DEVELOPMENTAL CONDITIONS
Legg-Calve-Perthes disease is osteonecrosis of the capital femoral epiphysis in children (11). The condition usually presents between the ages of 4 and 10 years, with a peak incidence of 5 to 7 years.
Presentation has been seen as early as 2 years and as late as the late teens. There is a definite male preponderance, with a 4:1 ratio. The incidence of bilaterality has been reported as 10% to 12% (171,172), rarely simultaneous. There is no evidence that the condition is inherited. Limitations in internal rotation, extension, and abduction of the effected hip, with slight shortening of the leg, are common physical findings. Children presenting with knee pain always require a thorough examination of the hip, as this is a common referral pattern. Catterall classification (173) is graded over four degrees of involvement, depending upon the extent of necrosis across the capital femoral epiphysis. A Catterall classification I involves up to 25% of capital femoral epiphysis involvement; classification II, 25% to 50%; classification III, 51% to loccurs under the age of 6. The short-term goal is reduction of pain and stiffness of the hip. The disease process is self-limited and may last for two to four years. NSAIDs are effective in reducing synovitis. Restriction of activity helps relieve pain, which at times may include non-weight bearing with crutches. Abduction orthosis and casting may be helpful at some point, with improved abduction and femoral head containment the goal. For abduction orthosis to function satisfactorily, the affected hip must be able to be abducted in extension to 40 or 45 degrees. After the orthosis is applied, an anterior-posterior (AP) radiograph of the pelvis is obtained to ensure that the affected femoral head is contained within the acetabulum. To be effective, the orthosis must be worn full-time. The use of the orthosis is continued until subchondral reossification is demonstrated on the AP radiograph (174,175). The important principal of treatment is based on femoral head containment within a spherical acetabulum so that at least theoretically, reossification is also spherical. Generally, the active phase of the disease that requires an orthosis is 9 to 18 months. Patients with Catterall classifications I or II can be treated conservatively, while levels III or IV often require more surgical intervention. Surgery, including proximal femoral varus osteotomy, may eliminate longer-term bracing and allow earlier resumption of activities in some children. The prognosis again is better with earlier detection under the age of 8 years and with less than 50% involvement of the femoral head. With increased involvement of the lateral femoral head, more extensive surgical options may be chosen. Femoral osteotomy can result in elevation of the greater trochanter accentuating the abductor dysfunction. Patients older than 9 years of age at onset with Catterall groups III and IV have unpredictable success rates, regardless of treatment methodology. Return to high-impact athletics is restricted until a pain-free status is found during clinical examination and radiographs show healing. Osteoarthritis later in life is often seen, with 50% of untreated patients showing severe changes by the age of 50 years (176). Other causes of avascular necrosis always need to be considered, including sickle cell anemia, femoral neck fracture, Gaucher’s disease, slipped epiphysis, congenital hip dislocations, rheumatoid arthritis, and other collagen disorders, not to mention steroid therapy. Bilateral involvement may be confused with multiple epiphyseal dysplasia or spondyloepiphyseal dysplasia and can be differentiated by doing a skeletal survey. Acute transient synovitis of the hip (ATS) is the most common cause of hip pain in children and can present in a fashion similar to Legg-Calve’- Perthes disease (6). In fact, a transient ischemia may occur during acute synovitis of the hip with some rare reports of progression to Legg-Calve’-Perthes disease at a later date. The condition may develop at any time from toddler age onward, with a peak age between 3 and 6 years, and slightly more common in boys. At least half of the children with ATS have or recently have had an upper respiratory illness, including pharyngitis or otis media. Trauma of a mild nature is frequently present. Annual hospital admissions for the diagnosis of ATS are reported between 0.4% to 0.9% (6,10,177). The actual incidence of ATS is likely higher, however, as many patients never seek medical attention, and a minority of patients are hospitalized once the diagnosis is made. A lower incidence in African Americans has been noted (178). Ninety five percent of the cases are unilateral. Annual risk of recurrence for a child with an affected hip is 4% (179). Viral etiologies are suspected. Common presentations include rapid onset of limping, unilateral pain involving the hip or groin with referral to the knee, and refusal to bear weight on the involved extremity in an otherwise healthy child. A low-grade fever may be present related somewhat to an associated upper respiratory infection. Septic arthritis needs to be excluded, as this is a much more serious joint- and limb-threatening condition. Radiographs are frequently reported as normal when compared to the opposite side, but may show some slight intracap- sular effusion. Ultrasonography remains most helpful in detecting effusion (180) and may correlate with MR imaging and a positive radionuclear bone scan. ATS remains a diagnosis only after other conditions have been excluded. Laboratory evaluation may show normal to mild elevation of the white blood cell count and erythrocyte sedimentation rate along with the C-reactive protein. Other laboratory parameters are generally within normal limits. Upon hospital admission, aspiration of the hip joint should be performed if septic arthritis is suspected. Long-term follow-up of children with ATS has demonstrated some Iife- long abnormalities, including increased coxa magna (defined as an enlargement of 2 mm or more of the proximal femoral epiphyses) in one-third of patients (181). A reactive increase in the blood supply to the femur with increased growth of the articular cartilage secondary to the transient inflammation may be associated with this finding (182). Long-term changes of degenerative arthritis in the hip have been reported in some individuals as well. The fundamental treatment consists of rest and age-appropriate NSAIDs. Partial weight bearing with crutches can begin with improvement in pain and full range of motion through the hip. Most patients will resolve of symptomatology within five to seven days, and recurrence is uncommon unless premature activity occurs. Persistent symptoms should be reevaluated, realizing that low-grade symptomatology can last, in some, up to several weeks. Full, unrestricted activity should be avoided until the hip is completely pain-free and there is no evidence of limping.A slipped capital femoral epiphysis (SCFE) usually involves posterior inferior displacement of the epiphysis on the proximal femoral metaphysis. The term slipped capital femoral epiphysis is actually a misnomer. More accurately, the epiphysis remains in normal position within the acetabulum while the proximal femoral neck and shaft move anteriorly and rotate externally relative to the femoral head (183). The incidence of SCFE in the literature can vary between 1 and 61 per 100,000 persons (11). SCFE is approximately twice as common in boys than in girls and may be bilateral in up to 25% of cases, 5% of which occur simultaneously (6,184). More than 90% who develop late SCFE on the contralateral side are asymptomatic. Affected children are often large and overweight, and an association with endocrine factors such as hypothyroidism, hypopituitarism, hypogonadism, and excessive growth hormone has been reported. Body mass index (BMI) may be an accurate tool for assessment of risk for SCFE (185). Findings show that patients with SCFE had a statistically higher BMI during growth than normal developing children. It is more common in African American boys with accumulated risk that may be as high as 1 in 400 (11).
