
- Low lactose/starch digestibility, due to physiological lactase/ amylase deficiency. Carbohydrates should not exceed 40-50% of preterm feed, of which at least 50% should be as glucose polymers, e.g. maltodextrin, polycose.
- Poorfat digestibility/absorption, due to physiological deficiency of pancreatic lipase and bile salts. Medium chain triglycerides, e.g. coconut oil, which are directly absorbed in portal circulation without micelles formation, are better tolerated in preterms. As essential fatty acid deficiency is common in preterms, 1% of total energy should be provided by linoleic acid.
- Higher sodium requirements due to inadequate renal conservation capacity. A preterm feed should provide ~2.5-3.5 mEq/kg/d of sodium (4-8 mEq/ kg in VLBWs).
- Micronutrient supplementation (Table 12.26) is necessary due to poor stores and higher requirements. However, iron supplements should be delayed till ~2-4 weeks, due to potential risk of hemolytic anemia (competitive vitamin E deficiency) and pathogenic diarrhea (iron binds lactoferrin-an inhibitor of E. coli growth).
While the precise mode of feeding depends on the acceptability by the baby, following general guidelines may be used for initial feeding decisions in different categories of preterms (Table 12.27):
*From 2 weeks onwards, except vitamin K (from birth)
**In VLBWs only, till 36 weeks maturity is reached
***After full enteral feeding established, not later than 8 weeks
TABLE 12.27: Modes of feeding in preterms/LBW
Birth weight (gm)
Kamp;S: Katori and spoon, BF: Breastfeeding
Uncomplicated preterms gt;1800 gm or gt;32 weeks usually accept breastfeeds and may be fed directly or via bondla/spoon by mothers.
Preterm milk is qualitatively different from termmilk on following counts-Low caloric density (51 vs. 67), high proteins (2.2 vs. 1.1 gm), low lactose (6.0 vs. 7.0 gm), low fat (1.6 vs. 3.5 gm), high sodium (2.6 vs. 0.7 gm) and high Ca/P ratio (20/10 vs. 34/15 mg). (All values/100 ml milk, composition changes with gestation)
Uncomplicated preterms 1200-1800gm or 28-31 weeks usually require intragastric feeding of expressed breast milk (EBM) for first few days, followed by Bondla/spoon feeding or direct breastfeeds, as soon as acceptable.
It is advisable to begin with 60-80 ml/kg/d of EBM on first day (on lower side in better weight babies and increase by 15 ml/kg every day till ~150 ml/kg/d is reached. Volume of each feed may be calculated by dividing the total daily requirement with number of feeds.
Position of nasogastric tube should be checked before feeding, as also the amount of pre-feed aspirate, which should not exceed gt;1/3rd of previous feed. Increased pre-feed suggests poor gastric emptying— an early indicator of necrotising enterocolitis, intestinal obstruction or paralytic ileus.
Human milk fortifiers (HMF) are natural or commercial substances, used to improve energy content of EBM without significant volume load. These include vegetable oils, e.g. coconut oil or safflower oil (2-3 drops/20 ml feed) and commercial preparations (~ 2 cal/gm; 1 gm/10 ml feed). HMF may be used in uncomplicated infants lt; 1800 gm, after 1st week, to enhance caloric density of EBM.
Complicated or extreme preterms (lt;1200 gm or lt; 28 weeks) usually need parenteral nutrition for first 48-72 hours, provided as 60-80 ml/kg of 5% dextrose, higher side in lighter babies. Sodium and potassium must be added in IV fluid after 48 hours. Fluid requirements increase with increasing age as 10-15/ml/kg/day, to a maximum of 150 ml/kg/day after the first week.
While most preterms can be gradually switched on oral feeds, those who need parenteral nutrition for more than one week, must be considered for total parenteral nutrition (Ch 27.4.5).
Non-nutritive sucking or trial breastfeeding is advised to all babies on parenteral or nasogastric feeding, to promote lactation and emotional bonding. While the breast milk from own mother is best and gestation-specific for preterms, breast milk from milk-bank or other mothers may be used in cases with maternal death/serious illness. If it is inevitable to use top milk, only a preterm-specific formula milk must be used rather than term-milk formulas or animal-milk, to avoid solute overload and other complications.
e. Monitoring: All preterms should be constantly monitored for adequacy of feeding, weight gain and danger signals and IV sites. Non-invasive devices, e.g. apnea alarms and pulse oximeter are frequently used to monitor extreme/complicated preterms.
All babies in hospital must be weighed daily to assess adequacy of nutrition. Preterm babies loose ~15% of birth weight in first week (vs 10% loss in terms) and regain it by 10th-14th day (7-10 days in terms), followed by gaining ~15-20 gm/day, even 20-40 gm/day as they approach near term (catchup growth). Fenton charts may be used to monitor infant's growth in preterms till they reach 50 weeks of gestational age.
f. Prevention of nosocomial infections requires: (a) restricted-entry in nursery, (b) minimal handling, (c) proper hand-washing, (d) ensuring asepsis during diagnostic/therapeutic interventions, and (e) early detection/treatment infections. Prophylactic antibiotics are not necessary in preterms, except those with other risk factors.
g. Discharge criteria for preterms include: (a) weight gt;1800 gm with steady gain, (b) absence of complications or need for parenteral medications, (c) adequate feeding with acceptance of direct breastfeeding or EBM with Bondla/spoon, (d) Complete age- appropriate immunization, (e) Adequate maternal counseling for general baby care, thermo-care, feeding and follow-up.
It is advisable to keep mother and baby in intermediate care or regular postnatal ward for a few days after discharge from NICU, to ensure baby's well-being.
Outcome of prematurity depends on its severity and presence of complications. With therapeutic advances, even babies as young as 22 weeks (gt;500 gm) are salvageable. However, survival of extreme preterms has also increased the risk of late sequelae in these babies and Follow-up of all preterms is necessary at periodic intervals till at least one year, to assess catch-up growth and identify late sequelae.
12.11.2