PEDIATRIC ADVANCED LIFE SUPPORT (PALS)
Pediatric advanced life support (PALS) is a more organized approach than BLS towards the evaluation and management of CPA, before, during and after the arrest. Unlike sequential actions in BLS, resuscitative measures in PALS are applied simultaneously and concurrently, as it usually takes place in hospital environment with many rescuers and technological support.
Pediatric chain of survival includes 6 components— (1) early recognition and prevention of cardiac arrest, (2) activation of emergency response, (3) high quality cardiopulmonary resuscitation, (4) advanced resuscitation, (5) post-arrest care, and (6) recovery.
Important components of PALS include—(1) basic life support, (2) use of equipments and techniques to establish and maintain oxygenation, ventilation and perfusion, (3) clinical and ECG monitoring for arrhythmia and management, (4) establish and maintain vascular access, (5) identify and treat reversible causes of cardiopulmonary arrest, (6) emergency treatment of cardiac and respiratory arrest, and (7) treating patients with trauma, shock, respiratory failure and other prearrest conditions.
While important aspects of these components have been discussed here sequentially, PALS involves concurrent efforts on all fronts, as follows:
A. Initial assessment: Most cases requiring PALS are already in hospital, under constant monitoring and usually deteriorate gradually. Cases with acute CPA are usually managed by BLS, discussed earlier, before transfer to the hospital. Hence, it is often possible to anticipate the need for resuscitation in these cases, based on clinical and laboratory assessment.
Initial assessment about the need and strategy of the resuscitation largely depends on five vital parameters, often termed as ABCDE, i.e. Airway, B reathing, Circulation, Disability in terms of neurological functions and Exposure or visual search for bodily injuries.
A quick history at this stage also helps to look for special danger signs and decide course of resuscitation. Important pointers towards the need of PALS usually relate to signs of:• Airway obstruction, e.g. stridor, poor chest expansion or breath sounds, etc.
• Respiratory failure, e.g. tachypnea, dyspnea, grunt, cyanosis, apnea/gasp, etc.
TABLE 27.1: Normal range of vital signs in children
*Lowest of the range for systolic/diastolic BP.
• Circulatory failure, e.g. tachycardia, cold extremities prolonged capillary refill time, weak pulse, hypotension, etc.
• Neurological dysfunction, e.g. altered sensorium, dilated and slow-reacting pupils, flaccid tone, decerebrate/decorticate posture, etc.
Table 27.1 provides acceptable ranges for normal vital signs, i.e. heart rate (HR), respiratory rate (RR) and blood pressure (BP), at various ages, to identify the need for intervention. However, three simple rules are:
• RR should never by gt;60/minutes for sustained period.
• HR should never be gt; 3 times of RR.
• BP should never be lt;60 mm Hg in newborns, lt;70 mm Hg in infants, lt; 70 + (2 x Age) in 1-10 years age or lt;90 mm Hg in older children.
B. Effective airway maintenance, may require—
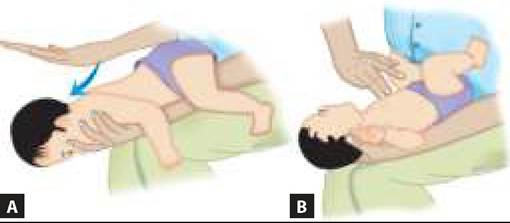
(a) correct positioning, as discussed previously under BLS, (b) airway suction, (c) Oro-/naso-pharyngeal airways, or (d) endotracheal intubation/Tracheostomy. The fact that pediatric airways differ from adult airways on several aspects (Table 27.2) has led to evolvement of specific PALS guidelines, which should be followed meticulously during respiratory resuscitation. Some important considerations in airway maintenance are as follows, while procedural/instrumental details are discussed in Ch 32.4.
Airway suction in older children requires use of a portable foot-operated/electric suction machine or central suction system. Oral mucus extractors are not much effective beyond the neonatal period.