It is also more common in northern environments, possibly related to less sun exposure and relative vitamin D deficiency. Laboratory studies have demonstrated that estrogen strengthens and testosterone weakens the physes (186,187). SCFE may be thought of as occurring because of physiologic loads across an abnormally weak physes (more common in peripubertal children) or abnormally high loads across a normal physes (more common in obese children). The increased prevalence of hypothyroidism in children with Down's syndrome is a likely explanation for the increased risk of this condition in these children (188,189). Mechanical factors appear important with an association of SCFE, with decreased femoral anteversion and femoral neck shaft angle (190). Age at presentation is typically between 12 to 16 years for boys and 10 to 14 years for girls. Presentations of SCFE outside of these age ranges should alert physicians to potential endocrinopathy or alternative conditions such as renal osteodystrophy. The two most common features of presentation are pain and altered gait. The pain may come on acutely (unstable SCFE), but more commonly builds over a number of weeks or months. As usual with hip pathology in children, pain occurs in the groin region and radiates to the knee and medial thigh. It is aggravated by walking and other high-impact activities. External rotation of the leg is common with some shortening and antalgic Trendelenburg's gait. Physical examination demonstrates a loss of internal rotation, diminished flexion, shortening of the leg, and atrophy of the thigh if the symptoms have been longstanding. Mild slips show displacement of the epiphysis up to one-third of width of the metaphysis, moderate slips up to two-thirds, and severe slips greater than two-thirds displacement. The displacement is best quantified on lateral radiographs, which should not be lacking in the workup of a child with hip pain. Klein's line (or Trethowan's sign) is a line drawn along the superior surface of the femoral neck, which normally should pass through the lateral portion of the capital femoral epiphysis. If this line passes above the epiphysis, at least minimal slippage is present and further intervention required (191,192). Slip angle is another good way of measuring degree of severity on a true lateral radiography (193). A perpendicular line drawn from the base of the capital femoral epiphysis bisecting a line drawn through the midshaft of the proximal femur is measured. An angle less than 30 degrees is mild slippage, 30 to 60 degrees moderate, and 60 to 90 degrees severe. When SCFE is suspected, ambulation should not be allowed until an orthopedic surgeon sees the child. Other radiographic features include widening of the epiphyseal line (Salter I fracture-type appearance) with metaphysial changes including rarefaction and cysts. Bone scan and MRI can be helpful in determining the preslip stage as compared to the opposite uninvolved side (11). The current standard of treatment for SCFE is situ two cannulated screw fixation done on an urgent basis. The goal of treatment is to arrest further progression of the slip and to gain closure of the capital femoral epiphysis. Management of patients with unstable SCFE can involve minimal repositioning by an experienced orthopedist and two-screw fixation instead of one. Generally, the epiphysis is left in its displaced position because avascular necrosis is a 10% to 25% risk if manipulation is attempted. Spontaneous reduction of the slippage or controlled reduction by an experienced orthopedist under fluoroscopic guidance has not been associated with an increased rate of osteonecrosis in patients with unstable SCFE (11). Cortical bone grafts have also been used, crossing from the metaphysis to the epiphysis and resulting in epiphysiodesis. Spica casting is becoming a less common practice because of secondary complications in obese children and immobility for up to three months. After successful physeal closure, the proximal femur can remodel, particularly in children under the age of 10 years. Bony osteotomies can be indicated if further femoral head coverage is required despite more conservative care. Chondrolysis or acute cartilage necrosis may occur postoperatively in severe cases. If chondrolysis is present, most individuals go on to develop narrowing of the joint space with some degree of ankylosis, degenerative arthrosis, and pain. Total hip arthroplasty can be a consideration for older individuals. Weight bearing is generally avoided for at least six weeks after surgery followed by active assistive exercises and strengthening to restore lengthening, adduction, and internal rotation. Full identification of this condition while only minimal displacement is present and immediate surgery generally allow rapid mobilization and return to full activity with no sequelae. Prophylactic pinning of the contralateral hip is an area of ongoing discussion. In one recent study of 94 hips treated with prophylactic pinning, there were no significant complications (194). The risk of osteonecrosis and chondrolysis was felt to be virtually negligible when using insight two-screw fixation with improved imaging technology and radiolucent tables. Opponents of prophylactic pinning cite the complications and potential risks of pinning numerous hips that will never slip. They also point out that with appropriate patient counseling and close follow-up, most subsequent slips will be detected early while they are still mild and treatable. Currently, prophylactic contralateral hip fixation is recommended for patients with established metabolic or endocrine disorders, those with increased risk from radiotherapy or chemotherapy, and for children with SCFE who are younger than 10 years of age. Once the triradiate cartilage is closed (around the age of 14 to 16 years) and when Risser lines appear, the risk of contralateral slip is felt to be negligible (11). SCFE differs from other pediatric disorders of the hip such as Legg-Calve-Perthes disease and developmental dysplasia of the hip, in that SCFE occurs at an age when the majority of the acetabulum has been developed and thus less acetabular adaptation to deformity of the femoral head can occur. All of this speaks to early detection and early treatment, particularly in those children of elevated risk.Developmental dysplasia of the hip (DDH) is the most common disorder of the hip in children and the musculoskeletal condition, causing the highest level of concern for the pediatric practitioner (11). Dysplasia of the hip (mostly involving the acetabulum) occurs in approximately 1 in 100 births, with frank dislocation in approximately 1.5 births per 1,000. DDH is not always detectable at birth, and thus the term “developmental” rather than “congenital” has been chosen by the Pediatric Orthopedic Society of North America. The term DDH is felt to more accurately reflect the variable presentation of this complex disorder. Dysplasia refers to an underdeveloped acetabulum, subluxation to hip still in partial contact, with the acetabulum and dislocation to femoral head not contained in the acetabulum. The dislocated hip should be detectable clinically in the newborn period by four to six weeks. Teratologic hip dislocations (atypical) occur in utero and are not reducible on neonatal examination. Atypical dislocations are present about 10% of the time and are more commonly associated with other chromosomal or neuromuscular conditions, such as myelomeningocele, arthrogryposis, or Ehlers-Danlos syndrome. Typical DDH occurs in an otherwise normal infant and may take place in utero, perinatally, or postnatally (Table 14.4). Risk factors associated with DDH are listed in Table 14.5. DDH predominates
Classification of Developmental Dysplasia of the Hip
| Classification | description |
| Atypical (10%) or teratological | Primarily malformed acetabulum or femoral head in utero associated with myelomeningoceole, arthrogryposis, Ehler-Danlos or other syndromes |
| Typical (90%) | Otherwise normal infant but varying degrees of hip morphology and placement |
| Subluxed | The femoral head and the acetabular cartilage are in contact, but not correctly centered |
| Dislocatable | The femoral head can be dislocated with maneuvering |
| Dislocated | The femoral head is completely out of the acetabulum |
14.4
in the left hip (60%), but often bilateral involvement can be discovered. Bilaterality can be most difficult to diagnose with the absence of asymmetry as a helper. Beware of bilateral DDH when thigh skin folds extend past the anus and decreased absolute abduction is present on both sides (6). In the older child, bilateral involvement may be detected only by hyperlordosis and a waddling gait. First-born females presenting with breech have the highest risk for DDH at 8% (11). Risks for DDH in subsequent pregnancies is 6% when neither parent has a positive history and 12% when one parent is with positive history. The presence of idiopathic clubfeet do not obligate special screening (195), but this may be helpful in a small percentage. Ultrasound screening of newborn hips continues to be with some controversy (196). The technique is sensitive for detecting abnormalities of the newborn hip, but has poor specificity in detecting patients with DDH who require treatment. Cost-effectiveness has yet to be shown. Neonatal hips with immaturity or mild dysplasia that have no instability do not benefit from early treatment, as more than 95% of such hips spontaneously normalize (197,198). Certainly infants with risk factors (see Table 14.5) need to be screened in ultrasound followed by careful clinical examinations until the child reaches walking age. The alpha angle is measured from the vertical reference through the iliac bone and tangential to the osseous roof of the acetabulum. This angle represents the hard bony roof and reflects acetabular depth (11). The beta angle is created by the vertical reference through the iliac bone, intersecting with a line drawn
14.5
Risk Factors Associated With Developmental Dysplasia of the Hip
Caucasian
Hip swaddling in extension (Native American, Lapland) Female: Male ratio 6:1
Breech birth
Positive Family History
Primaparity
Ligamentous laxity
High birth weight (>4000gm)
Congenital muscular torticollis
Metatarsus adductus
Oligohydramnios
Hip asymmetry (limited abduction of one or both hips) Congenital knee dislocation/recurvatum.
