Level of Injury-ASIA Impairment Scale
The most common method of classifying impairment from SCI is the American Spinal Injury Association (ASIA) impairment scale. The classification is based upon assessment of strength and sensation to light touch and pinprick in defined myotomes and dermatomes.
Key muscle groups and sensory points are shown in Figure 11.1. The ASIA impairment scale has been modified over the years, originally based on the classification system defined by Frankel. Completing the ASIA examination on a child requires a certain level of maturity in being able to follow motor commands and respond appropriately to sensory stimulation. The examiner must take this into account when assessing children. Other factors that may limit examination (eg, long bone fractures or decreased level of consciousness) need to be taken into account as well.The motor examination scores strength on a six- point scale: 0-5. For each strength grade, the joint being assessed must be moved through full available range of motion. A strength grade of 0 is given for total paralysis. A 1 is given for a visible or palpable contraction that cannot move the joint through its available range of motion with gravity removed. A grade 2 is given if the muscle group can move the joint through its range of motion with gravity removed. The joint is positioned parallel to the ground to limit the effect of gravity. A grade 3 is given when the patient can move the joint through full available range of motion against gravity but cannot bear any additional resistance. If a patient can bear additional resistance, they are given a grade 4, and a grade 5 is given for normal strength. Motor scores are documented on the ASIA form and summed for a total motor score. A rectal exam must be performed to assess for voluntary contraction, and is scored as yes/ no. As individual muscles are almost always innervated by multiple spinal cord levels, a strength grade of 3 is considered normal for a muscle group if the level above has grade 5 strength. This implies that the grade 3 muscle group is only partially innervated and the more proximal innervation level is intact.
STANDARD NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY
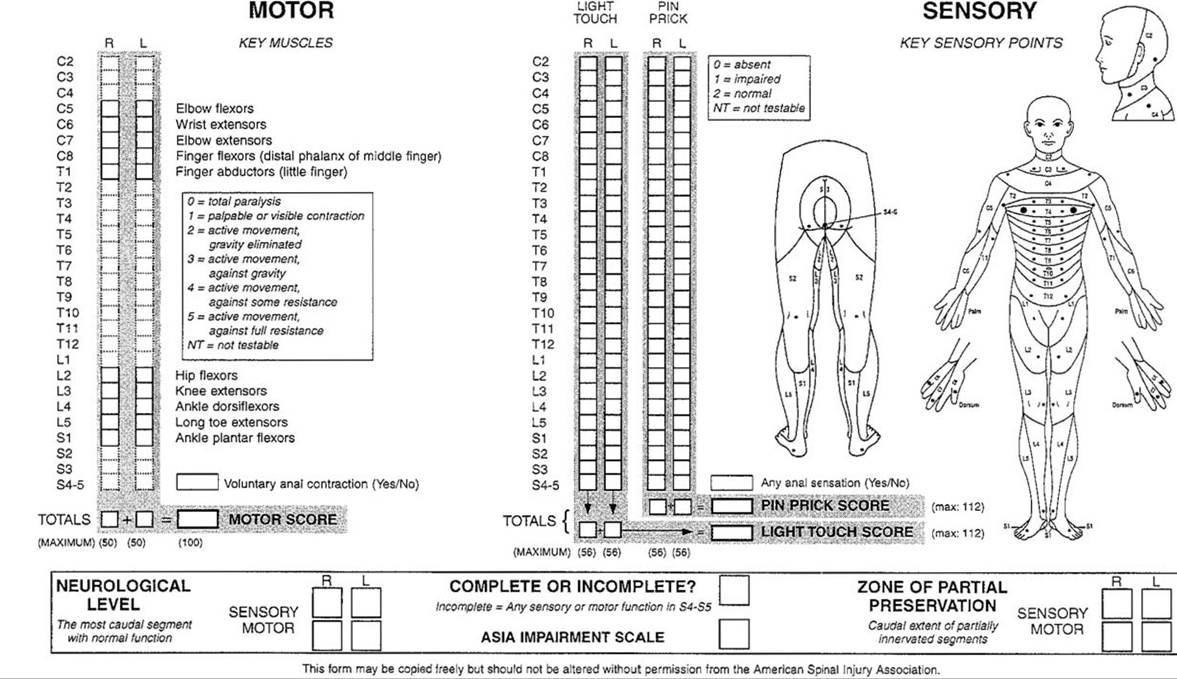
Figure 11.1 American Spinal Injury Association guide.
Sensory examination is performed using pinprick and light touch at key points, and grades as 0 for absent, 1 for impaired, and 2 for normal.
These results are summed as well for total light touch and pinprick scores. Again, a rectal exam is necessary to assess anal sensation, also scored yes/no.The ASIA neurologic level is the most caudal segment with intact motor and sensory exam. In addition to the level is whether the injury is complete or incomplete. With a complete injury, there is no motor or sensory function in the lowest sacral segment (ie, no anal sensation or voluntary anal contraction). A complete injury is classified as ASIA-A. Incomplete injuries are classified as B-E, as listed in Figure 11.1. While an “E” is described as normal sensory and motor function, this is in the context of a previously abnormal examination.
Paraplegia affects the lower extremities and, to varying degrees, the trunk. It does not affect the upper extremities; thus, T2 must be normal and any deficits are below that sensory and motor level. The preferred term from ASIA for involvement of all four extremities is tetraplegia, though quadriplegia is much more commonly used. Any injury that affects motor and/ or sensation at or above the T2 level is tetraplegia. In addition, a number of syndromes have been described based upon the patterns seen after specific areas of the spinal cord have been injured.
More on the topic Level of Injury-ASIA Impairment Scale:
- Immersion Injury (Trench Foot)
- The historical record: how traditional is local government in Asia?
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY