ACUTE RESPIRATORY FAILURE
Acute respiratory failure (ARpF) may be defined as - quot;a state of inadequate pulmonary functions to maintain adequate O2 supply and CO2 elimination' usually denoted by PaO2 lt; 60 mm Hg on room air and/or PaCO2 gt;50 mm Hg.quot; Depending on the course, ARpF may be sudden or superimposed on chronic respiratory insufficiency.
Pathophysiology: Gaseous exchange in the lungs depends on three major functions—ventilation, perfusion and diffusion of gases. ARpF may develop due to abnormalities of any one or more of these functions, unless compensated by other components.
In children, capacity for this compensation is limited due to various developmental handicaps, e.g. (a) higher airway resistance, (b) poor chest wall compliance,
(c) lesser lung volume, and (d) higher oxygen requirements (6-8 ml/kg vs. 3-4 ml/kg in adults).
Depending on the primary pathology, ARpF may be classified as:
a. Type Ifailure (hypoxemic), due to impaired diffusion/ perfusion, predominantly characterized by hypoxia (PaO2 lt; 50 mm Hg), with/out hypercarbia,
b. Type II failure (hypoxemic-hypercarbic) due to impaired ventilation, predominantly characterized by hypercarbia (PaCO2 gt;50 mm Hg), though hypoxemia is almost also present.
Note that the tissue hypoxia may also develop despite adequate pulmonary functions due to circulatory insufficiency (CCF, shock) or poor oxygen carrying capacity of blood (anemia). Hence, a normal PaO2 does not guarantee adequate tissue oxygenation.
Etiology: Ventilatory insufficiency due to airway obstruction is the predominant cause of ARpF (Type II) in children, followed by intrinsic lung diseases (type I). Common causes of respiratory insufficiency and failure are listed in Table 27.5.
Clinically, important indicators of ARpF are:
a.
Signs of respiratory distress, e.g. tachypnoea, dyspnoea, grunt, cyanosis or apnea.b. Signs of cerebral hypoxia, e.g. restless/drowsiness, headache, convulsions, coma.
c. Signs of circulatory compensation/failure, e.g. tachy-/ bradycardia, hypo-/hypertension, diaphoresis and terminal cardiac arrest.
d. Signs of primary disease, e.g. stridor, wheeze, lung signs, signs of bulbar palsy, etc.
Diagnostic evaluation: Confirmation and monitoring of ARpF revolves around the arterial blood gas (ABG) analysis
TABLE 27.5: Causes of acute respiratory failure
Primary ventilatory failure (Type II ARpF)
• Upper airway obstruction
- Intrinsic: Malformations, croup, foreign body
- Extrinsic: RPA, vascular rings, mediastinal mass
• Pleural: Empyema, pneumothorax, effusion
• Restrictive lung: Diaphragmatic hernia, scoliosis
• Neurological disorders
- Central: CNS infections, head injury
- Neuromuscular*, GBS, poliomyelitis
Primary gaseous exchange failure (Type I ARpF)
• Lower airway obstruction: Asthma, bronchiolitis
• Intrinsic lung disease: Pneumonia, atelectesis,
• Impaired perfusion: Pulmonary edema, shock-lung GBS: Guillain-Barre syndrome; RPA: Retropharyngeal abscess *due to diaphragmatic or bulbar palsy
TABLE 27.6: ABG analysis in acute respiratory failure
* due to hyperventilation
that provides valuable information regarding not only the blood-gas status but also of acid-base balance (Table 27.6). Noninvasive monitoring techniques for ventilatory status, e.g. pulse oximetry (SaO2) and end tidal CO2 (EtCO2) have revolutionized management of ARpF.
Other investigations in ARpF are necessary to assess the: (a) etiology, e.g. chest X-rays, (b) oxygen carrying capacity of blood, e.g. hemoglobin levels, and (c) extent of hypoxic damage, e.g. serum electrolytes, renal/liver function tests and coagulation profile (DIC is common).
Management of ARpF aims to ensure adequate air entry, alveolar ventilation, gaseous diffusion and oxygen carrying capacity of blood to deliver adequate O2 at tissue levels and eliminate excess CO2. It requires highly- skilled intensive care and includes:• Initial clinical evaluation for
- Spontaneous breathing efforts
- Air entry into chest
• Ensuring airway patency by.