through the labrum representing the cartilaginous roof of the acetabulum. The beta angle indirectly reflects the lateral position of the femoral head. A normal alpha angle is greater than or equal to 60 degrees and a beta angle less than 55 degrees (199). DDH classification is based on the Graf method (200), with varying severity having type I, a normal hip and type IV, a severely affected dislocated hip. After 4 to 5 months of age, when the ossific nucleus of the femoral head has generally appeared, radiographic screening replaces ultrasound in evaluation of infants with DDH. Parameters for monitoring hip dysplasia in this age group are represented in Figure 14.10. Measurement of center-edge angle becomes useful in the patient who is more than 5 years of age and particularly useful in the adult patient (201). Center-edge angles are less than 20 degrees (angle between a vertical line drawn through the center of the femoral head intersecting with the tangential line drawn through the lateral acetabular edge) are concerning for unwanted lateralization of the femoral head. Clinical examination with repetitive follow-up continues to be the mainstay of diagnosis for DDH (6). The infant should be quiet and comfortable so the muscles about the hip are relaxed and supple to exam. In early infancy, instability is the most reliable sign (193). Instability declines rapidly with age, over 50% within the first week. Stiffness, shortening, and limited abduction become much more prominent by 2 to 3 months of age. Initial instability may be the result of maternal or fetal hormonal laxity, genetics, and intra- or extra- uterine malpositioning. The longer the femoral head remains in a subluxated or dislocated position, the more likely progressive change in acetabular anatomy will occur. A hip that is reduced at rest but subluxated or dislocated by adduction, flexion, and posterior pressure has a positive Barlow's maneuver. Concurrent acetabular dysplasia may or may
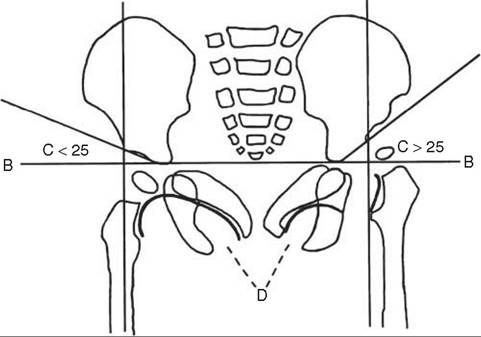
Figure 14.10 Radiographic evaluation in developmental hip dislocation. (A) Perkin's vertical line: perpendicular dropped from the lateral acetabular margin. (B) Hilgenreiner's line, through the Y cartilages. The femoral head should lie in the lower medial quadrant formed by the intersection of the two lines. (C) Acetabular index: the angle formed by a line through the acetabular roof and Hilgenreiner's line; normal below 25 degrees. (D) Shenton's line: the arc appears broken in the presence of dislocation. The abnormal hip appears on the right.
not be present (197,198). Barlow tests often become negative by 2 to 3 weeks of age as maternal or fetal hormonal influences diminish. Hips that are dislocated can be reduced back into the acetabulum by abduction and forward lifting of the thigh producing a palpable “clunk.” A hip that is reduced this way has a positive Ortolani’s sign and is often accompanied by acetabular maldevelopemnt. Hip “clicks” are short-duration, high-pitched sounds that are common, benign, and need to be distinguished clearly from “clunks.” “Clicks” and asymmetrical thigh folds are common in normal infants and generally benign (193). A positive Galeazzi’s sign may be seen in infants with DDH, noting a decrease in height of the involved knee with the hips flexed supine to 90 degrees. In infants older than 3 months, limitation of motion and apparent limb shortening predominate. The dislocated or subluxed hip develops tightness in the adductor muscle groups with limited asymmetric abduction. Again, this is much easier to detect when unilateral than bilateral. Parental or family reports of an infant with unusual positioning of legs or crawling warrants investigation. In older ambulatory patients, Trendelenburg’s limp, waddling gait, and hyperlor- dotic posture require evaluation. Fatigue, pain, and instability can still occur in adolescence.
For the infant with a positive Barlow’s sign and normal ultrasound at 4 to 6 weeks (no evidence of instability on stress maneuvers) with clinical stability returned, no treatment or radiograph follow-up is recommended (11). Serial clinical examinations of the hip should continue by the primary care physician until the child reaches walking age.
For children with dysplasia and an abnormal ultrasound or persistent subluxation, treatment is with the Pavlik harness. Follow-up clinical examinations should be completed at least every two weeks, with serial ultrasound studies at least monthly. The Pavlik harness needs to be adjusted at least every two weeks for the rapid growth evident in this young infantile population. Failure to adjust the Pavlik harness can cause additional acetabular pathology, including a now-dislocated hip that was previously reduced. The anterior adjustable straps for the Pavlik harness are set to keep the hips flexed at approximately 100 degrees. Excessive flexion and tightening needs to be avoided, as additional problems can be caused such as femoral nerve palsy. The posterior straps are meant to encourage gentle abduction of approximately 45 degrees. They should be loose enough to allow two to three fingerbreadths between the knees when the knees are held flexed and adducted. Forced abduction should be avoided to minimize any complication of osteonecrosis. The child can be weaned from the Pavlik harness over a three- to four-week period once ultrasound parameters become normal along with stability on clinical examination. Treatment with the Pavlik harness for neonatal acetabular dysplasia is more than 90% successful. Follow-up is still required with AP radiographs through the growing years, with a 10% risk of deformity necessitating clinical follow-up into adolescence. Fixed hip abduction orthosis replaces the Pavlik harness in children over 6 months of age, generally because of strength and size (202). Early screening and repetitive clinical examinations have been shown to significantly reduce surgical procedures and hospitalizations, including late presentation of DDH in this population (203,204,205).
A hip with reducible dislocation (Ortolani’s sign positive) may still be initially treated with the Pavlik harness under 2 months of age. Ultrasound imaging is required to document hip centering over the acetabulum once in the harness (206). Clinical and ultrasound follow-up is weekly, with a careful clinical examination at three weeks, prior to further decision-making. If the hip is not reduced, continuation of the harness until normal exam, ultrasound, or radiographs have been obtained can occur (206). If instability is present on exam but reducible, a fixed abduction brace or spica casting should be considered (6). If the hip is not reduced, traction, adductor tenotomy, or closed or open reduction including arthrogram and spica casting need to be considered (201). Treatment with the Pavlik harness is effective in achieving reduction of a reducible hip in 85% of patients with a low incidence of osteonecrosis (less than 5%) with early treatment (11). Persisting with the Pavlik harness when reduction is not achieved by three to four weeks may cause additional femoral head deformity or posterior fixation, and make closed reduction difficult or impossible (193). The Pavlik harness is not appropriate for teratologic dislocation.
The preferred method of treatment in children 18 months of age or younger is closed reduction, provided it can be achieved without undue force (11). The preliminary use of traction for three to four weeks before attempting closed reduction is becoming less common (207,208). The quality of reduction is confirmed by arthrography and objectively defined by the width of the contrast column remaining between the femoral head and the acetabulum, including the status of the limbus. Stability of the reduction needs to be assessed in all planes by determining the stable zone and safe zone. The stable zone is defined as a difference between the maximum abduction of the hip and the minimal amount of abduction before hip dislocation (6). The safe zone is the range of motion where the hip is safe from excessive abduction that can cause osteonecrosis and adduction that may facilitate dislocation. The safe zone is generally 15 degrees less on the limits of motion defined in the stable zone. With the stable and safe zone in mind, reduction is maintained in a bilateral hip spica cast (202). The hips are generally maintained in about 0- to 100 degrees of flexion, with abduction less than 60 degrees. Reduction of the hip or hips in the spica cast must be confirmed, usually by CT scan (6). Immobilization in the spica is continued for approximately three to four months with cast changes about every six weeks. With clinical stability achieved and visualized on radiographs, abduction bracing can be used subsequently until a normal acetabulum is achieved.