A sterile/TABLE 27.2: Anatomical peculiarities of pediatric airway
• Smaller airway diameter, easily blocked by edema/mucus
• Large tongue with risk of posterior displacement and airway block
• Relatively cephalad larynx with acute angle between tongue base and glottic opening*
• Short-narrow epiglottis at sharper angle with trachea*
• Lower anterior attachment of vocal cords*
• Funnel-shaped larynx, narrowest below the vocal cord at the level of non-distensible cricoid cartilage*
*Leading to intubation difficulties
disposable flexible suction catheter of Fr 8 (Fr 5 or 6 in newborns lt; 3 kg) is preferable and less traumatic, except to remove thick secretions or particulate matter by rigid catheter. Important consideration during suction are:
• Optimum suction force should be ~80-120 mm Hg (vs ~30 mm in newborns),
• Suction time should not exceed gt;5 seconds at one attempt. Intermittent O2 supplements are necessary between multiple attempts to prevent hypoxia.
• Heart rate should be monitored to detect significant bradycardia, due to vagal stimulation.
Important complications of suction are—(a) oral mucosal trauma, (b) nosocomial infection and rarely, (c) sudden CPA due to vagal stimulation.
Airways: Different devices used to maintain patency of airways include:
Oropharyngeal airway is a curved rubber device to prevent glossoptosis and ensure clear airway/suction channel (Fig. 32.10). Proper size may be estimated by placing its flange at the corner of mouth, when tip should reach the angle of mandible. It should not be used in a conscious child.
Nasopharyngeal airway is a short disposable rubber/ plastic tube, better tolerated in conscious patients, though not used frequently. It is inserted via nostrils with proper length being the distance between tip of the nose and tragus. Use of fabricated nasal airways by cutting an endotracheal tube, should be avoided due to risk of accidental slippage beyond nares, unless an adapter is used.
Laryngeal mask airway (LMA) may be used to ensure patent airway and support ventilation, only if Bag and Mask Ventilation is unsuccessful and Endotracheal intubation is not possible. However, difficulty in its placement and higher incidence of complications precludes use of LMA in young children.
Endotracheal intubation is indicated in presence of—(a) airway obstruction, (b) poor response to bagmask ventilation, (c) need for mechanical ventilation. Important considerations in endotracheal intubation are:
• A sterile endotracheal tube of proper size (uncuffed tubes of 2.5-3 in preterms, 3-3.5 in term newborns, 3.5-4 mm in infants and 4+(age/4) in older children) should be inserted under laryngoscopic visualization to the desired depth from alveolar margins (Age/2+12; in cm) up to mid-trachea.
• Despite the lower risk of aspiration, cuffed endotracheal tubes are rarely used in children as normal anatomically-narrow cricoid cartilage itself provides a functional cuff. If used, size should be 0.5 mm less than uncuffed tubes.
• A straight laryngoscopic blade (Miller type) is preferred in infants/young children, while curved blade (MacIntosh type) is preferable gt; 8-10 years.
• IPPV with 100% oxygen via bag/mask should be given before and between intubation attempts, to prevent prolonged hypoxia. Each intubation attempt should not last for gt;30 second. Baby should be constantly monitored for bradycardia and cyanosis/ pallor to prevent severe hypoxia.
• Post-intubation, the tube should be secured and its position and patency should be checked frequently to ensure adequate bilateral air-entry in lungs by auscultation. Position of the tube may also be checked by chest skiagram and ETCO2 monitoring. Pulse oximetry is unreliable as SaO2 may not decline for over 3 minutes, even without effective ventilation. Repeated suction are required to maintain tubal patency.
• If an intubated patient's condition deteriorates consider Displacement of the tube, Obstruction of the tube, Pneumothorax or Equipment failure (DOPE).
• For Endotracheal suction, catheter should not be inserted beyond the tip of endotracheal tube.
Tracheostomy is indicated in children with airway obstruction or difficult intubations, using a disposable tracheostomy tube. It serves the same purpose as intubation, with an added advantage of reducing dead space. However, disadvantages, e.g. infection, tracheal injury and subglottic stenosis, should be considered before tracheostomy decision.
C. Effective ventilatory support depends on the status of spontaneous breathing efforts and include: (a) oxygen supplementation in children with adequate spontaneous breathing, and (b) manual (Bag and mask) or mechanical ventilatory assistance in cases with absent/feeble breathing efforts.
Some important considerations in ventilatory support are as follows, while procedural and equipmental details are given in Ch 31.4 and 27.2.
Oxygen therapy aims to deliver 100% oxygen during the resuscitation till circulation is established, and then to raise O2 content in inspired air (FiO2) to maintain PaO2 gt;60-70 mm Hg or SaO2 gt; 94%, via: (a) low-flow devices, e.g. nasal catheters, prongs or face-masks, (b) high-flow devices, e.g. face-tents or oxygen-hoods, and (c) bag/mask ventilation.(Ch 32.4)
Efficacy of these devices varies according to the oxygen flow rate and amount of mixing with expired/ environmental air (Table 27.3).
