Overview
Scoliosis is a frontal plane deformity of the spine of >10 degrees, with frequent coexistence of rotational deformity. It is the most common pediatric spine deformity, and is classified into congenital, idiopathic (subtypes: infantile, juvenile, adolescent), neuromuscular and functional types (Table 14.6).
While the etiology, onset, prognosis, and treatments vary between classifications, the possible outcomes of severe untreated scoliosis are the same: respiratory compromise, seating compromise, pain, gait impairment, difficulty with activities of daily living, and psychological distress (280,281). Understanding the natural history and available interventions is important in helping patients achieve long-term comfort and functionality.Embryology, Growth, and Maturation
Spinal development is a complex process, which begins in the first month of gestation when mesoderm cells surrounding the notocord begin to differentiate into sclerotomes. These will ultimately form vertebral bodies and arches. Injury in early gestation often affects other nearby organs, primarily the cardiac, renal, and gastrointestinal systems. Approximately 60% of those with spinal anomalies have other congenital malformations, so abnormalities in these areas are essential to screen for (282).
14.6
Type of Scoliosis With Categorical Description
| TYPE OF SCOLIOSIS | CAUSE | SEX/AGE OF ONSET (YR) | COMMON ASSOCIATED CURVES | COMMON CHARACTERISTICS |
| Functional | Nonstructural, secondary to leg length discrepancy, herniated disk, trauma, arthritis | Any | None | Resolves with correction of underlying cause |
| Congenital | Failure of somite formation or segmentation 60% have other anomolies | Birth, but delayed diagnosis possible | None | Progressive tendency, surgery more likely |
| Idiopathic Infantile (Female,females progress more often, >10 yr | Right thoracic | 10% require treatment (bracing > surgery) | ||
| Neuromuscular | Upper or lower motor lesions, myopathic processes | Any age | Long sweeping typical | Aggressive, less responsive to bracing, |
progress after maturity
Unlike limb growth, vertebral growth is nonlinear.
Two major growth spurts typically occur: the first before the age of 3, and the second during puberty. The relationship of scoliosis to growth has been well established, and screening programs and surgical interventions best planned with these in mind. The Tanner stage and/or the Risser's sign classifications are helpful in predicting growth spurts, the progression of scoliosis, and the cessation of growth (193).While race, heredity, physical activity, physical disability, and nutrition may affect growth, growth typically accelerates girls at Tanner stage 2 and in boys at Tanner stage 3 (283).
The use of Risser lines, seen by posterior anterior (PA) radiographs of the iliac crest, assist in staging skeletal maturity and predicting future growth (Fig. 14.18). The Risser system is based on ossification of the iliac crest proceeding from the lateral to medial, and extends from grade 0 (no ossification) to grade 5 (complete fusion to iliac apophysis) (284,285). Risser 1 represents the period of most rapid skeletal growth, and correlation of the Risser's sign with the degree of a scoliotic curve can be predictive of curve progression (see Fig. 14.18).
Curve Classification and Naming
Scoliotic curves are named by their direction, location, and magnitude (Fig. 14.19). The curve's convex apex
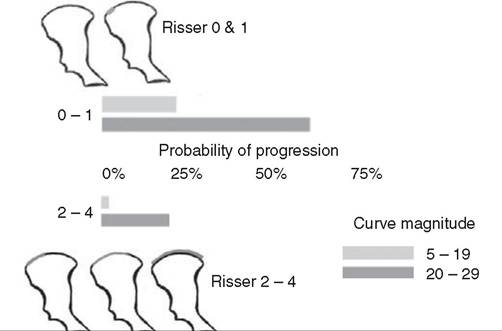
Figure 14.18 Risser sign. Likelihood of progression is based on the Risser sign and curve magnitude. (From Ref. 375)
(most laterally deviated vertebrae from the sacral line) indicates its named direction and location, and measurement by the Cobb angle provides its most reliable magnitude (Fig. 14.20) (286). If more than one curve exists, the largest-degree curve is designated as major and the others minor. Curves over 60 degrees are associated with restrictive lung disease.
Rotation of the spine, commonly present with scoliotic curves, is measured using a scoliometer when the child is bending forward, or radiographically by the Nash-Moe method or by CT scan (287,288).
Rotational deformities may complicate surgical correction.History, Physical Exam, and Treatment Overview
The scoliosis exam will vary, depending on the patient's age and associated diagnosis, but important general information must be collected from all patients. A positive family history is particularly pertinent in congenital and idiopathic scoliosis, and the presence of back pain may indicate a serious discitis or tumor. Rapid curve progression, bowel and bladder changes, recent trauma, associated weight loss, muscle weakness, or joint pain can point to other serious primary processes such as spinal cord syrinx or tethered cord, spinal fracture, rheu- matologic disease, osteoblastoma, or hip deformity.