When treatment with the Pavlik harness and/or closed reduction fails, surgical reduction is required, more commonly after the age of 18 months (206). Often, the decision to perform open reduction is made in the operating room following arthrography and failed closed reduction. The purpose of open reduction is to remove obstacles to reduction, achieving increased stability and clinical outcome. Intraoperative arthrography can be helpful in defining specific anatomic blocks to reduction and choosing the best surgical approach. Obstacles to reduction include the iliopsoas tendon, which is interposed between the femoral head and acetabulum and often must be released. Capsular constriction needs to be released in addition to the transverse acetabulum ligament when blocking a deep concentric reduction (193). Pulvinar fatty fibrous tissue filling the depth of the acetabulum is removed with a rongeur. The ligamentum teres, when hypertrophied, is usually removed, the vascular contribution of which is felt to be minimal. The limbus is generally left alone, as it will remodel and form the labrum postoperatively, an important structure for hip stability and longevity (6). Numerous pelvic and femoral osteotomies are available, with choice based on the pathology and the experience in surgical preference (206). Femoral shortening can relieve pressure on the femoral head and acetabulum, reducing cartilaginous pressure and the risk of osteonecrosis (209,210). Derotational femoral osteotomy can be helpful if excessive anteversion is present requiring extreme internal rotation to maintain reduction. Secondary producers, including redirectional femoral and pelvic osteotomies, are more common after the age of 2 in an effort to maintain concentric reduction and minimize the risk of osteonecrosis. Remodeling of the hip and acetabulum is most predictable under the age of 4, less predictable between the ages of 4 and 8, and unpredictable after the age of 8. Secondary procedures should be performed if at all possible prior to the age of 8 for best outcome (206). Failure to achieve reduction in the older child results in a permanently subluxed hip with marked gait deviation and susceptibility to osteoarthritis and pain syndromes. Long-term outcomes can include joint arthrodesis and the need for total hip arthroplasty in the younger adult (6). Spica casts applied after surgery need appropriate infantile care for hygiene, toileting, and positioning and mobility devices such as scooters, carts, and accessible toys. The importance of early diagnosis and treatment of developmental hip dysplasia cannot be overemphasized: The results are generally good with appropriate intervention and disastrous if neglected.
Traumatic hip dislocations in children are relatively rare, and when they occur, they are usually posterior (11,211,212). The mechanism is usually traumatic, with a direct blow to the knee with hip and knee flexed, as occurs with a fall during ground impact or dashboard contact injury in a car accident. Some dislocations have occurred during mini rugby, in which players kneeling on the ground have had someone fall on top of them. Avascular necrosis may occur in up to 10% of cases. Sciatic nerve palsy is rare, but needs to be ruled out. Only 5% of all traumatic hip dislocations occur in patients younger than 14 years. Males account for approximately two-thirds of these dislocations, with more than 99% being unilateral. Posterior hip dislocation is an emergency that requires immediate referral to an orthopedic specialist (6).
Overuse syndromes are generally conditions caused by unresolved Submaximal stress in previously normal tissues. They involve microtrauma resulting from chronic repetitive insults to the musculoskeletal system. With focus on single sports early in life, these injuries have become more prevalent in the pediatric athlete (6,193). Growth cartilage seems to be more susceptible to stress and overuse than adult cartilage. Growth cartilage is present at three different sites: the physes, the joint surface, and the major muscle-tendon insertions or apophyses. Little League elbow comprises a group of pathologic entities in and about the elbow joint in young developing pitchers. The injury may include medial epicondular fragmentation and evulsion, osteochondritis of the capitulum or radial head, and delayed closure of the growth plates around the elbow (213). The mechanism of injury appears to be repetitive valgus strain applied to the elbow by throwing (214). Guidelines for young pitchers include participation in only three to four innings per game, fewer than 90 pitches per outing, fewer than 200 pitches per week and mandatory rest periods between appearances (11). Stress injuries to the distal, radial, and ulnar physes are commonly found in gymnasts (6,214). X-rays demonstrate widened epiphyses, cystic changes, and beaking of the distal metaphysis (215, 216). Some risk of distal, radial, and ulnar growth arrest exist. Overuse injuries around the pelvis and hips are common and may be seen along the iliac crest; ischial tuberocities; and anterior, superior or inferior iliac spine. Sometimes, late diagnosis of the avulsion of the ischial tuberocity is mistaken for an osteosarcoma. An avulsion may occur with a hamstring tear in a child sprinting during sporting activities or other recreational pursuits. Bones grow faster than muscles in children, and with associated growth spurts and limited stretching and warm-up activities, epiphyseal avulsions are more common (214). Treatment of overuse syndromes generally involves conservative modalities and rest, followed by strengthening and stretching of muscle imbalances and gradual return to activity as tolerated. The snapping hip syndrome in children is an entity most commonly associated with iliotibial band irritation of the greater trochanteric bursa on hip flexion, extension, and internal rotation (6). It can also occur with the iliopsoas snapping over the lesser trochanteric process (193). Osteoitis pubis is more common in adults, but may be occasionally seen in older teenagers with high-mileage running (6,217).
The most frequently injured area in childhood and adolescent athletics is the knee (6,11,193). The collateral ligaments of the knee, especially the medial collateral ligament, are frequently injured in sports. An isolated injury to the medial collateral ligament usually may be treated successfully without surgery in the immature athlete. Anterior cruciate ligament (ACL) injury in the immature athlete has always been considered a relatively rare occurrence (6). Increased participation in organized sports, along with improved imaging techniques such as MRI, appears responsible for the reported increased incidence of this injury (218,219). Girls are two to nine times more likely to disrupt their ACL than boys (220), with a soccer injury a common scenario. Often, these injuries are associated with avulsion of the anterior tibial spine. Anterior cruciate ligament reconstructions in children, when performed, need to consider early closure of the distal, femoral, or proximal tibial physes or other growth disturbances with grafts that might cross the growth plate (221). Concerning growth disturbances include limb length discrepancy and angular deformities. Autogenous patellar tendon grafting appears to be the surgical choice, not to exclude other surgical considerations of autologous iliotibial graft or hamstring autograft or allograft. Over-the-top femoral graft placements (graft passed through the interchondular notch of the femur) have been reported by some authors with good success and efforts to spare excessive physeal penetration (222,223,224). Additional physeal-sparing reconstructions with minimal risk of growth arrest have been reported, with good success in the younger child (under 12) and adolescence (225). Conservative care, including rest, elevation, ice and derotational bracing, are recommended initially under a rehabilitation program that can take two to three months. Surgical repair is considered thereafter for ongoing instability and to minimize additional cartilaginous and meniscial injuries. An isolated meniscial tear in a child under the age of 10 is unusual. Surgery is used only if conservative measures fail. The choice is often repair of the meniscus rather than surgical resection because of the increased potential in children for cartilaginous healing.