- Positioning
- Oro-/naso-pharyngeal airways
- Airway suction
- Endotracheal intubation/tracheostomy
• Oxygen delivery via.
- Direct nasal cannula/catheter
- Via face mask or oxygen tents
• Ventilatory assistance by.
- Mouth-to-mouth (rescue) breathing
- Bag and mask ventilation
- Mechanical ventilation
• Continuous clinical and blood gas monitoring
• Treatment of primary cause
• Management of hypoxic tissue damage
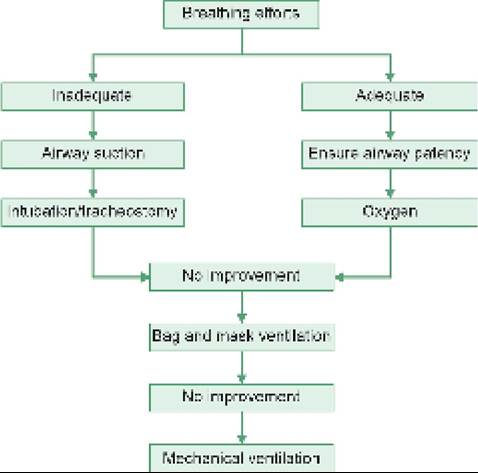
A schematic approach towards management of established or impending ARpF is given in Fig. 27.12. While emergency measures, e.g. airway maintenance, oxygen supplementation and manual ventilator assistance are discussed in previous chapter, most cases ultimately require mechanical ventilation.
Mechanical Ventilation
While detailed description of modalities for mechanical ventilation is beyond the scope of this book, some important considerations are as follows:
Fig. 27.12: Schematic management plan in ARpF.
TABLE 27.7: Indications for mechanical ventilation
• Prolonged apnea or need for bag and mask ventilation
• PaCO2 gt; 55 mm Hg
• PaO2 lt;60 mm Hg on 60% FiO2
• Persistent cyanosis on 60% FiO2
• Severe acidosis: pH lt;7.2
TABLE 27.8: Types of mechanical ventilation
• Controlled mechanical ventilation (CMV)
- Intermittent positive pressure ventilation (IPPV)
- Positive end-expiratory pressure ventilation (PEEP)
• Synchronized intermittent mechanical ventilation (SIMV)
• Spontaneous mechanical ventilation, e.g.
CPAP• Newer modalities (see text)
CPAP: Continuous positive airway pressure ventilation
Indications: Mechanical ventilation is indicated in children with persistently poor breathing efforts and deteriorating ABG parameters, despite initial bag and mask ventilation (Table 27.7).
Modes: Primary modes of mechanical ventilation include: (a) controlled mechanical ventilation (CMV) in a totally apneic child, (b) synchronized intermittent mandatory ventilation (SIMV) in a child with poor breathing efforts, and (c) spontaneous mechanical ventilation, e.g. CPAP, in a child with good breathing efforts (Table 27.8). Some newer modes of ventilation are discussed later.
• Controlled mechanical ventilation (CMV) may be volume-cycled or pressure-cycled, the later is preferred due to lesser risk of barotrauma and air-leaks. Two main types of pressure-controlled CMV are: (i) intermittent positive pressure ventilation (IPPV), where end-expiratory alveolar pressure falls to zero, and
(ii) positive end-expiratory pressure ventilation (PEEP), where a pre-determined positive pressure is maintained even in end-expiration. PEEP is usually used in cases with decreased lung compliance and tendency for alveolar collapse, e.g. hyaline membrane disease or acute respiratory distress syndrome.
• Spontaneous mechanical ventilation, e.g. CPAP is used for similar purpose as PEEP, but in a spontaneously breathing child. It may be provided through special ventilator or even with an indigenous breathing circuit via endotracheal intubation or long nasal-prongs. CPAP prevents complete collapse of alveoli in end-expiration and thus facilitates longer gaseous exchange and easier re-expansion of lungs during inspiration.
