Somatosensory-Evoked Potentials
General Principals
The somatosensory-evoked potential (SSEP) is the sequence of voltage changes generated in the brain and the pathway from a peripheral sensory nerve following a transient electrical stimulus to the sensory cortex.
Evidence suggests that these signals are related to large afferent fibers and peripheral nerves, which ascend through the dorsal column pathways of the spinal cord, proceed to the thalamus, and arrive at the somatosensory cortex. These are the same pathways that mediate light-touch two-point discrimination, proprioception, and vibration. Sensitive amplification and averaging techniques enable discrimination between the evoked response and other larger and more random physiologic potentials with which the signal is mixed. As a general rule, SSEP studies may be considered whenever the disease process in question can involve the somatosensory system. SSEPs reflect neurophysiologic activity in the posterior column, medial leme- niscus pathways. They do not reflect activity in the anterolateral column of the spinal cord. Thus, SSEPs correlate better with clinical examinations of proprioception and vibration rather than pain or temperature sensation.Individual components of the SSEP waveform are identified by their latency (ie, the time at which they occur following a peripheral stimulus), their polarity, their position at which they are observed to be maximal, and, to a lesser extent, by the amplitude and shape of the waveform. Individual components are referred to by a letter and number. The letter (N for negative or P for positive) refers to the polarity of the wave and the number either to the latency in milliseconds of the signal from the time of the stimulus (eg, N20), or alternatively, especially appropriate in pediatric SSEPs, the order in which the component was observed (eg, N1, P2). Examples of median and tibial SSEPs are shown in Figures 7.16 and 7.17.
With mixed-nerve stimulation, recording electrodes are placed over the peripheral nerve more proximally, thoracolumbar or cervical spine, linked mastoids, and scalp. For upper extremity stimulation, the likely generator source for the cervical spine response is the incoming root, as well as postsynap- tic excitatory potentials generated at the dorsal root entry zone (108). For the lower extremity, the lumbar spine responses are similarly a reflection of the root or cauda equina activity and the postsynaptic activity of the cord. The linked mastoid response is generated at the brainstem level. The difference in the latency of scalp N1 and the cervical spine response with median nerve stimulation gives a central conduction time. Similarly, the difference in latency between scalp P1 for posterior tibial nerve stimulation and the spinal potential generated over T12 or L1 gives a central conduction time.
Filter settings vary from a low-frequency filter of 3-30 Hz to a high-frequency filter of 1.5-3 KHz. The peripheral nerve is typically stimulated with a rate of 3.1 Hz. Our lab utilizes a stimulation intensity of 1.5 times motor threshold for mixed-nerve stimulation and 2.5 times sensory threshold for dermatomal stimulation. Electrodes are positioned according to a modified international 1020 electrode system.
SEP latencies decrease with age until well into childhood (108-111). The maturation with growth of SSEPs is mainly associated with cell-growth processes such as myelination and with cell differentiation and synaptic development. Conduction velocity along the central pathways progressively increases until 3-8 years of age, remains constant between 10-49 years of age, and slows thereafter. The N1 scalp latency of the median SSEP decreases until 2 to 3 years of age (owing to peripheral myelination) and then increases with body growth until adulthood. The cervical spine latency is relatively stable during the first two years (due to concomitant peripheral myelination and body growth), and then increases with age from 2 to 3 years until adulthood.
The median SSEP central interpeak latency between cervical spine latency and scalp N1, which reflects central conduction time, decreases from a mean of 11.6 milliseconds at 4 to 8 months of age to a mean of 7 msec at 6 to 8 years of age, and remains constant between 6.9 and 7.0 msec until adulthood (112,113).Among infants less than 4 months of age, sleep can affect the cortical components and is best performed on the awake infant. With children greater than 4 months of age, sleep or sedation usually has little effect on the SEP waveform when performing mixed- nerve stimulation. Indeed, the author has had no difficulty obtaining median nerve scalp responses in the pediatric ICU in comatose children with head trauma or those heavily sedated. Dermatomal SSEPs, on the other hand, are state-dependent responses affected by both sleep and sedation.
