LIFESPAN PERSPECTIVE
Improved medical care, increased life expectancy, and better services for lifelong care and support in society have provoked an interest and need for long-term future planning. This includes transitions in care from typical nurturing pediatric care systems to more traditional adult self-directed services.
Retrospective reviews and anecdotal experiences also question some long-held beliefs of “use it or lose it” to one of “conserve it to preserve it (7).” Choice of health care providers for adults with early-onset disabilities and special health care needs is often limited by insurance and expertise.Clinicians with an understanding of the natural history of disabling conditions can be helpful in monitoring and keeping vigilance for and prevention of some general health conditions and aging or secondary conditions seen in disability. This public health model of prevention also includes tertiary prevention with the use of environmental modifications and technologies and removal of barriers to participation. There are general aging, associated conditions, secondary conditions, and health concepts that are helpful in understanding a lifespan perspective.
Aging is a developmental process. It begins at birth and continues to death. Typically, however, children and adolescents are said to develop, whereas adults, especially adults over 50 or 60, are said to age. During the early stages of aging (infancy, childhood, adolescence), attainment of skills and capabilities is on the rise; in the middle stages (adulthood), maintaining and retaining function is the focus. Over a normal lifespan, natural physiological declines are not truly preventable, although they may be accelerated or slowed by a variety of individual genetic factors, personal behaviors (eg, diet and exercise), health care practices, and environmental conditions. Aging changes in motor performance seem to be accelerated in some adults with early-onset disabilities, with earlier-than-typical manifestation of slowed or decreased motor performance and pain complaints.
Persons with disabilities follow a course of aging, although likely with a slower and lower attainment of skills and a smaller capacity to adjust to acute or intercurrent health or medical and surgical intercedents (Fig. 15.1). So the emphasis here is on aging with a disability, not aging into disability.There is also a need to appreciate the different time dimensions at play, as noted by Campbell (8) and
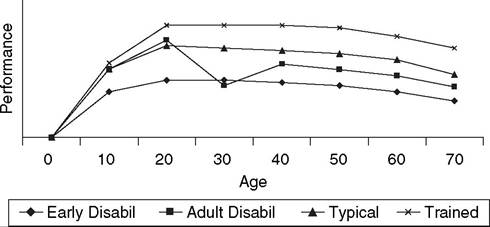
Figure 15.1 Conceptual model of aging and performance. Performance is a conceptual quotient of multiple skills. The trained person will achieve a higher level of performance than typical and, assuming ongoing exercise, will have a slower decline with age. With the onset of disability in adult years, there is loss of skill then improvement, but often not achieving the previous typical level. Those with early- onset disabilities do not achieve full “performance” and are slower to achieve the maximum level.
Krause and Adkins (7). These include the typical aging process, as noted previously, age of onset of disability in relation to developmental maturity (congenital onset versus adolescent onset), the number of years spent with a disability (hemiparesis onset at age 5 years versus age 17 years), cumulative effects of medications or treatments (long-term steroid use), and era of disability onset (cerebral palsy onset in 1950s versus 1990s, including different treatments, opportunities, and attitudes). Anticipated aging changes and treatment strategies will be modified by these temporal concepts.
Secondary conditions are defined as “any additional physical or mental health condition that occurs as a result of having a primary disabling condition (2,9).” The initial concept (10) and intended use (11) distinguishes secondary health conditions from the social and economic consequences that may follow a primary disabling condition (societal limitations and barriers—for example, poverty with disability, social isolation, limited transportation). There are key common features of secondary conditions (9):
■ Causal relationship to the primary disability—the primary disability is a risk factor for the secondary condition
■ Preventable or modifiable conditions
■ Variability in expression and timing of manifestation
■ Capability to increase the severity of the primary condition
■ Potential to become the primary health concern
Many secondary conditions are linked across several primary disabling conditions through common physiologic processes or functional characteristics.
As an example, disabilities with sensation changes and immobility are risk factors for pressure ulcers, such as spinal cord injury, spina bifida, multiple sclerosis, and severe brain injury. Three common secondary conditions noted through cross-disability studies are fatigue, chronic pain, and depression (1,12-14).Secondary conditions are distinct from associated conditions or residual deficits and comorbidities. Associated conditions describe elements that result from the defect, injury, disease, or pathology, although the expression may be variable. These conditions are the residual from the original pathology, and are often present at the time of diagnosis of the primary disability, although by development or evolution may not be expressed or expressed fully at initial diagnosis. For cerebral palsy or other brain injuries, the list of associated conditions includes seizures, spasticity, learning disabilities, intellectual disability, sensory problems, and oral motor and communication problems. These conditions may not be present for all people with the specific disability, are fairly well known to require monitoring by clinicians, and their presence is confirmed through typical timely evaluation. Persons with a primary disabling condition may have any combination of associated conditions, all of which will affect their ultimate functional capabilities. Comorbidities are other medical conditions unrelated to the primary disabling condition, and not a feature of the primary disability. As an example, persons with cerebral palsy may also develop diabetes mellitus or colon cancer should they have the risk factors or genetic predisposition for these conditions. As research continues, especially through longitudinal studies, links may be identified between primary disabilities and specific health conditions.
Health is a concept only recently considered to be an important goal for people with disabilities, and is the absence of disease or illness, beyond the disabling condition.
Health perception is an individual determination, and is affected by personal expectations, experiences, sense of vulnerability, support, and locale. How people with disabilities self-rate their health has been in question (15). This self-concept may also direct consideration of engagement in typical health and wellness activities. Often, the health of persons with disabilities is perceived as poor by clinicians and providers when individuals report a positive perception of their own health. This health provider concept may limit the offer of screening or health promotion opportunities. Perception of health in adults with disabilities may be related to time of onset, with report that adults with early-onset disabilities may identify better health than those with adult-onset disabilities (16,17). Research further suggests that adults with disabilities likely have a different construct of and self-rating process for health (18). In general, persons with nonprogressive disabilities should be considered healthy, with a shift of the health care model from an illness and disability paradigm to one of wellness and prevention or early identification of secondary conditions, aging issues, and/or comorbidities.