• Synchronized mechanical ventilation (SIMV) is used in children with spontaneous but poor respiratory efforts, specially during weaning phase from ventilatory assistance. In SIMV, ventilator allows the child to trigger a breath by spontaneous efforts. However, if patient takes too long time to initiate this effort, the inspiration is triggered by preset inspiration time.
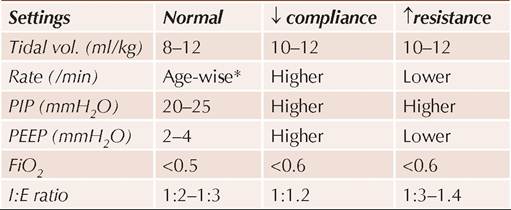
Initial ventilator settings: Although ventilation requirements of each child need to be individualized according to frequently monitored ABG status, initial ventilator settings usually depend on the state of lung compliance and airway resistance (Table 27.9).
For initial setting, the primary pathology may be classified as: (a) normal lung compliance and resistance,
(b) decreased lung compliance, e.g. pneumonia, ARDS, atelectasis, pulmonary edema, hyaline membrane disease, etc. and (c) increased airway resistance, e.g. asthma, bronchiolitis, etc.
A higher PEEP with lower inspiratory time is required in disorders with poor lung compliance, while reverse is indicated in cases with high airway resistance.
Monitoring: A child on ventilator should be frequently monitored for clinical improvement/deterioration, air entry into lungs, arterial blood-gases and spontaneous breathing efforts, to determine the need for revision of ventilator settings or tracheal tube.
Complications: Common complications of assisted mechanical ventilation are: (a) barotrauma, e.g. pneumothorax, (b) nosocomial infections, (c) ventilator malfunction, and (d) tracheal injury, e.g. sub-glottic stenosis.
Newer modes of ventilation: Although not widely available, some important new modes of mechanical ventilation are as follows:
High frequency ventilation (HFV) aims to provide adequate ventilation by increasing the frequency of ventilatory cycles with low tidal volume and inspiratory pressures. It is particularly useful in cases with airleak syndromes or refractory to conventional modes of ventilation.
Heliox ventilation is an experimental mode of ventilation, in which nitrogen in inspired air is substituted with helium. Helium, being an inert gas, facilitates laminar airflow, reduces airway resistance and allows good ventilation at lower inspiratory pressures. It is potentially useful in cases of air-leak syndromes and partial airway obstruction, e.g. croup and asthma.
Nitric oxide (NO) ventilation is based on adding 20-40 ppm of NO in inspired air.
As NO is a potent and selective pulmonary capillary vasodilator, it improves ventilation of poorly perfused lung segments and particularly useful in persistent pulmonary hypertension in newborns (PPHN) and acute respiratory distress syndrome (ARDS).Liquid ventilation, an experimental modality, substitutes air nitrogen with inert perfluorochemical (PFC) liquids, which lower the alveolar surface tension and open atelectatic alveoli for ventilation.
Extra-corporeal membrane oxygenation (ECMO) is an external mode of ventilation, where venous blood is passed through an in vitro membrane oxygenator for gaseous exchange (which acts as physiological lung) and then returned back to venous or arterial side. It is a highly effective mode of ventilation, though rarely available and associated with risks of thromboembolic complications and cannulation problems.
TABLE 27.9: Guidelines for initial ventilator settings
*infants: 30, toddlers: 20, older:16.
PIP: Peak inspiratory airway pressure, PEEP: Peak end-expiratory pressure, FiO2: Oxygen fraction in inspired air, I:E ratio: Inspiratory vs. expiratory time.
Acute Respiratory Distress Syndrome
Acute respiratory distress syndrome (ARDS) is an uncommon but potentially fatal cause of respiratory failure in critically sick children, characterized by:
a. Severe hypoxemia (PaO2:FiO2 gradient lt; 0.2),
b. Diffuse pulmonary infiltrates on chest X-ray,
c. Normal cardiac function.
Etiologically, ARDS is the pulmonary manifestation of systemic inflammatory process, triggered by various events, e.g. viral infections, septicemia, shock, aspiration, head injuries and immunological insults, e.g. bone marrow transplants.
