NORMAL GAIT IS CYCLICAL AND SYMMETRIC
The principal goal of locomotion is to propel the body forward as efficiently as possible. The most natural way to accomplish this task is to employ a bipedal gait pattern, where the base of support alternates from one leg to the other.
Inman has described the cyclical alteration of each leg's support function and the existence of a transfer period when both feet are on the ground as essential features of normal locomotion (3). Since normal gait assumes no biomechanical advantage provided by either limb, a natural consequence of these essential features is the existence of a repeatable pattern that is both cyclical and symmetric. Figure 16.1 illustrates one complete gait cycle, or stride, and includes the time periods and temporal events associated with foot/floor contact that necessarily arise from changing the support limb. Temporal events are specific moments in time that divide the gait cycle into discrete time periods of specific duration, and are identified by the stick figures along the top of Figure 16.1. Typically, a cycle begins when one foot makes contact with the walking surface (initial contact) and ends when that same foot strikes again. This is the functional definition of a stride. Using such a convention allows a stride to be time-normalized, where a specific stride location is expressed as a percentage of the total cycle time or stride period. Time normalizing the gait cycle facilitates comparing subjects with different stride lengths, stride periods, and walking speeds on the same scale. Figure 16.1 illustrates the time periods and temporal events relative to the shaded ipsilateral side. If a subject's gait pattern is normal, the stride would be cyclical and symmetric inherently, and so be equally ascribed to either side. The temporal event of foot off (sometimes referred to as terminal contact) separates the gait cycle into stance and swing periods. Typically, stance period accounts for 60% to 62% of the total gait cycle and swing period takes the remaining 40% to 38%. We have intentionally refrained from using the terms “stance phase” and “swing phase” here to avoid confusing these intervals with the phases of gait to be introduced in a later section, although in common practice, the terms can be used interchangeably.Stance period includes two intervals of double limb support at the stance/swing transitions, each lasting approximately 10% to 12% of the gait cycle at typical walking speeds. These are generally described as initial and final double support, but can also be identified in the context of the leading limb as right or left double limb stance period. The duration of the double limb support periods decrease with increasing walking speed, reaching zero at the moment running begins. The time interval between the initial and double support periods is defined as the single support period, and is the same duration as the swing period of the opposite limb. Assuming normal symmetry, any reduction in double limb support time is absorbed by a proportional increase in single limb support time, but since single limb support always corresponds to the contralateral swing period, the overall stance period decreases, reaching 50% at the initiation of running when double limb support reaches zero. When both limbs' primary temporal events of foot-strike (initial contact) and foot-off (terminal contact) are represented on the same time scale, the duration of each time period is easily illustrated. These general terms for temporal events are applicable, regardless of gait pathology. Other terms are routinely used to identify temporal events marking the transition from swing period to stance period (heel strike, forefoot initial contact, foot flat) and stance to swing (toe-off, push-off), but should only be used when they clearly describe the observed foot/floor contact pattern.
While period durations relative to a single side are easily described when the gait cycle is represented on a linear scale, left/right symmetry may be more easily conceptualized when the gait cycle is wrapped around a unit circle (2,4,5), as shown in Figure 16.2.
For typically developing children and adults, ipsilateral and contralateral initial contact and foot-off will occur directly opposite each other around the circle, or 180 degrees out of phase. This graphically illustrates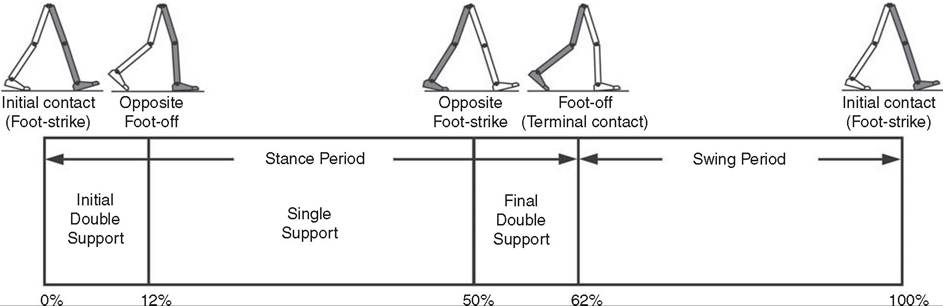
Figure 16.1 A typical gait cycle normalized in time, and represented on a linear scale from 0-100% of the total stride. This repeating cycle begins with initial contact and ends with the next initial contact of the same foot. The stick figures shown on top represent temporal events associated with foot-to-floor contact. They divide the cycle into swing and stance periods, one period of single support and two equal periods of double support.
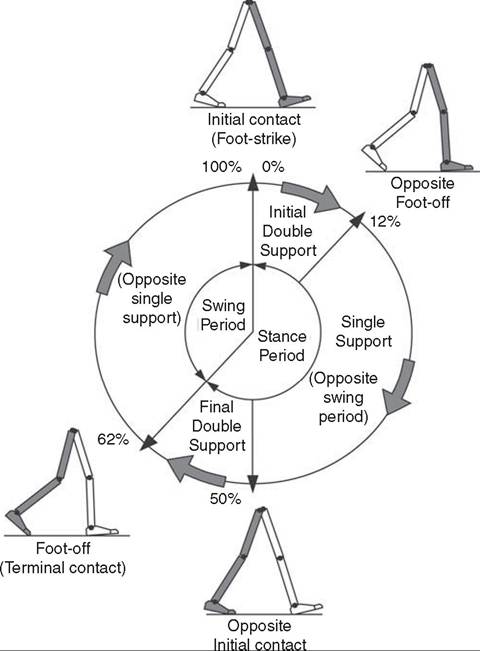
Figure 16.2 A typical gait cycle normalized in time, but wrapped around a continuous unit circle to illustrate symmetric phase relationships of temporal events and time periods. The beginning and end of the cycle occur at the 12 o'clock position. The temporal events of initial contact and foot-off for each leg are typically opposite each other on the unit circle, and the single support period of one limb is equal to the swing period of the opposite limb.
that the resulting time periods must be of equal duration for left and right single support, initial and final double support, and left and right swing periods. Any disruption in the natural sequence of temporal events anywhere along the cycle as a result of physical impairment, weakness, or spasticity will result in incorrect timing for the events that follow. This necessarily leads to a loss of symmetry that can be quantified by comparing the timing of temporal events between sides. Changes in symmetry reflected in the gait period durations is an index of gait pathology, and measuring this simple quantity can be quite useful for evaluating treatment performance over time.