The elbow continues to be the most commonly injured joint in children (6). Acquired dislocations account for about 8% of elbow injuries and are most frequent in children under the age of 10 years (11,226,227). Typically, the injury involves the nondominant extremity with a fall onto the outstretched hand (228). Nursemaid’s elbow consists of radial head subluxation from a sharp upward pull on the extended pronated arm in preschoolers. A generalized ligament dyslaxia of children with large cartilaginous components of the distal humerus and proximal ulna, in addition to osseous instability, with numerous secondary ossification centers and epiphysis all contribute to the tendency for the pediatric elbow to dislocate. Posterior or posteriolateral dislocations account for up to 90% of the injury and can be reduced through numerous conservative techniques (6,228,229). With nursemaid’s elbow, typically the child will not move the arm and holds it in a slightly flexed and pronated position. Radiographs are usually not indicated, as the injury is more subluxation of the annular ligament rather than true joint subluxation. Longitudinal traction and additional pronation followed by flexing the elbow above 90 degrees and then fully and firmly supinating the form produces reduction in most cases. A click or snap is often felt as the annular ligament repositions (6).
Shoulder injuries remain relatively uncommon in the overall picture of injuries to the pediatric musculoskeletal system (11). When they occur, they include separation of the acromioclavicular joint from direct trauma, osteolysis of the distal clavicle (mostly in weightlifters), and cervical clavicular injuries in the young thrower (6,230). Rotator cuff injuries remain less common in the younger athlete. Conservative treatment for musculoskeletal injury in children includes rest, ice, compression, and elevation (RICE) in addition to NSAIDs such as Telectin, naproxen (Naprosyn), and ibuprofen (Children’s Motrin, Children’s Advil). Appropriate equipment, coaching, recreation environments, and training often prevent sports injury, with safety remaining the primary consideration.
Osteochondritis dissecans is a condition resulting in partial or complete separation of a segment of normal highland cartilage from its supporting bone. Depending on the separation, cartilaginous or osteochondral intra-articular fragments may form (193). Mechanical symptoms may arise within the joint such as catching or locking. Although it has been more than 100 years since Konig (230) coined the term osteochondritis dissecans, the cause remains unclear. Five theories commonly suggested are ischemia, genetic predisposition, abnormal ossification, trauma, and cyclical strain (6). The condition most commonly affects the knee (lateral aspect of the medial femoral condyle in 70% of patients, lateral femoral condyle in 20%, and the patella in 10%) or can be seen in the elbow (11). Treatment of osteochondritis dissecans remains controversial. Intact lesions can often be treated symptomatically, with or without activity modification or immobilization (6). Free fragments often require surgical removal. Drilling techniques are commonly utilized and can help stimulate new bone formation healing and return of mobile bodies to their original donor sites (11). Long-term sequelae can be garnered in up to 25% with atypical lesions, older age, effusion, and larger lesions.
Chondromalacia of the knee needs to be distinguished from the more serious osteochondritis dissecans. Chondromalacia is a term used to describe anterior knee pain of undetermined cause in the younger athlete associated with softening of the articular cartilage beneath the patellar surface. The pain is frequently worse with squatting and climbing stairs, and is associated with a high-riding patella or malalignment. Patellar dislocations can occur in association and are usually lateral and associated with genu valgum, external tibial torsion, and general ligament dyslaxity. The subluxation of the patella is usually reducible, but can be painful. Exercises to strengthen the quadriceps, particularly the vastus medialis and the use of patella tracking braces, may be helpful. Surgical stabilization of the medial patellar tissues and lateral retinacular release can be helpful in more difficult cases.
Osteochondrosis is characterized by a disturbance in endochondral ossification, including both chondrogenesis and osteogenesis, in a previously normal endochondral growth region (6). The term osteochondrosis is preferred, as not all conditions are inflammatory, making the term osteochondritis inappropriate (193). Osteochondrosis is idiopathic and has been reported in nearly every growth center of the body, including apophyses, epiphyses, and physes. Their eponyms are generally named according to the region of the body and growth center involved (193). Most osteochondroses have well-defined natural histories and generally predictable outcomes (231). Freiberg’s disease involves collapse of the articular surface in subchondral bone, usually of the second metatarsal (232,233). Kohler’s disease involves irregular ossification of the tarsal navicular joint with localized pain and increased density. Freiberg’s disease is more common in girls between the ages of 12 and 15 years, whereas Kohler’s disease occurs in younger individuals age 2 to 9 years and is frequently reversible with conservative care including orthoses and casting. Apophysitis is relatively common at the knee, foot, and ankle, all secondary to traction overuse and microtrauma. Apophysistis at the inferior pole of the patella is called Sinding-Larsen-Johansson syndrome. Osgood-Schlatter disease involves apophysitis at the tibial tuberocity, and Sever’s disease involves apophysitis at the posterior calcaneus. These conditions generally occur around the age of 10 to 15 years of age, a few years earlier in girls, and are generally treated conservatively with the RICE protocol. Care should be taken not to overgeneralize treatment, however, as each condition can be different and require special attention. LaNec disease or ischial pubic synchondrosis, for instance, can be confused with a bone tumor if not careful and subsequently overtreated (193). Heel cups may be helpful with Sever’s disease in addition to short periods of casting and/or splinting. Stretching of the quadriceps and hamstrings can be helpful with Osgood-Schlatter disease in addition to knee sleeves or knee straps. NSAIDs are often prescribed as well. Pain-free strengthening of weight bearing soft tissues using more closed kinetic chain techniques may be best. Chondromalacia needs to be differentiated also from the osteochondroses in the young person with anterior knee pain. Chondromalacia is associated with softening of the cartilage beneath the patellar surface and often a high-riding patella or malalignment. The pain frequently gets worse with squatting and climbing stairs, and benefits with conservative treatment under the RICE protocol. Osteochondrosis of the vertebral end plate is known as Scheuermann’s disease. The incidence of Scheuermann’s deformities in the general population ranges between 0.5% and 8%, with an increased prevelance in males (6,234). It is distinguished from postural roundback by its more rigid structural characteristics. Symptoms are common during the early teenage years and in most instances decrease in late adolescence (11). When three or more consecutive vertebrae are wedged more than 5 degrees, radiographic criteria for Scheuermann’s disease are met (235). The radiographic picture includes irregular vertebral endplates, protrusion of disc material into the spongiosum of the vertebral body, Schmorl nodes, narrowed disc spaces, and anterior wedging of the vertebral bodies. The cause of Scheuermann’s disease again is unknown, but thought by some to fall within the spectrum of repetitive microtrauma and fatigue failure of the immature thoracic vertebral bodies. An increase in the incidence of disabling back pain in adults has been reported and may lead to surgery in this older age group (11,236). More severe pain is reported in patients with kyphotic deformities greater than 75 degrees. Cardiorespiratory conditions may occur in patients with severe deformities (kyphosis greater than 100 degrees). Atypical Scheuermann’s disease (237) or thoracolumbar apophysitis is named because it does not meet the usual radiographic criteria for Scheuermann’s disease established by Sorenson (238). This phenomenon is usually seen at the thoracolumbar junction and may be the pediatric equivalent of an adult compression fracture. There is a 2:1 male-to-female predominance, with a peak age of incidence between 15 and 17 years. When Scheuermann’s disease is associated with pain in the presence of one or more irregular vertebral bodies, physical exercise is prohibited. A thoracic lumbosacral orthosis (TLSO) or Milwaukee brace is used for more severe involvement. Sometimes bracing is required for three months to achieve pain control. Conservative care, including traditional RICE protocol, gentle flexibility routines, and NSAIDs, can be helpful. For correction of spinal deformity with bracing, a mobile kyphotic deformity is required in addition to at least a year of growth remaining in the spine (11). In most cases, brace treatment must be continued for a minimum of 18 months to have an effect on vertebral wedging. Severe involvement progressing to more rigid kyphosis, greater than 75 degrees, may require spinal fusion, both posterior and anterior (11).