TABLE 27.10: Berlin criteria (2013) for diagnosis of ARDS
TABLE 27.11: Causes of circulatory shock
• Onset within 1 week of known insult with progression
• Bilateral opacities on chest X-ray resembling pulmonary edema, and not explained by lung pathology#
• No obvious cardiac cause or fluid overload
• PaO2/FiO2 ratio lt;300 mm Hg on PEEP/CPAP gt;5 cm H2O Severity classification (PaO2/FiO2 Ratio)
Mild*: 200-300; Moderate: 100-200; Severe: lt; 100
#see Fig. 16.19
*Also termed acute lung injury
Pathological course of ARDS may be divided into three stages: (i) Exudative phase with increased capillary permeability leading to alveolar exudation (2-3 days), (ii) Proliferative phase with fibroblast proliferation (2-3 weeks), and (iii) pulmonary fibrosis in survivors with decreased lung compliance and vital capacity.
Clinically, early cases present like any other pneumonia, but with progressive hypoxia and hypercarbia, which does not respond to regular therapy.
Possibility of ARDS should be considered in any critically sick child, when SaO2 fails to rise gt;92% on gt;50% FiO2 delivered via spontaneous or assisted ventilation.
Diagnosis of ARDS should be considered in any case of pulmonary edema on chest skiagram (Fig. 16.19) without cardiac etiology, and confirmed on PaO2/FiO2 ratio, along with exclusion of other causes. Berlin criteria (2013) is commonly used to diagnose and classify the severity. (Table 27.10).
Management of these cases revolves around high PEEP ventilation for expansion of exudates-filled alveoli and reduce intrapulmonary shunting. Other modes of ventilation, e.g. high-frequency ventilation or extracorporeal membrane oxygenation (ECMO) are necessary in cases with high PEEP (gt;15 cm H2O) requirements and risk of air-leak syndromes.
Outcome is poor in most cases, with overall mortality ranging from 40-60% in early diagnosed cases to ~ 100% in un-ventilated cases.
27.3 SHOCK
The term 'Shock' denotes a “clinico-pathological state of circulatory insufficiency to meet metabolic and oxygen demand of tissues, due to any cause'. While hypotension is a common preceding event, shock may also develop despite well- maintained blood pressure due to inappropriate microcirculation, e.g. compensated shock.
Etiology: Adequate tissue perfusion depends on four major and interdependent factors: (a) blood volume, (b) myocardial function, (c) A-V pressure gradient at tissue level that determines capillary flow velocity and time available for exchange of oxygen/metabolites, and
(d) integrity of microvascular capillary bed.
• Hypovolemic shock
- External fluid losses:
#9830; GIT: Diarrhea, vomiting
#9830; Urinary: Diabetes insipidus
#9830; Skin: Heat stroke, burns
#9830; Lungs: Severe respiratory distress
- 3rd space losses: Ascites, paralytic ileus, edema
- Blood loss: Trauma, surgery, GI bleeding
• Septic shock
• Distributive
- Anaphylaxis: Drugs, envenomation
- Neurogenic: Head injury, spinal shock
- Toxic
• Cardiogenic shock
- Primary: Myocarditis, myocardiopathy
- Secondary: CCF, CHDs, RHDs
• Obstructive shock
- Cardiac: Pericardial tamponade, aortic stenosis
- Vascular: Coarctation of aorta
- Lungs: Tension pneumothorax, severe asthma
Shock represents abnormality in any one or more of these factors due to any cause. Consequently, it may be classified as (Table 27.11):
a. Hypovolemic shock, due to decreased intravascular volume, e.g. dehydration;
b. Distributive shock, due to decreased vascular tone with vasodilatation, increased venous capacitance and hypovolemia, e.g. anaphylaxis or septic shock;
c. Cardiogenic shock, due to impaired myocardial contractility, e.g. myocarditis;
d. Obstructive shock due to reduced cardiac output d e s p it e a d equa te my o cardial con trac tility, e.g. pericardial tamponade;
e. Dissociative shock, due to impaired oxygen utilization by cells, despite normal perfusion, e.g. abnormal Hb, preventing release of oxygen in tissues.
