PHYSIOLOGY OF WATER BALANCE
Physiology of water balance may be broadly divided into: (a) overall quantitative regulation of TBW, and (b) its inter-compartmental distribution, as follows:
A. TBW homeostasis revolves around the maintenance of normal plasma volume and osmolality.
Volume of the TBW depends on the equilibrium between external intake and small amount produced endogenously on oxidation of nutrients on one side; and excretion via urine (65%), skin (40%), lungs (15%) and stools (5%) on other side.Osmolality of the plasma depends on the pressure exerted by its two components: (a) colloids, e.g. albumin, and (b) crystalloids or electrolytes, e.g. Na+ and Cl-. Though colloidal (oncotic) pressure contributes only to a small fraction of total plasma osmotic pressure, it is more important determinant of osmotic gradient across the cell membranes than crystalloid pressure, as colloids do not pass through cell membranes.
The terms molality and molarity refers to number of solute molecules in 1 kg and 1 liter of solvent, respectively. Accordingly, osmolality refers to the 'pressure exerted by number of molecules in 1 kg of solvent', while osmolarity denotes 'molecular pressure in 1 liter of solvent'. Normal plasma osmolality (285-295 mOsm/kg H2O) roughly equals to the twice of plasma sodium concentration in mEq/L, though may be precisely calculated by following formula:
Osmolality = 2 (Na+ + K+) +
Glucose BUN
---------- +
18 2.8
Osmolality in mOsm/kg; Na/K in mEq/L; glucose/BUN in mg/dl.
Important regulatory mechanisms for TBW balance in human body (Fig. 7.1) are as follows:
a. Water intake depends on thirst, i.e. conscious desire to drink water, which is regulated by a center in mid-hypothalamus with two important afferents: Osmoreceptors in hypothalamus to detect changes in plasma osmolality and baroreceptors in atria and vascular bed to sense changes in plasma volume.
Probably, elevated angiotensin II levels in hypovolemic states also stimulate thirst.Primary disorders of thirst, i.e. polydipsia or adipsia are usually psychogenic in origin, though altered thirst may also indicate hypothalamic disorders, hypokalemia, malnutrition and disorders of renin-angiotensin system.
b. Urinary excretion is the most important determinant of TBW regulation. A part of urinary water excretion is obligatory, necessary to excrete the solute load. However beyond this, urinary volume is regulated by: (a) plasma
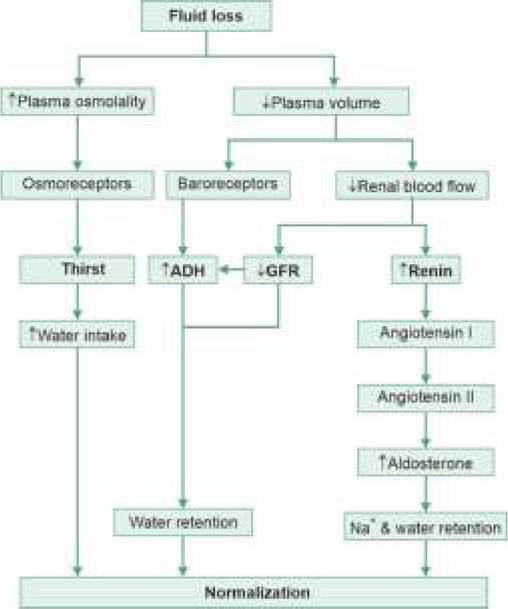
Fig. 7.1: Physiology of total body water balance.
volume and osmolality, (b) dietary solute load, (c) renal functions, and (d) hormonal control. Three important hormonal regulators of urinary water excretion are antidiuretic hormone (ADH), aldosterone and atrial natriuretic hormone peptide.
• Antidiuretic hormone of hypothalamic-hypophyseal axis, is a direct regulator of urinary water excretion. ADH secretion is regulated by osmotic pressure of ECF and it acts by increasing the cell-permeability of collecting ducts to enhance water absorption.