Intervertebral disc injuries in children and the young athlete are uncommon (11). In contrast to the selective motor and sensory deficits often observed in adults with disc herniation, athletes under 20 years of age have pain and tenderness localized generally to the midline and, to a lesser extent, over the course of the sciatic nerve (239). Of surgically treated disc herniations, only 1% to 2% percent occurs in the pediatric population. Many of these children have underlying congenital anomalies, including transitional vertebrae, spondylolisthesis, and congenital spinal stenosis. Spondylolysis has never been found in the newborn. Its occurrence increases between the ages of 5.5 and 6.5 years to a rate of 5%, close to the frequency of 5.8% in the Caucasian population (240). The condition involves a fracture to the paras interarticularis and is more common in athletes involved with repetitive flexion-extension and hyperextension activities of the lumbar spine. Oblique radiographs of the lumbar spine show the classic “scotty dog” sign (241). A positive stork leg test with careful hyperextension of the lumbar spine is often present. Common sports associated with this condition are collisional in nature: gymnastics, weight lifting, and figure skating. Involvement is generally at the L5-S1 level, but can occur at other levels. In the absence of disc herniation or spondylolisthesis, radicular symptoms are uncommon. Treatment often consists of activity limits, stretching of tight hamstrings, and lumbar corsets or bracing in carefully selected individuals. Nuclear medicine bone scans can be particularly helpful in identifying these lesions and eventual healing, which can take up to nine months (242). The incidence of back pain in backpack users of school age has been noted in up to 74% of individuals (243). Heavy backpack use, female gender, and larger body mass index were all associated with back pain. Back pain from backpacks needs to be considered readily in all individuals, particularly those with spondylitic conditions and regular daily use (244). Spondylolisthesis, or slipping forward of the vertebral body, may occur during childhood, with a prepubital peak incidence and promoted by hyperlordosis. Grading of spondylolisthesis is according to the classification developed by Meyerding (245). The superior border of the inferior vertebrae is divided into four equal quadrants, with slips in each quadrant accounting for one grade. Surgical treatment is necessary in the presence of neurologic signs or forward slipping of the vertebral body beyond 50% of its width. Other apophyseal injuries in the spine include slipped vertebral apophysis or endplate fracture (246). This condition may mimic a herinated lumbar disc and is often associated with heavy lifting. Commonly, the inferior apophysis of L4 is displaced into the vertebral canal along with some attached disc material (11). Radiographs reveal a small bony fragment pulled off the inferior edge of the vertebral endplate. A CT scan or MR imaging reveals an extradural mass. Surgical excision can provide excellent relief of symptoms in those in whom conservative care has failed. Epidural steroids may be used for individuals in whom initial nonsurgical treatment is unsuccessful. Strains of the lower back are less common in children in view of the open iliac apophysis. Children with iliac apophysitis usually have a beltlike pain along the muscular attachments of the superior iliac crest (247). Lumbar interspinous process bursitis, or “kissing spines,” also needs consideration in the young patient, especially those participating in gymnastics or other activities involving hyperextension of the thoracolumbar spine.
Discitis is a rare condition (occurring in less than 1%) that also causes back pain in children (206). It can be divided into septic and aseptic types. Between the vertebrae, the notochord expands to form a gelatinous center of the intervertebral disc called the nucleus pulposis. This nucleus is later surrounded by circularly arranged fibers from sclerotome-derived mesodermal cells called the annulus fibrosis. The nucleus pulposis and the annulus fibrosis together constitute the intervertebral disc. The intervertebral disc is vascular in children up to 7 years. Around the age of 7, the disc begins to develop some of the end arteries common to the adolescent and adult. From the age of approximately 13 years, all end arteries are thought to be formed and thus, the disc becomes avascular. It may well be that the more vascular nature of the disc is a major reason why discitis occurs almost solely in children (248,249,250,251). Positive cultures are generally more common in younger children, with Staphylococcus aureus by far the most common finding (206). A slower, indulent form of discitis may develop in a child from brucellosis or tuberculosis. A skin test for tuberculosis may be helpful. Trauma might cause release from the disc tissue enzymes such as phospholipase A2, known to be a potent inflammatory simulator, which could, in theory, cause inflammation. Viral causes are also thought to be present and likely make up a substantial component of the aseptic variety. High fever, toxemia, elevated white blood cell counts, positive blood cultures, and bone scans in a child under the age of 3 who refuses to sit or stand is a common history. The diagnosis must be considered in a child with just mild illness who has abdominal pain or refuses to walk for unclear reasons. Pain frequently occurs at night, and children are usually not systemically ill (252). An MR imaging scan shows involvement of the disc space and vertebral bodies one level above and below. The two most serious diseases in the differential diagnosis include vertebral osteomyelitis, rare in children, and spinal tumors. Biopsy of the disc space may be necessary, particularly in an adolescent suspected of abusing drugs. Vancomycin may be the treatment of choice or other staphylococcal antimicrobials. When there is no response to early antibiotic therapy, aspiration or biopsy should be performed, followed by culture-specific antibiotic treatment (11). Immobilization of the child may or may not be helpful. Hematogenous spread is the most common cause of vertebral osteomyelitis, with Staphylococcus aureus the most common organism. Vertebral osteomyelitis generally involves the more anterior aspects of the spine and may be associated with paravertebral collections. Tuberculous spondylitis or Pott's disease remains common worldwide and is still seen in some neglected areas of the United States (253).
Gait abnormalities, although frequently benign, can be a great source of parental concern. The child's whole posture needs to be looked at carefully, particularly from the waist downward, because malalignment of any lower extremity joint may stem from another. Figure 14.11 shows anteversion of the femoral head and neck on the femoral diaphysis in addition to coxa valga and coxa vara. The normal angle of the femoral neck and shaft at birth is approximately 160 degrees and decreases to approximately 140 degrees at 5 years and 120 degrees at adulthood. At birth, the normal anterior femoral neck angle relative to the transcondylar line of the distal femur is approximately 40 degrees. This angle decreases to approximately 25 degrees by age 5 and 15 degrees in adulthood (254,255). An increase in the anteversion angle is frequently associated with in-toeing and increased internal rotation best assessed with the child lying prone. Figures 14.12 and 14.13 show normal degrees of internal and external rotation throughout the lifetime within two standard deviations. The degree of femoral neck anteversion is generally thought to be
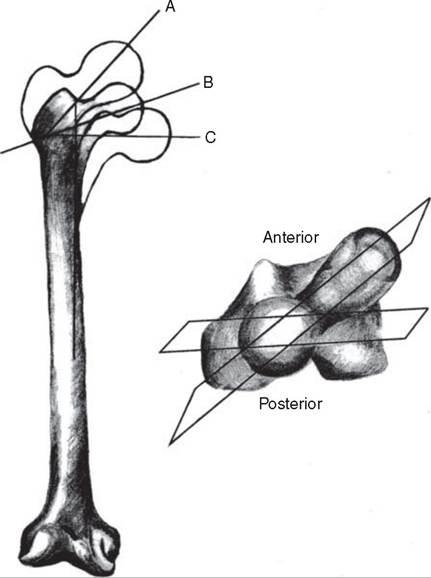
Figure 14.11 Angle of neck shaft and anteversion of the femur: (A) increased, coxa-valga, (B) mormal, (C) decreased coxa vara. The smaller diagram shows a top view relating a plane from left to right through the greater trochanter and femoral head referenced to the transcondylar femoral axis distally.