Septic shock, commonly seen in gram-negative infections, is a unique combination of distributive, hypovolemic, and cardiogenic shock, due to peripheral vasodilatation, capillary leak and myocardial dysfunction respectively. Apart from the infection per se, endogenous release of inflammatory mediators in response to the infection (Systemic inflammatory response syndrome or SIRS) contributes to the pathophysiology of septic shock.
In children, hypovolemic shock and septic shock are two most common causes of shock.
Pathophysiology of shock may be broadly divided in three stages—(a) compensated shock, (b) uncompensated or decompensated shock, and (c) multi-organ dysfunction.
Impaired tissue perfusion is the pathophysiological hallmark of shock that triggers various compensatory mechanisms to restore blood flow to vital organs, e.g. increase in HR, stroke volume, vascular tone and respiration (compensated shock). However, failure
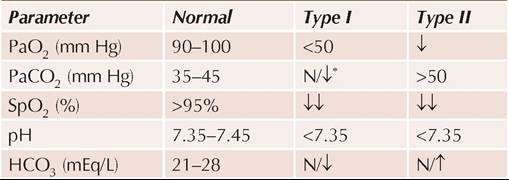
Fig. 27.13: Pathogenesis of shock.
of these compensatory mechanisms (uncompensated shock) leads to cellular hypoperfusion gt; hypoxia gt; shift to anaerobic metabolism gt; acidosis and ultimately multiorgan dysfunction, e.g. renal failure, hypoxic- ischemic brain damage, myocardial failure, acute respiratory distress syndrome (ARDS), hepatic failure, metabolic derangements, DIC and death (Fig. 27.13).
The term cold shock is used to denote shock with decreased capillary refill (gt;3 seconds), which is normal (lt;3 seconds) in warm shock.
Diagnosis: Early diagnosis of shock in compensated state and its etiology is vital to prevent irreversible multi-organ dysfunction. Assessment of a child in shock includes:
a. Detailed history, regarding etiology, e.g. fluid/blood loss, drug/toxin exposure, fever, previous cardiac disease, etc. as well as state of organ functions, e.g. urine output, sensorium, respiratory distress, etc.
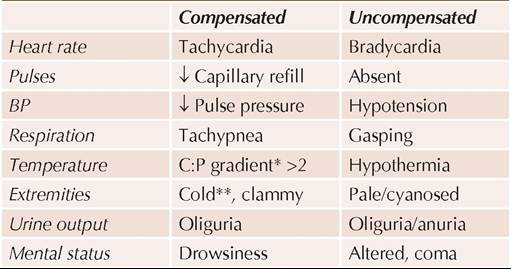
b. Clinical examination, to differentiate between compensated and uncompensated shock (Table 27.12), to identify possible etiology, and to assess organ damage. While tachycardia is the first compensatory phenomena, two other reliable signs of early/ compensated shock are: (i) increased capillary filling time (gt;3 second), usually tested on the heels by blanching,
TABLE 27.12: Clinical signs of shock
*Core (rectal)-Peripheral (axillary) temperature difference of gt;2°C **Warm extremities indicate septic shock
and (ii) increased core (rectal) vs peripheral temperature gradient (gt;2°C). BP may be normal in compensated state, though pulse pressure falls earlier, due to decreased systolic pressure.
c. Investigations in shock are usually deferred till initial stabilization, when detailed work-up is necessary for etiological diagnosis as well as to assess exact hemodynamic status and organ dysfunction. Important baseline investigations include:
• Hematological work-up for
- Hemoglobin (need for transfusion)
- White cell counts (septic etiology)
- Coagulation profile (secondary coagulopathy)
• Biochemical work-up, for
- Arterial blood gases (metabolic acidosis)
- Serum electrolytes
- Renal/liver function tests (organ dysfunction)
- Blood sugar (hypoglycemia)
• Chest X-ray (for ARDS, i.e. shock-lung)
• Other relevant investigations, as required for etiological diagnosis.
Management of shock aims to—(a) restore adequate perfusion, (b) revert secondary organ damage, and
(c) treat the primary cause. Important steps in management of shock are as follows:
Step I. Quick clinical assessment regarding presence of shock, its severity and probable cause, as well as general cardiopulmonary status and need for resuscitation.
