RENAL TUBULAR ACIDOSIS
Renal tubular acidosis (RTA) denotes impaired renal capacity for urinary acidification, due to either (a) inadequate reabsorption of bicarbonates or (b) secretion of acids (H+ ions) in renal tubules, leading to a state of persistent metabolic acidosis (normal anion gap) with normal or near-normal GFR.
Pathophysiology: Kidneys is the prime regulator of normal acid-base balance by:
• Reabsorption of HCO3-, mainly in proximal tubules,
• Secretion of H+ in distal tubules and collecting ducts.
About 85% of HCO3- are absorbed in proximal tubules with recycling of H+- a process that needs adequate carbonic anhydrase activity (Fig. 21.7). However, there is no net excretion of H+ ions at proximal tubules level and hence, urine is not acidified here.
On the other hand, distal tubules and collecting ducts can retrieve only ~15% of bicarbonates but net H+ secretion occurs here, leading to actual acidification of urine.
TABLE 21.18: Selection criteria for renal transplant
• Chronic renal failure/end-stage renal disease
• Age gt; 2 years and/or weight gt; 10 kg
• Absence of HIV, serious systemic illness, severe mental retardation and untreated malignancy
• Availability of suitable living related donor
• Ensured compliance for long-term management
Consequently, RTA may be broadly divided into:
• Distal RTA or type I,
• Proximal RTA or type II,
• Hyperkalemic RTA or mineralocorticoid deficiency or type IV.
Type III RTA is a combination of type I and II RTA, not considered as a separate entity at present.
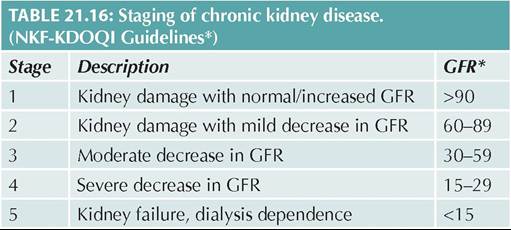
Fig. 21.7: HCO3 reabsorption in proximal tubules.
• Proximal RTA is a severe defect due to near-complete loss of HCO3- reabsorption capacity, which cannot be compensated by distal tubules, leading to severe bicarbonaturia.
However, urine is well acidified (pH lt;5.5) in these defects, due to intact distal tubular functions, i.e. H+ secretion. Proximal RTA may be an isolated defect, or more commonly a part of generalized proximal tubular dysfunction (Fanconi syndrome) leading to proteinuria, aminoaciduria, glucosuria and other electrolyte wasting along with bicarbonaturia (Ch 21.11.2).• Distal RTA is a milder defect due to minimal loss (10-15%) of HCO3- reabsorption capacity. However, urinary acidification is significantly impaired in these cases due to impaired H+ secretion and urinary pH does not fall lt;5.5, despite severe systemic acidosis.
• Type IV RTA, due to impaired aldosterone production or renal responsiveness to aldosterone is characterized by impaired secretion of both H+ and K+ ions at distal nephrons, leading to acidosis and hyperkalemia.
Important metabolic defects in RTA include:
• Persistent metabolic acidosis due to excessive excretion of bicarbonates in urine and defective urine acidification;
• Hyperchloremia due to compensatory reabsorption of chloride ions;
• Hypokalemia due to entry of more NaHCO3 (unabsorbed in proximal tubules) in distal tubules, which stimulates Na+ absorption in exchange for K+, in distal/collecting tubules. Hyperkalemia occurs in type IV RTA.
Etiology of RTA is heterogeneous and depends on the site of lesion (Table 21.20). While isolated defects of proximal or distal RTA are known as sporadic or inherited disorders, most cases are part of generalized defects in tubular transport.
TABLE 21.20: Causes of renal tubular acidosis (RTA)
Distal RTA (Type I)
• Isolated (Sporadic, AD, AR)
• Syndromic: Familial hypercalciuria, Wilson disease
• Secondary
- Interstitial nephritis, nephrocalcinosis, sickle cell disease
- Reflux nephropathy and chronic pyelonephritis
- Drugs and toxins: Amphotericin, Cisplatin
Proximal RTA (Type II)
• Isolated (sporadic or AR)
• Fanconi syndrome (Multiple tubular dysfunction)
- Primary or inherited (Ar, AD, XLR)
- Syndromic: Cystinosis, Lowe syndrome
- Drugs: aminoglycosides, Ifosfamide, cisplatin
- Toxins: Lead or other heavy metals
- Others: Myeloma, collagen disease, transplant rejection Hyperkalemic RTA (Type IV) (Mineralocorticoid deficiency)
• Primary: Addison disease, CAH, hypoaldosteronism
• Pseudohypoaldosteronism (aldosterone resistance)
• Secondary:
- Pyelonephritis, interstitial nephritis,
- Drugs: Cotrimoxazole, cyclosporine
AR: Autosomal recessive; AD: Autosomal dominant; XLR: X-linked recessive; CAH: Congenital adrenal hyperplasia
Fanconi syndrome is the commonest cause of proximal RTA, while distal RTA is usually acquired after toxic renal injury or interstitial nephritis.
Clinically, inherited RTA defects present in late infancy, while acquired cases may present at any age depending on the cause. Important manifestations include:
• Progressive failure to thrive,
• Persistent metabolic acidosis,
• Polyuria with dehydration,
• Signs of hypokalemia, e.g. muscular weakness,
• Signs of primary disease, e.g. rickets,
• Signs of other metabolic defects, e.g. nephrocalcinosis due to hypercalciuria and hypercitraturia
Diagnosis of RTA should be suspected in any case of failure to thrive with typical biochemical abnormalities, i.e.: (a) fluid-refractory metabolic acidosis, (b) low serum bicarbonate levels, (c) hyperchloremia and (d) hypokalemia; after excluding more common causes, e.g. diarrhea.
Important laboratory differences between proximal RTA and distal RTA (are provided in Table 21.21.
Treatment of RTA aims to correct acidosis and maintain normal serum bicarbonate and potassium levels. After
initial parenteral correction of acid-base and electrolyte disturbances, long-term therapy includes:
• Oral bicarbonate supplements as Shohl solution (1 mEq/ ml of bicarbonate equivalent) or Sodium bicarbonate tablets (3.4 mEq/300 mg tablets). Higher doses (5-20 mEq/kg/d) are required in proximal RTA or distal RTA in infancy, than distal RTA in older children (2-4 mEq/kg/d).
• Oral potassium supplements (2-4 mEq/kg/d) as Kesol solution (1 mEq/ml) in hypokalemic cases. Type IV RTA may need chronic treatment for hyperkalemia with sodium-potassium exchange resin (Kayexalate). Oral Potrate (potassium citrate) (1 ml = 2 mEq of K) has additional effect by improving the acidosis and the hypokalemia and is preferred alkali supplements
• Other supplements, e.g. vitamin D, phosphates, etc. may be required, specially in proximal RTA.
• Patients with distal RTA with symptomatic hyper- calciuria (recurrent hematuria or nephrocalcinosis) may require thiazide diuretics to decrease urine calcium excretion.
Prognosis of RTA depends on the cause. Isolated proximal RTA, though more severe initially, may resolve in first decade but isolated distal RTA is a life-long disease.
21.11.2
More on the topic RENAL TUBULAR ACIDOSIS:
- 3 Critical Care
- Defects of Tubular Bone or Spinal Growth Present at Birth
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025