Direct nasal devices are simple but least effective, potentially traumatic and cannot be used to deliver a flow rate of gt;2-4 L/minute due to nasal irritation. 100% oxygen can be truly delivered only by mechanical ventilation via endotracheal tube, though fairly high FiO2 (gt;60-80%) may be achieved in spontaneously breathing child, by high-flow delivery (gt;10 L/minute) via face masks with reservoir/re-breathing bag.
TABLE 27.3: Common oxygen delivery devices
| Device | Flow (L/min) | FiO2 |
| Nasal cannula | 2-4 | 20-40% |
| Simple mask | 4-6 | 30-40%’ |
| Venturi mask | 6-10 | 40-60% |
| Face tent | 10-12 | ~40% |
| O2 hood/tent | 10-12 | ~80% |
| Bag-mask | Adjustable | 100% |
*up to 60-70%, if tight-mask and reservoir is used
Reservoir is a bag attached to the face-mask, which collects initial O2-rich portion of exhaled air that remains in upper airways.
During next breath, it is mixed with fresh oxygen, to enrich inspired air. Continuous pulse oximetry to monitor SaO2 is advisable during CPR (Ch 27.4.4), in all cases.Bag and mask ventilation (Manual resuscitator) is a simple method to deliver high-oxygen concentration, specially in children with inadequate breathing efforts till mechanical ventilation is arranged or during transport.
Common AMBU bag (Ambulatory manual breathing unit) may be used to deliver—(a) continuous positive airway pressure (CPAP) ventilation by maintaining a constant pressure of ~5-10 cm H2O over bag, or
(b) intermittent positive pressure ventilation (IPPV) by active deflation, followed by self-inflation. Important considerations in bag-mask ventilation are as follows, while procedural/equipmental details are given in Ch 32.4.
• Proper supine position with slightly hyperextended neck (head-tilt, chin-lift) to keep the airway open.
• Proper-size, Snuggly-fitted face-mask, to minimize dead space and rebreathing of exhaled air.
• Proper-size resuscitation bag (450-1000 ml), to deliver a tidal volume of ~10-15 ml/kg.
• Proper pressure on the resuscitation-bag, just to raise the chest visibly but never to exceed 35-45 cm H2O, except during initial resuscitation. Excessive pressure not only risks barotrauma but also impedes systemic venous return due to high intrathoracic pressure, thus reducing cardiac output and cerebral and coronary blood flow.
• Proper rate of 2 breaths/15 chest compressions during CPR and ~12-20 breaths/minutes post-CPR, with an inspiratory time of ~1 second/breath.
• Frequent check on air-entry into lungs and clinical signs to ensure adequate ventilation.
A self-inflating resuscitation bag (without oxygen source) delivers ~20% of FiO2, which may be increased to ~30% if an oxygen source with a flow rate of ~10-12 L/min is connected; and ~60-80% if oxygen source as well as oxygen reservoir is connected. 100% oxygen can be delivered only if resuscitation bag is connected to endotracheal tube, instead of face mask.
Two-person bag and mask ventilation, with one rescuer maintaining the open airway with a jaw-thrust and tight mask-to-face seal and the other compressing the ventilation bag, is more effective than single-person method.
Main complication of bag and mask ventilation without endotracheal tube is gastric distension gt; regurgitation gt; aspiration, which can be minimized by inserting a nasogastric tube or Sellick maneuver (pressure on cricoid cartilage to occlude proximal esophagus).
Bag and mask ventilation is contraindicated in—
(a) diaphragmatic hernia, or (b) suspected kerosene poisoning, where endotracheal intubation is mandatory, which may be attached to resuscitation bag.
Mechanical ventilation is indicated in children with established respiratory failure with specific indications, discussed in Ch 27.2.
D. Adequate vascular access: A reliable venous access is the crucial step in PALS, though temporary intraosseous route may be used for emergency fluid and drug administration, if venous access is not achieved in three attempts or 90 seconds (see Ch 32.3).
While central venous access is more secure for longterm use and to deliver irritant medicines, e.g. calcium, placement of central venous catheter is time consuming and needs experience, hence, not recommended as the initial route of vascular access in an emergency (also see Ch 27.4.3).
