Sensory Deficit
Partial or complete absence of different sensory modalities predisposes individuals with spina bifida
SEGMENTAL INNERVATION
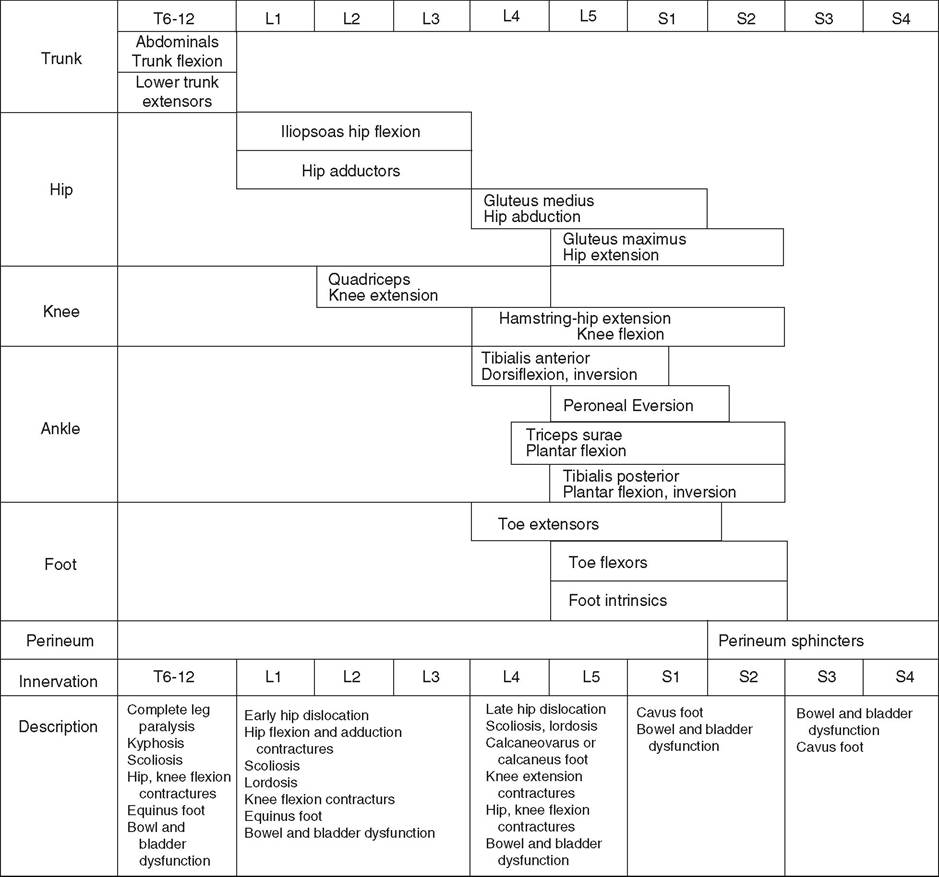
Figure 9.1 Musculoskeletal, sensory, and sphincter dysfunction by segmental level.
to skin injuries because of decreased ability to perceive pressure, pain, trauma, or heat (23,24,25,27). Skin breakdown tends to occur over areas of prominence and weight bearing. The lower back, inter- gluteal, perineum, feet, heels, and toes are the sites of predilection, but any area with sensory loss may be affected. Scoliotic and kyphotic prominences are areas prone to breakdown (26). Pressure ulcers often heal slowly, tend to get infected, and often recur. A pressure ulcer may be a symptom of a tethered cord. Long-standing ulceration with deep tissue necrosis may spread to bone and lead to acute or chronic osteomyelitis.
Other complications of denervation include vasomotor instability, neuropathic Charcot joints, and osteoporosis in individuals with extensive lower extremity weakness (25,26,27,28).
The spinal cord defect usually results in a lower motor neuron process. Spasticity is present in most individuals with spina bifida across their lifetime (29). The presence or gradual development of spasticity above the level of the spinal cord lesion may be related to tethering of the spinal cord, Chiari type II malformation exerting pressure on the cervical spinal cord, decompensating hydrocephalus, ventriculitis, syringohydromyelia, or coexistent encephalopathy sustained at birth (30-33).
More on the topic Sensory Deficit:
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY
- Inspection
- THE IMPORTANCE OF SOCIAL-EMOTIONAL LEARNING AND CONFLICT MANAGEMENT
- Mind Projection
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- B Hypotheses: Always Under Construction
- Focal Segmental Glomerulosclerosis
- Feet
- NEURAL TUBE DEFECTS
- Perioperative Care and Complications of Gynecologic Surgery