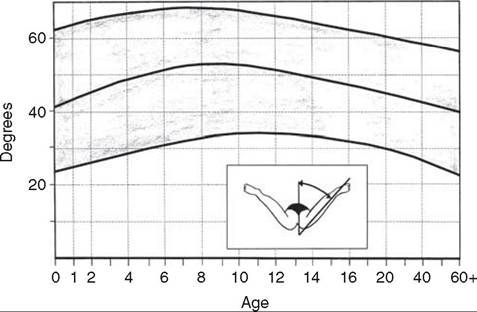
Figure 14.12 Hip internal rotation assessed with the child prone. Normal ranges are shaded. (Adapted from Ref. 256 with permission.)
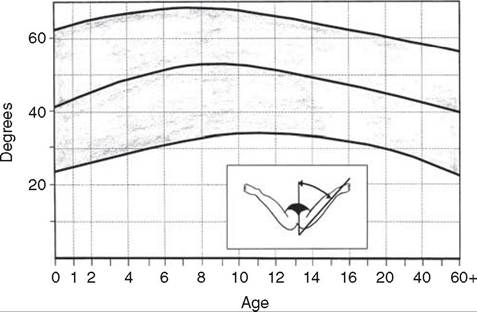
Figure 14.13 Hip external rotation assessed with the child prone. Normal ranges are shaded. (Adapted from Ref. 256 with permission.)
about 20 degrees less than full internal rotation of the hip (6). An estimate of anteversion can be measured by trochanteric palpation with the child prone on the examination table. The degree of internal rotation measured at the point where the greater trochanter is most prominent on the lateral surface of the hip is the estimate of anteversion. In-toeing may persist into adulthood, but often improves with time in the physically normal child by the age of 8. Exercises to strengthen the external rotators of the hip and physical and verbal cues to out-toe and compensate may, at times, offer benefit. This benefit is achieved through facilitating motor memory and improved compensatory strategy to increase out-toeing and not the result of any change in the bony anteversion. Severe intoeing not correcting over time, associated with falls and significantly limited external rotation, can be corrected surgically. Surgery is deferred at least beyond the age of 6 years and frequently after 10 years, when there is less chance of postoperative derotation of the surgically corrected torsion. Surgery should not be taken lightly, and good indication should be present along with well-educated parents and child to justify the risk.
Excessive hip external rotation with minimal internal rotation, often tested with the child lying prone with hip extended (see Fig. 14.13), is associated with femoral retroversion (opposite of anteversion). This condition can be seen more common in children with low tone and increased joint laxity, such as those with Down's syndrome and Ehlers-Danlos syndrome. Gait is with excessive out-toeing, and familial traits may be present. Most rotational variations in children resolve spontaneously with time and minimal intervention (257,258). Careful examination is required to exclude more serious disorders.
Tibial torsion, both internal and external, may occur as compensation for the femoral version or by
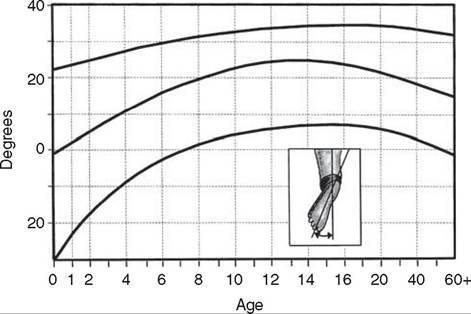
Figure 14.14 Rotational status of the tibia assessed by evaluating the child in the prone position. Foot placed in plantigrade neutral position. (Adapted from Ref. 256 with permission.)
themselves, causing in-toeing and out-toeing. The transmalleolar axis may be palpated in prone and knee-flexed positions. The lateral malleolus is approximately 5 to 10 degrees posterior to the medial malleolus in the toddler and increases to approximately 15 degrees by adolescence (259). Figure 14.14 (256) shows the normal degree of thigh-foot angle over the lifetime within two standard deviations. Dennis-Brown bars have been found to have essentially no effect in altering tibial torsion and have generally fallen into disuse for this condition (6). In measurement of the thighfoot angle, the foot is placed into the plantigrade and hindfoot neutral position with palpated talonavicular alignment. This helps eliminate other, more intrinsic foot conditions, such as metatarsus varus and adduc- tus, that can otherwise confound the thigh-foot angle measurement. Figure 14.15 shows normal foot progression angle over the lifetime (256). All rotational abnormalities of the lower extremities have influence on the
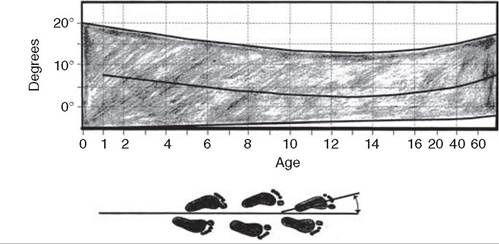
Figure 14.15 Foot progression angle. Normal ranges shaded. (Adapted from Ref. 256 with permission.)
foot progression angle. Flat feet, or pes planus, is no exception. Flexible pes planus is usually asymptomatic, at least in earlier years, and more common than its rigid counterpart in children. Inexpensive scaphoid pads or medial inserts may help to create more plantigrade weight bearing and improve foot progression angle, but they do not correct the deformity. Extreme cases such as in children with hypotonia may require surgery after the age of 5 years in the form of calcaneal lengthening once bony cortices are more solid. Untreated progression with increased foot progression angle may occur along with compensatory hallux valgus, planovalgus, and secondary bunion and toe deformities. Pes planovalgus is associated with more active or shortened peroneal musculature, progressing over time, with the development of pain particularly in later years. Rigid pes planus is a congenital deformity associated with other anomalies in 50% of cases, as discussed earlier in this chapter.
Angular deformities of the femoral-tibial alignment are also a source of frequent concern for parents and families. At birth, the infant has a bowlegged posture with a genu varum of 10 to 15 degrees (260,261). The bowing gradually straightens so that the femoral- tibial alignment is neutral or 0% by 12 to 18 months of age (6). Continued growth results in a peak valgus angulation of 12 to 15 degrees by the age of 3 to 4 years (11). Subsequent growth reduces the genu valgum to normal adult values of approximately 5 to 7 degrees by the age of 12 years. At any age there is a fairly wide standard deviation of normal (256). Figure 14.16 shows the normal variation of valgus and varus at the knee up through adulthood values (256). Measurements between the medial and femoral condyles or intermal- leolar distance help to quantitate the deformity (256). The most common cause of genu varum in children is physiologic bowlegs. Children with this condition have genu varum that persists after the age of 18 months, usually resolving before the age of 3 years. X-rays show symmetric growth plate anatomy and medial bowing that involves the proximal tibia as well as the distal femur. Measurement of the metaphyseal-diaphyseal
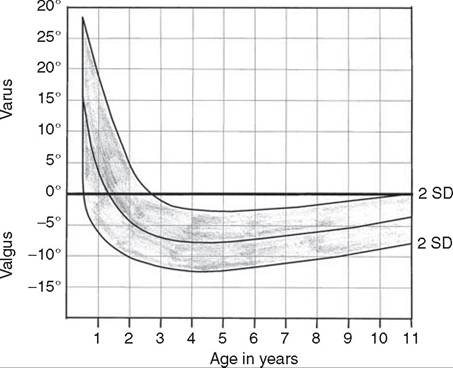
Figure 14.16 Normal values for knee angle measured in valgus and varus. (Adapted from Ref. 256 with permission.)