Since the duration of the swing period and leg length determine the distance covered by the swinging limb, deviation from normal symmetry and timing will give rise to differences in step length on each side, and subsequently total distance traveled per gait cycle. By definition, step length and stride length are not synonymous. Step length is the distance (in the direction of progression) from a point of ground contact of the trailing foot to the next occurrence of the same point of ground contact with the leading foot. It is measured during initial double support and named for the leading limb. In contrast, stride length is the distance from initial contact of one foot to the next initial contact of the same foot, corresponds directly to the stride period, and is equivalent to the sum of successive left and right step lengths. Recognizing that speed is defined as the ratio of distance per unit time, step length, stride length, cadence (steps per minute), and walking speed are mathematically related by simple formulae:
walking speed (m/s) = (cadence ? stride length)∕120 or
step length (m) = (walking speed ? 60)/cadence
These basic outcome measures of overall gait performance, including the timing measures previously described and other quantities such a stance/swing ratio, are collectively known as temporal-distance or temporal-spatial parameters. They can provide considerable insight into the overall effect of subtle gait abnormalities on walking performance. For example, children with cerebral palsy may experience foot clearance problems during limb advancement due to excessive ankle plantar flexion or decreased knee flexion during swing period. Evidence of this could be found in prolonged single support times on the more normal or less involved side, and a reduced stance period, step length, and stance/swing ratio on the more involved side (6). If the source of the limb advancement problem can be attributed solely to the excess plantar flexion, the simplest intervention would be to prescribe a solid or leaf-spring ankle foot orthotic (AFO) with a rigid plantar flexion stop to restrict excess plantar flexion during swing.
Evidence that this intervention improved gait performance could be found in more symmetric single limb support times and step lengths, a more normal stance/swing ratio, and a higher walking speed.While clinical motion laboratories routinely compare a patient’s temporal-spatial measures to age- matched normative values, caution should be used when interpreting these results. Temporal-spatial parameters of cadence and stride length are directly related to walking speed (7), and since humans routinely walk at a variety of speeds, simple deviations from reference values alone may not be indicative of gait pathology. Rather, reduced values for these measures may simply reflect the need to adopt a speed appropriate to the terrain, the required task, or the size of the room (8). A person’s natural gait is also dependent on the environment, with studies showing that subjects walk faster on a long walkway compared to a short one, and typically walk faster in outdoor studies compared to indoor studies (9). This lack of consensus regarding normal values supports the convention adopted by most clinical laboratories to compare patient results to their own laboratory-collected references, where these environmental factors can be consistent for all subjects. Nevertheless, while it is “normal” to walk at a variety of speeds, it clearly is abnormal to walk asymmetrically, so side-to-side differences in temporal/spatial measures within a particular patient should always be investigated.
When comparing temporal-spatial parameters in children, even greater care must be exercised, since several age-related differences arise from the close relationship of these measures to leg length and gait maturity (10). Sutherland has shown that in typically developing children, heel-first initial contact, sagittal plane knee flexion wave, reciprocal arm swing, and an adult joint angle pattern are acquired prior to the development of mature temporal-spatial parameters (11). All of these adult gait characteristics arise before the age of 3 years in most children (6).
Because of this, Sutherland believes that gait maturity is best judged by the following five features, which he calls “determinants of mature gait (11).” These are: duration of single support, walking speed, cadence, step length, and ratio of pelvic span to ankle spread (P/A ratio). Notice that in addition to the first four measures that are fundamental temporal-spatial parameters, an anthropometric measure (P/A ratio) has been added, mainly to address the increased hip adduction common in the immature child's gait. In general, walking speed, step length, single support, and P/A ratio increase linearly with advancing age, with the greatest changes occurring during the first four years of life (6). Cadence decreases significantly between the ages of 1 and 2 years, after which it gradually continues to decrease (10). By age 4, the interrelationship between temporal/distance measures is fixed, although stride length and walking speed continue to increase with increasing leg length. Muscle phasic alterations in the early walkers are generally characterized by prolonged activation periods and subsequent longer periods of agonist/antagonist cocontraction around the joints of the lower extremities (12), most likely caused by neurologic immaturity associated with incomplete myeliniation (6). Despite all these age-related differences, the fundamental elements of a repetitive gait cycle are in place at a very early age. For this reason, asymmetric temporal/ spatial measures can be used as indicators of gait pathology in both children and adults.Because normal gait should be cyclical and symmetric, the existence of even small amounts of step-to-step variability may be an indication of gait pathology. Gait is most variable in the toddler, but gradually stabilizes as the child reaches adolescence (9). Hausdorff and colleagues have shown that the coefficient of variation for stride time in typically developing 3-4-year-olds is approximately 6%, but decreases to 2% in 11-14-year-olds (13). In the elderly, increased variability is associated with increased risk of falling, with speed variability the single best predictor of falls (9). These examples provide further evidence of the importance of a cyclical and symmetric gait pattern and how variations in symmetry and cycle times reflected in the temporal-spatial parameters of gait may be associated with gait pathology.