Some lipid-soluble drugs, e.g. adrenaline, atropine, naloxone, lidocaine, etc. may also be given intratracheally before IV access is obtained, in doses 10 times (for adrenaline, for others 2-3 times) of IV dose, diluted up to 5 ml of normal saline. Each intrathecal administration should be followed by 5 manual ventilations to ensure adequate absorption.
Lipid-insoluble drugs, e.g. sodium bicarbonate and calcium may injure the airway and should not be administered via endotracheal route.
E. Effective circulatory support: Circulatory insufficiency is an integral component of CPA and all children after initial ventilatory resuscitation should receive 20 ml/kg of IV ringer lactate or normal saline, before definitive assessment and treatment of shock (Ch 27.3). Dextrose- solutions should not be used for initial resuscitation, except in suspected/documented hypoglycemia, as they are poor volume expanders and may cause hyperglycemia and consequently, diuresis.
F. Monitoring: Constant monitoring is essential component of PALS for timely therapeutic decisions and includes: (a) clinical assessment of biophysical parameters, e.g. HR, RR and efforts, BP, and (b) relevant laboratory investigations, e.g. Blood sugar, ABG and electrolytes. Real-time non-invasive monitors, e.g. pulseoximeter, have revolutionalized constant monitoring during PALS (Ch 27.4.4).
G. Treatment of complications: Three important and potentially fatal immediate consequences of CPA are: Respiratoryfailure, Shock and arrhythmia, of which first two are discussed in later chapters. Common medications used to manage these complications have been listed in Table 27.4.
Arrhythmias may develop during or immediately after CPR, usually due to 6Hs (Hypoxia, Hypovolemia, Hypokalemia, Hyperkalemia, Hypoglycemia and Hydrogen ions, i.e. acidosis) or 5Ts (Trauma, Toxins, Temponade, Thrombosis and Tension pneumothorax), apart from drugs used in resuscitation. Although discussed in detail elsewhere (Ch 17.10), some important aspects of the management for common arrhythmias are as follows:
• Bradycardia or bradyarrhythmias are common rhythm abnormalities just before the arrest, which may prevent adequate circulatory resuscitation. Specific management involves chest compressions once the HR drops lt; 60/min with poor perfusion, followed by Adrenaline in non-responders (IV


Fig. 27.11: Management algorithm: Cardiac arrest in children.
Based on AHA/AAP guidelines 2020.
0.1 ml/kg of 1:10,000 solution or IT 0.1 ml/kg of 1:1000 solution, repeated every 3-5 min) except in heart block or excessive vagal tone. Bradycardia due to vagal overtone is best treated with atropine (IV 0.02 mg/kg). Correction of causative factors is equally important.
• Tachyarrhythmia may originate in sinus node, atria (narrow-complex) or ventricles (wide-complex) and differentiation is important for management decisions. No specific treatment is required for sinus tachycardia except close monitoring. Supraventricular tachycardia needs immediate vagal maneuvers, followed by rapid 'push' adenosine infusion. Ventricular fibrillation or pulseless ventricular tachycardia develops in ~10% cases of pediatric CPA, which needs immediate defibrillation, along with simultaneous correction of causative factors.
• Pulseless electric activity (PEA) is a precursor of asystole, characterised by positive ECG activity without pulse or audible heart beat, also termed electro-mechanical dissociation. Treatment of PEA is same as that for asystole.
Recognition and Treatment of Cardiac Arrest
Unlike adults, cardiac arrest in children is usually due to non-cardiac causes, e.g. asphyxia, though some cases may develop acute CPA due to arrhythmias specially ventricular fibrillation.
High-quality CPR with effective chest compressions and breathing support, as discussed under BLS, is the key of management in these cases, along with emergency defibrillation in cases with shockable rhythm, i.e. ventricular fibrillation on ECG or cardiac monitoring.
Defibrillation in children requires two appropriate size paddles (8-10 cm, above 10 kg weight), one over the right upper chest and another over apex of the heart. Initial dose in children is 2 J/kg, which may be doubled in unsuccessful cases (Max 10 J/kg). After three failed attempts, child should receive epinephrine and CPR for 30-60 seconds before next effort, while amiodarone (IV 5 mg/kg bolus) or lidocaine (IV 1 mg/kg bolus) may be used after subsequent attempts.
Figure 27.11 provides an algorithm for resuscitation of a child in cardiac arrest, as per American Heart Association guidelines.
27.2