Important ADH disorders include: (a) excess secretion in neurological disorders, i.e. syndrome of inappropriate secretion or SIADH, (b) ADH deficiency in central diabetes insipidus, and (c) tubular nonresponsiveness to ADH in nephrogenic diabetes insipidus (Ch 22.2.4).
• Aldosterone, an adrenal hormone, is an indirect regulator of urinary water excretion, by manipulating sodium excretion. It is mainly secreted in response to reduced plasma volume via renin-angiotensin mechanism and increases tubular sodium reabsorption with passive water absorption.
• Atrial natriuretic hormone peptide is produced and stored in atrial myocytes and released in response to ECF overload leading to atrial stretching. It prevents the sodium/water reabsorption by antagonizing the renin-angiotensin mechanism.
TABLE 7.1: Major ions in body fluids
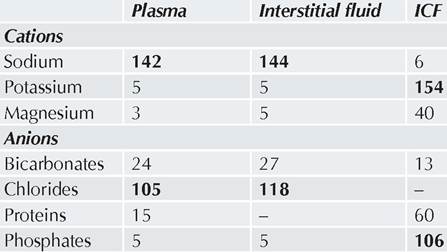
Figures in bold indicate major cation/anion in respective fluid compartments
c. Non-urinary losses in stools or insensible losses via skin/lungs are fairly constant in normal children with a little influence on overall water balance. However, these are important exits in pathological states, e.g. diarrhea (stools), fever (skin), respiratory distress (lungs). Insensible losses are also influenced by environmental temperature, humidity and body surface area, which should be considered during calculation of fluid requirements in sick children.
B. Inter-compartmental distribution: Water in ECF and ICF compartments is freely exchangeable and exists in a state of dynamic equilibrium. Within ECF too, water continuously moves between plasma to interstitial fluids. Important determinants of these inter-compartmental water distributions are as follows:
Extracellular vs intracellular fluid: Water movement between these two compartments depends on the relative osmotic gradient and active movement of ions. While sodium is the principle cation in ECF, potassium is principle cation in ICF (Table 7.1). Since cell membranes are free permeable to water, osmotic force across them is maintained by active transport of Na+ out of the cell and K+ into the cell-an energy-consuming process. Any change in Na+ content of ECF alters its osmolality with secondary effects in ICF. For example, hypernatremia increases osmolality of ECFgt; movement of water from ICF to ECFgt; cellular dehydration. Conversely, hyponatremia leads to movement of water into the cell and consequent cellular edema.
Plasma vs interstitial fluid: Interstitial fluid is derived from plasma, filtered through the semi-permeable capillary bed at the arteriolar end. However, most of it returns back to plasma at venular end, while the rest is carried back to vascular space via lymphatics.
Important determinants of fluid movements between plasma and interstitium are:Hydrostatic pressure in capillary bed that facilitates water movement from plasma to interstitial space; Osmotic pressure of plasma that prevents or reverts this movement; and
Capillary permeability.
In normal conditions, osmotic gradient between plasma and interstitial space (28 - 4.5 = 23.5 mm Hg) and capillary permeability is virtually constant, and water movement between these compartments is mainly decided by hydrostatic pressure, as follows:
• At the arteriolar end of capillary bed, hydrostatic pressure is more in vascular space than in interstitial space. Consequently, net hydrostatic pressure gradient (25 - (-7) = 32 mm Hg) exceeds osmotic gradient (23.5 mm Hg) and water moves out into interstitial spaces.
• At venular end, hydrostatic pressure in vascular space drops to 9 mm Hg. Consequently, net hydrostatic pressure gradient (9 - (-7) = 16 mm Hg) is less than osmotic gradient and water moves back in vascular space. Some interstitial fluid is collected by lymphatics, ultimately to return in vascular compartment.
Two important pathological abnormalities of fluid imbalance in children are edema and dehydration, discussed in following sections.
7.1.2
More on the topic PHYSIOLOGY OF WATER BALANCE:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- REFERENCES
- Equilibrium