Reflexes, strength, range of motion, general posture, and gait must be examined. Seating systems and assistive devices should be assessed, as improper walker or crutch height and truncal weakness with poor seating support can affect spinal position in children with disabilities. Examination of the skin for cafe au lait spots, webbed neck or low hairline, and
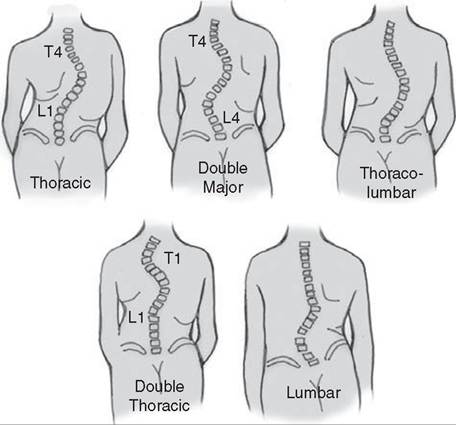
Figure 14.19 Classification of scoliosis. Scoliosis is classified into general categories by level. (Adapted from Ref. 284).
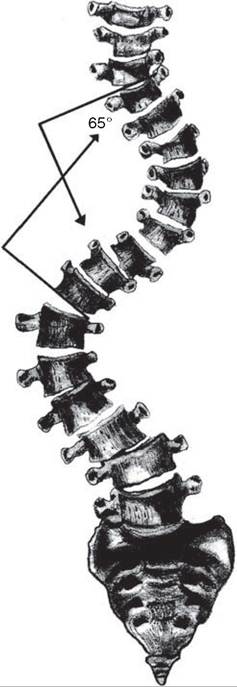
Figure 14.20 The Cobb method of measuring curvature in scoliosis. The angle measured is formed by perpendicular lines drawn through the superior border of the upper vertebra and the inferior border of the lowest vertebra of a given curve.
hairy patches or skin dimples may lead to recognition of disorders such as Klippel-Feil, spina bifida occulta, or neurofibromatosis. Excessive height, arm span, or joint hyperextensibility may signal a connective tissue disorder of which scoliosis is only a presenting symptom. Leg length, straight-leg raise, and range of motion should be checked, as length discrepancies, asymmetry, contracture, or pain may point to hip dysplasia or an underlying neurologic disorder such as hemiplegia or herniated disk.
Examine the back for pelvic obliquity, elevation of either iliac crest, or asymmetry of the scapula or shoulder girdle. Forward bending (Adam's test) with the feet and palms together may show asymmetrical prominence of the rib cage (vertebra rotate into the convexity of the curve), which can be measured with a scoliometer. A rotation of over 7 degrees warrants further investigation. Side bending may help assess the flexibility or rigidity of a curve, which is important when considering treatment options.
Curve Documentation. A full spine PA radiograph is usually appropriate for screening purposes, although certain curves (ie, congenital, infantile) may require CT or MRI evaluation. Curves with significant rotational components or kyphosis may require lateral views. Radiographs should be taken standing, if possible and, if wearing an orthosis, both in and out of the brace. Cobb angles, which have proven reliable in tracking curves, should be followed every three months to a year, depending on the rate of progression (286). Serial evaluations should continue until growth is complete, although neuromuscular curves often progress after maturity, so continued screening is warranted (284).
General Treatment Options. Orthotic management is not appropriate, effective, or recommended for all forms of scoliosis. Long-term bracing, while reducing curve progression and maintaining flexibility, needs to be considered carefully with respect to function, social development, and self-esteem (285).
Curves less than 40 degrees are typically compatible with bracing, but their location affects brace choice. Curves with apex at or below T7 are typically managed with a soft or rigid TLSO, which allows more functional activity than the Milwaukee brace used for curves above T7 (Fig. 14.21). This brace often incorporates a chin and head pad, is more restrictive, and is less well tolerated. It is recommended that both braces be worn 16-24 hours a day to be effective (282). Removing the brace for an hour or two per day to accommodate athletic or recreational pursuits is not uncommon.
A Charleston- or Providence-style brace, which bends the body away from the curve and is worn at nighttime, may be more tolerable, but is likely to be less effective unless it is used for a thoracolumbar curve of less than 35 degrees (see Fig. 14.21) (282).Surgical Interventions. Achieving a balanced spine (head and shoulders over sacrum), a solid arthrodesis, and a reduction in the deformity are the primary goals of surgical intervention. Surgical techniques vary by type of scoliosis. Titanium instrumentation is recommended when it is clear that MRI imaging will be needed in the future, given the frequency of coexisting organ and developmental abnormalities seen in some children. Continuous intraoperative spinal monitoring (somatosensory-evoked potentials, motor- evoked potentials) is important for preventing neurologic injury during surgery (288). Complications of surgery vary with patient diagnosis, curve size, and a multitude of other factors, but infection, pseudarthrosis, anemia, hypotension, and hardware failure are the most common.
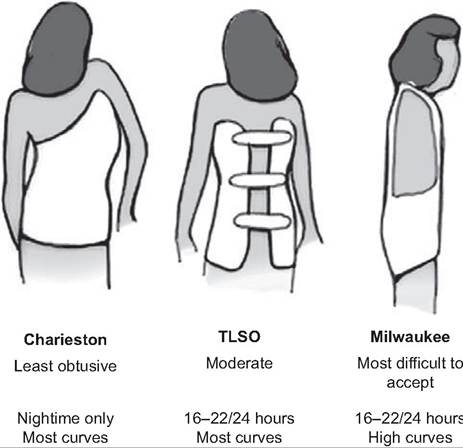
Figure 14.21 Types of braces. These are common braces and generalizations about their use. (Adapted from Ref. 284.)