Step II. Initial cardiopulmonary stabilization, i.e. ensuring airway patency and breathing support with 100% oxygen and/or assisted ventilation. Child should be placed in Trendelenburg position (supine with elevated legs) to facilitate cerebral perfusion.
Step III. Vascular access should be obtained as early as possible, via cannulation of a peripheral vein, or a large central vein, e.g. femoral or internal jugular vein. Intraosseous route may be effectively utilized in younger children with difficult venous access for immediate volume correction (see Ch 32.3).
*Improves / preserves Renal blood flow in doses lt;10 #956;g#8725;kg#8725;min ** vasoconstrictor in doses gt; 2 #956;g#8725;kg#8725;min
*** Load with 1.5-5 mg/kg bolus over 20 minutes
Step IV. Immediate volume expansion with 20 ml/kg of isotonic crystalloid infusion, e.g. Ringer lactate or Normal saline, over a period of 10-15 minutes is indicated in all cases, irrespective of the etiology of shock or hemodynamic status. Similar infusions may be repeated 2-3 times (max 60 ml/kg) over next one hour, if BP remains unrecordable or clinical improvement is not obvious. Colloids or blood transfusions have no role in immediate volume expansion.
Step V. Vasoactive agents, to improve myocardial function as well as to modify peripheral vascular resistance are indicated in—(a) hypovolemic shock not responding to volume expansion, or (b) all cases of nonhypovolemic, e.g. cardiogenic or septic shock. Many inotropic and vasopressor agents are available (Table 27.13) with variable effects on peripheral vascular resistance and the choice depends on cause of shock and hemodynamic status.
Generally, Dopamine (10 #956;g#8725;kg#8725;minutes) is preferred in most cases, for its beneficial vasodilator action on renal/splanchnic circulation along with inotropic effect at lower doses. Infusion rate must be titrated to response, up to 20 #956;g#8725;kg#8725;min.
Dobutamine-a pure inotropic agent with negligible peripheral effects is preferred in cardiogenic shock to augment myocardial contractility.
Norepinephrine is the inotrope of choice in septic and anaphylactic shock (with peripheral vasodilation), due to its peripheral vasoconstrictor effect.
Phosphodiesterase inhibitors, e.g. Amrinone or Milrinone, improve myocardial function directly by facilitating intracellular cAMP synthesis. However, these agents are potent peripheral vasodilators and should be used only after adequate volume replacement.
Selective vasodilators, e.g. sodium nitroprusside, (IV 0.3-7 #956;g#8725;kg#8725; minute) though rarely used, may be useful in selected cases of cardiogenic shock to reduce afterload and improve cardiac output during recovery phase.
Step VI. Reassessment of hemodynamic status is indicated as soon as BP starts improving and patient is stabilized with above measures. Most important concern at this stage is to avoid fluid overload and myocardial strain. Hence, it is preferable to establish a central venous line for monitoring of central venous pressure (CVP). Relevant investigations for etiological diagnosis are also indicated at this stage. Basic monitoring parameters in shock include:
• Clinical signs, e.g. HR, RR, BP, temperature and sensorium;
• Hemodynamic monitoring with CVP, PAWP;
• Respiratory monitoring with pulse oximetry and periodic ABG analysis; and
• Metabolic monitoring for electrolyte status.
CVP monitoring involves placement of a long venous catheter into right atrium through a peripheral vein. CVP is a very useful indicator of venous return and cardiac preload in hypotension/shock. Low CVP (lt;10 cm water) in shock indicates need for further fluid replacement while high CVP warns about the risk of volume overload or compromised myocardial function, to be managed with inotropic agents.
Pulmonary airway wedge pressures (PAWP), though more reliable indicator of circulatory overload, are difficult to monitor in day-to-day practice.
Step VII. Controlled fluid replacement, after initial volume expansion aims to keep: (a) BP gt;5th percentile, and (b) CVP between 10 and 16 cm H2O; and the rate of infusion should be guided with these parameters. Colloidal solutions, e.g. albumin, may be used at this stage, though blood is the best colloidal agent and also increases O2 carrying capacity. Blood transfusion is indicated in cases of hemorrhagic shock or severe anemia.
