MISCELLANEOUS LUNG DISORDERS
This chapter deals with some common acute or chronic lung disorders, not discussed elsewhere.
Atelectasis (collapse) denotes impaired expansion of alveoli with loss of lung volume, either due to absorption of alveolar air after airway obstruction or compression of alveoli by external pressure.
Etiologically, collapse may classified as:
• Obstructive collapse, due to intra-bronchial obstruction by foreign body, caseous material or mucus plugs, etc. or extra-bronchial obstruction by lymph node, tumors, etc.
• Pressure collapse, due to compression of lung parenchyma, e.g. in plural effusion, pneumothorax, diaphragmatic hernia, tumors, etc. Pressure collapse may also develop due to deformities of thoracic cage/spine.
Reduced surfactant production in preterm newborns is another cause of atelectsis in newborns or in some inhalant poisonings.
Clinical manifestations depend on the cause, severity and duration of collapse. While sudden collapse in previously normal lung may present with significant respiratory distress, long-standing collapse may be entirely asymptomatic.
Characteristic clinical signs include-(a) shift of trachea/mediastinum towards affected side, (b) dull percussion note, and (c) diminished air entry/vocal resonance. However, bronchial breathing with increased vocal resonance is common, if collapsed lung overlies a patent bronchus.
Diagnosis generally rests on chest skiagrams, showing: (a) tracheal shift on same side with overcrowding of ribs, and (b) homogeneous patchy or segmental opacity, with sharp and contracted borders (Fig. 16.17).
Right lower lobe collapse is most likely due to foreign body, while right middle lobe collapse is usually tubercular in origin following bronchial compression by mediastinal lymph nodes (middle lobe syndrome).

Fig.
16.17: Collapse of the lower zone in right lung.Bronchoscopy is essential in all cases of persistent collapse with unknown etiology or suspected foreign body.
Management includes: (a) bronchoscopic removal of obstructing material, e.g. foreign body or mucus plugs,
(b) chest physiotherapy with postural drainage and breathing exercises, (c) treatment of primary cause.
Persistent collapse for gt;4-6 weeks is unlikely to be reversible and becomes a nidus for chronic infection or bronchiectasis. Surgical resection, i.e. lobectomy or pneumonectomy, may be necessary in these cases to prevent development of bronchiectasis and further spread of infection.
Emphysema, i.e. distension of air spaces with irreversible disruption of alveolar septa may be localized or generalized. Mere distension of alveoli, without septal disruption, is called overinflation.
Etiology: Common causes of emphysema include:
• Partial airway obstruction (ball-valve mechanism) with expiratory air trapping by foreign body, mucus plugs or endobronchial tuberculosis.
• Compensatory emphysema, to overtake the function of diseased or surgically removed lung.
• Congenital lobar emphysema (CLE), either primary or due to secondary to bronchomalacia, bronchial stenosis/mucosal folds or aberrant vessels.
• Generalized air trapping and emphysema in asthma, cystic fibrosis, 1-antitypsin deficiency and interstitial lung diseases. Unilateral hyperlucency of lung following infections is termed as Swyer-James syndrome.
Clinically, emphysema is rarely symptomatic, except CLE that may present with respiratory distress in newborns or early infancy. Generalized emphysema may be associated with overinflation of chest and resonant percussion note.

Fig. 16.18: Emphysema: (A) Bilateral; (B) Segmental (Right lower zone)
Diagnosis rests on chest X-ray showing localized or diffuse hyperlucency (Fig.
16.18) but with visible bronchovesicular markings and no mediastinal shift (d/d pneumothorax). Treatment depends on primary cause. Congenital lobar emphysema may be associated with herniation of the lung across the mediastinum and needs lobectomy to prevent compression of other parts.Pulmonary edema denotes transudation or exudation of fluid from interstitial capillaries to alveolar space due to:
• Increased pulmonary vascular pressure, e.g. heart disease, left ventricular failure, etc.;
• Increased pulmonary blood volume, e.g. overhydration, renal failure;
• Decreased plasma oncotic pressure, e.g. nephritic syndrome, hypoproteinemia;
• Altered capillary permeability due to alveolar inflammation, e.g. acute respiratory distress syndrome (ARDS), etc.
• High altitude pulmonary edema, due to low atmospheric pressure.
Clinically, it presents with progressive dyspnea, wheezing and cough with frothy, pinkish expectoration.
Bilateral coarse, bubbly crepitations are common, specially in basal region.
Diagnosis rests on chest skiagram showing bilateral generalized haziness of lungs with/without Kerley's lines, i.e. linear streaks extending from hilum to periphery due to dilated lymphatics.
Presence of cardiomegaly, perihilar butterfly distribution of edema and Kerley's lines indicate cardiogenic pulmonary edema while normal heart size with peripheral/patchy distribution of edema and presence of air bronchogram suggests non-cardiogenic etiology (Fig. 16.19).
Treatment is directed to primary cause with diuretics, cardiotonic drugs, e.g. digoxin, and bronchodilators along with oxygen/ventilatory support.
Pulmonary hypertension (PHT) may be—(a) primary or idiopathic, (b) secondary to lung disease or airway

Fig. 16.19: Pulmonary edema (ARDS).
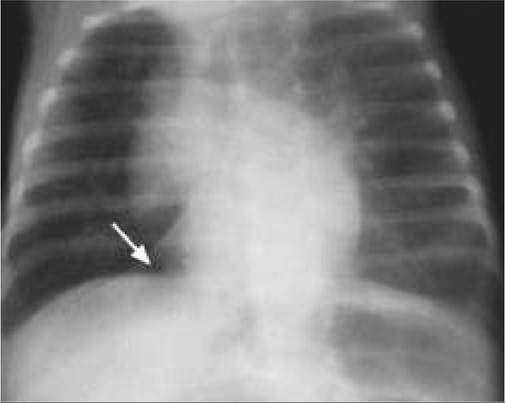
Fig. 16.20: Empyema thoracis.
obstruction, e.g. adenoids, pulmonary embolism, or
(c) secondary to cardiac disease (Ltgt;Rt shunt). PHT due to lung disease may lead to right ventricular hypertrophy/ dilation (Cor pulmonale) with congestive cardiac failure.
Diagnosis rests on cardiac evaluation (loud P2) and confirmed on echocardiography and cardiac catheterization. Treatment is same as for CCF, though IV prostacyclines may help to reduce PHT in severe cases.
Persistent pulmonary hypertension in newborn (PPHN) is an important hemodynamic complication in sick newborns, discussed elsewhere (Ch 12.12.2) due to pulmonary vasospasm or hyperplasia leading to pulmonary hypertension and consequent right to left shunting through foramen ovale or PDA.
16.12
More on the topic MISCELLANEOUS LUNG DISORDERS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- CONGENITAL LUNG MALFORMATIONS