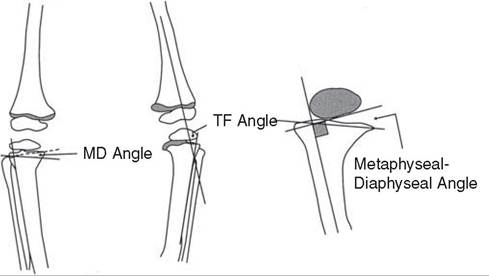
Figure 14.17 Measurement of metaphyseal-diaphyseal angle and tibiofemoral angle.
angle in addition to the tibiofemoral angles is helpful in the differential diagnosis (Fig. 14.17) (262,263,264). The differential diagnosis includes infantile tibia vara or Blount's disease, hypophosphatemic rickets, metaphyseal chondrodysplasia, focal fibrocartilagenous dysplasia, and trauma to the epiphysis. Blount's disease occurs in children with no apparent abnormality at birth, having a typical history of genu varum worsening with gait before the age of 2 years. The less frequent juvenile onset may occur between 4 and 10 years and the adolescent form over 11 years. The condition is more frequent in African Americans and girls, and is seen with obesity and in children walking at an early age (265). The condition is also more common in certain geographical locations such as the southeastern part of the United States (193). Classic radiographic changes associated with Blount's disease and tibial varum are seen in the Langenskiold classification (266). Blount's disease is believed to result from abnormal compression of the medial aspect of the proximal tibial physes, causing retardation of growth in that area or increased growth laterally of the proximal tibia or fibula (6,267). In juvenile Blount's disease, the etiology is less clear and may relate more to malalignment, leading to the characteristic changes visible on radiographs. Patients with metaphysial-diaphysial angles greater than 16 degrees have been reported to experience progression of the angular deformity (268). Early and continuous bracing in Langenskiold stage I and stage II disease (266) can achieve good results (11). Bracing should not be initiated after 3 years of age, nor should brace treatment be continued if Langenskiold stage III changes develop (269,270). The authors' preference is a medial upright knee ankle foot orthosis (KAFO) with valgus promotion padding through the center of the knee axis and free-swinging knee and ankle. Modified KAFOs preventing knee flexion have also been promoted (6). Proximal valgus osteotomies may be required for severe persistent angular deformity after the age of 3 years, along with consideration of Ilizarov techniques (11). Stapling of the lateral physis (often both tibia and femur) are also considerations, particularly in the adolescent prior to cessation of growth. Increased fragmentation, declination, and beaking of the medial-proximal epiphysis generally indicate the need for surgery. Surgical complications can include compartment syndrome with persistent neurovascular compromise. Careful postsurgical follow up of the child is required to prevent unnecessary over- or undercorrection. Graphs for timing of hemiep- iphysiodesis are available and can be helpful in experienced hands (271).
Genu valgum, or “knock-knees,” is a concern in children who are developing peak valgus alignment around the ages of 3 to 4 years. Almost 99% of the time, this valgus is benign in nature, correcting toward adult values by early adolescence. X-rays show symmetric growth plates with no particular abnormalities. Observation is the treatment of choice in these individuals. Children who have genu valgum with a femoral- tibial angle greater than 20 degrees require follow-up, but generally the problem resolves spontaneously. If abnormal genu valgum persists into the teens, correction by hemiepiphysiodesis or stapling of the medial physis may be effective (11,272). Staples that are placed extraperiosteal for varus or valgus deformity allow for growth to resume once removed. Rebound phenomena can be anticipated, undoing some of the corrected valgus or varus. Overcorrection slightly in anticipation of this problem, especially in children under the age of 12, needs to be considered (193).
Idiopathic toe walking is a common condition in children under 3 years of age. By 3 years of age, children should walk with a heelstrike (273,274,275). Persistent toe walking beyond this age is abnormal (6). Little is known about the natural history of idiopathic toe walking, with most individuals improving or showing resolution prior to the age of 6. Persistent toe walking in the older child and young adult can result in leg pains, more activity-related, and frequently in the anterior tibial or knee regions. Toe walking can diminish or cease with time, as body mass becomes too large to be supported by the triceps surae or as a result of secondary development of external tibial torsion (276). Toe walking developing sometime after birth can be associated more with problematic conditions, such as muscular dystrophy, dystonia, tethered cord syndrome, central nervous system neoplastic processes, or autism (277). A family history is often positive along with that of prematurity and a slight male predominance (277).
Leg pains in children are generally benign, but need to be followed carefully for signs of progression or persistence despite conservative care. Conservative care, generally involving the RICE protocol, NSAIDs, and warm baths and massage, often relieves most of the discomforts. A pattern of increased pain with activity or recreational pursuits is common. If improvements are not noted within a few weeks of conservative care, additional workup is required to rule out other, more concerning etiologic entities. Workup should include radiographs, hematology and metabolic parameters, erythrocyte sedimentation rate (ESR), possible nuclear medicine scan, and Lyme's disease titre along with other rheumatologic markers.
In children who toe walk, walking is generally not delayed as a developmental milestone, and when this occurs, conditions like spastic diplegia should be considered. A few beats of clonus at the ankle can be helpful in differentiating associated mild diplegia from idiopathic toe walking. Nonoperative treatment, including heel cord-stretching routines with the calcaneus midline or inverted, can be helpful when performed on a regular basis along with dorsiflexionstrengthening exercises. Stretching a tight heel cord with the hindfoot in valgus can contribute to midfoot breakage while being ineffective in lengthening plantarflexion soft tissues. Articulating AFOs with plantarflexion blocks or posterior leaf-spring types can be helpful in maintaining position both day and night. Serial casting can be an option for resistant equinous deformity not felt to be surgical at the time. Casting should occur with maximal dorsiflexion as tolerated, again with the heel in a neutral or slightly inverted position. Two or three sets of short-leg casts of the walking nature, lengthening the heel cord, can result in greater passive dorsiflexion. Short-term weakness of the anterior tibialis and dorsiflexors can be anticipated postcasting requiring additional strengthening intervention. Clostridium botulinum toxin A injections can be helpful also in weakening partially the plantarflexors, facilitating improved stretch into dorsiflexion along with relative strengthening of active dorsiflexion. Orthotics can be weaned over three to six months once toe walking has resolved and improvements obvious. Nighttime splinting can be discontinued in the absence of recurrent toe walking. Surgical intervention, including heel cord lengthening and/ or gastrocsoleus recession, is reserved for those who have failed conservative trial. Toe walking after the age of 6 years often does not improve, and heel cord contractures can worsen (6). External tibial torsion can progress further developing as compensation for lack of foot-flat contact. The torsion may be severe enough with excessive external foot progression angle to warrant corrective osteotomy. Surgical lengthening is performed sufficient to obtain 10 degrees of dorsiflexion with the knee extended (6,11). Overlengthening of the heel cord can be disastrous, resulting in persistent crouched gait and associated pain syndromes and limitations. In more severe and chronic equinous deformities, posterior ankle capsular release may be required. Short-leg casting postoperatively is common up to six weeks followed by custom-molded AFOs for up to two months thereafter. Home exercise, along with physical therapy for gentle heel cord stretching and strengthening ankle dorsiflexion, is mandatory or recurrent equinous deformity can be anticipated. Long-term outcomes of surgical lengthening in skilled hands are generally positive when recommendations are followed with satisfactory heel-toe walking over the lifetime (278,279).
More on the topic DEVELOPMENTAL CONDITIONS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- FIVE COMPONENTS OF LEGAL COMPETENCIES
- Unto This Last and Criticism of Economics
- Foreword: Frances Moore Lappe
- Reviewers
- The Netherlands and the UK: The Witteveen Reports and their contradictory results
- REVIEW OF FORENSIC ASSESSMENT INSTRUMENTS
- Diagnosis of Bovine Tuberculosis in Zambia
- Legal Aid and the Bar, from Symbiosis to Parasitism
- THE THEORY AND PRACTICE OF EMPIRE-BUILDING