Step VIII. Other Supportive measures should also be instituted after initial hemodynamic stabilization, including: (i) adequate nutrition, (ii) antibiotics, (iii) correction of metabolic abnormalities, e.g. hypoglycemia, acidosis and dyselectrolytemia.
Role of steroids, except in anaphylactic shock or adrenal crisis, is highly controversial, generally not indicated. Extracorporeal membrane perfusion and intra-aortic balloon pulsations are recent methods to maintain normal circulation in refractory cases of shock.
Step IX. Management of multi-organ dysfunction, discussed below, is usually a terminal event in shock, with wide clinical spectrum and high mortality. All cases of shock should be constantly monitored for early diagnosis of various organ dysfunctions and necessary support.
Figure 27.14 provides an algorithm to manage septic shock - the trickiest of all types due to combination of distributive, hypovolemic and cardiogenic factors, with high mortality.
Multi-organ Dysfunction Syndrome
Multiple organ dysfunction syndrome (MODS) denotes a constellation of common terminal events in critically sick children. It is defined as a state of “altered organ
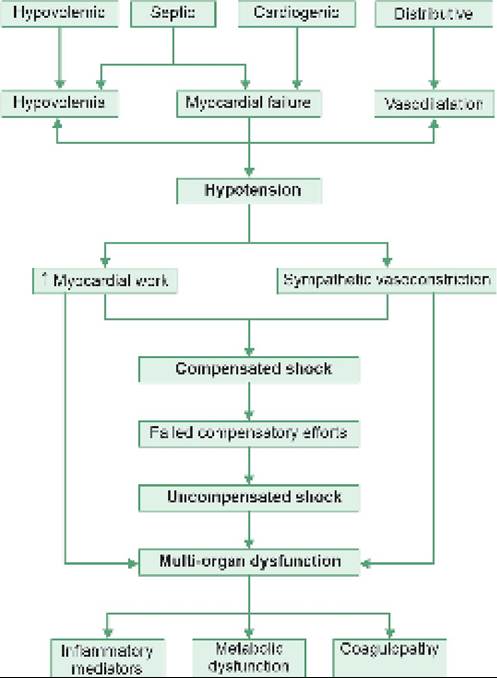
Fig. 27.14: Management of septic shock.
function in an acutely ill patient so that homeostasis cannot be maintained without intervention.”
MODS may be classified as: (a) primary, i.e. direct insult to multiple organs due to exogenous factors, e.g. bacteria or toxins, and (b) secondary, i.e. a consequence of exaggerated host response with generalized activation of inflammatory reactions in organs remote to the site of initial insult.
Pathogenesis: Though exact pathogenesis is unclear, important contributory factors for MODS include:
• Excessive stimulation of macrophages and consequent release of many humoral and chemical mediators, e.g. cytokines, (e.g. TNF#945;, IL-1, IL-6, etc.), bradykinin, nitric oxide, etc.
• Ischemic perfusion injury to vascular endothelium with consequent congestion, sludging and microthrombi formation.
• Impaired intestinal barrier, permitting entry of pathogenic gut organisms and endotoxins into systemic circulation.
• Generalized tissue hypoxia and consequent impairment of clearance mechanisms.
Clinical course: Regardless of etiology, MODS follows a downhill course in a critically sick child. Important manifestations include:
• Lungs : Acute respiratory distress syndrome.
• GIT: Bleeding, diarrhea, paralytic ileus.
• CVS : Shock or CCF.
• Renal : Oliguria and acute renal failure.
• CNS : Altered sensorium, seizures, encephalopathy.
• Blood : Bleeding diathesis, DIC, marrow failure.
Hepatic encephalopathy is relatively uncommon in children than in adults.
Management: Prompt recognition and treatment of potential causes is the most effective strategy in management of MODS, which includes: (a) appropriate antibiotic therapy, (b) local measures, e.g. drainage of abscesses, etc., (c) adequate hemodynamic and ventilatory support, and (d) continuous monitoring of various organ functions in intensive care unit.
Important diagnostic indicators as well as therapeutic interventions for various components of MODS are given in Table 27.14.
TABLE 27.14: Management of MODS in shock
*Glasgow coma scale
**More than two times of normal
27.4