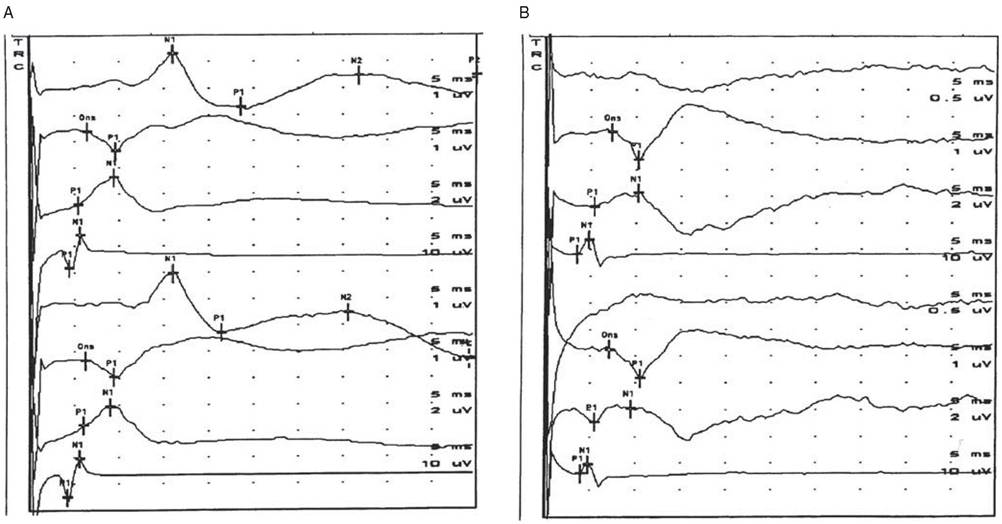
Figure 7.16 Median nerve somatosensory-evoked potentials (SSEPs) obtained in the pediatric intensive care unit. Channels 1-4 are responses with left median nerve stimulation, and channels 5-8 are responses with right median stimulation. Channels 1 and 5 are scalp responses (C4' and C3' referenced to Fz); channels 2 and 6 are brain (C4' and C3' referenced to linked mastoids); channels 3 and 7 are lower cervical spine responses (C7 spine referenced to Fz); channels 4 and 8 are peripheral responses obtained at the axillae. (A) Normal median SSEP responses obtained from a child with an epidural hematoma who was paralyzed with vecuronium for intracranial pressure control. There is no evidence of myelopathy. The child later recovered with minimal sequelae. (B) Abnormal median SSEP responses in a comatose child with severe brain injury and C1—C2 vertebral injuries. Note the bilaterally abnormal scalp reponses. Brainstem, C7 spine, and peripheral
responses show no evidence of a spinal cord injury affecting posterior column pathways.
Clinical Applications of SSEPs in Children
Brain Injury in SSEPs. Abnormalities of median SSEPs can be predictive of poor prognosis in the situation of brain injury due to head trauma or hypoxia. A loss of bilateral SSEP scalp waveforms, as shown in Figure 7.16A, portends a poor prognosis in comatose children (114-119). Asymmetric scalp responses in a comatose child may be associated with the development of motor abnormalities such as hemiparesis because of the proximity of the sensory cortex to the motor cortex (Fig. 7.17B). A recent study compared the predictive powers of clinical examination (pupillary responses, motor responses, and Glasgow Coma Scale [GCS]), electroencephalography (EEG), and computed tomography (CT) to that of SSEPs in a systematic review. SSEPs appear to be the best single overall predictor of outcome (118). Posterior tibial nerve SSEPs performed on neonates at high risk of future neurode- velopmental impairment have demonstrated a highly significant relationship between bilaterally abnormal posterior tibial nerve SSEPs and the presence of cerebral palsy at 3 years of age (120). Normal posterior tibial nerve SSEPs were associated with a normal outcome in 24 of 25 infants. In this study, posterior tibial nerve SSEPs were more predictive than cranial ultrasound. Another study of 43 children with hemiplegic cerebral palsy found a positive correlation between median nerve SSEPs and the affected side using the amplitude of the responses rather than the latency (121). Other studies have confirmed the prognostic value of SSEPs in infants at risk for neurodevelopmental impairment (122-125).
Traumatic Spinal Cord Injury. SSEP results combined with early American Spinal Injury Association (ASIA) motor scores have been shown to predict ultimate ambulatory capacity in patients with acute spinal cord injury (126,127). Other authors have shown that SSEP improvement over a one-week interval during the first three weeks after spinal cord injury was associated with motor index score improvement over a six-month period (128).
Both ASIA scores and MEP recordings are similarly related to the outcome of ambulatory capacity and hand function in patients with SCI. Dermatomal somatosensory-evoked potentials have also been shown to be more sensitive for the detection of sacral sparing and of more prognostic value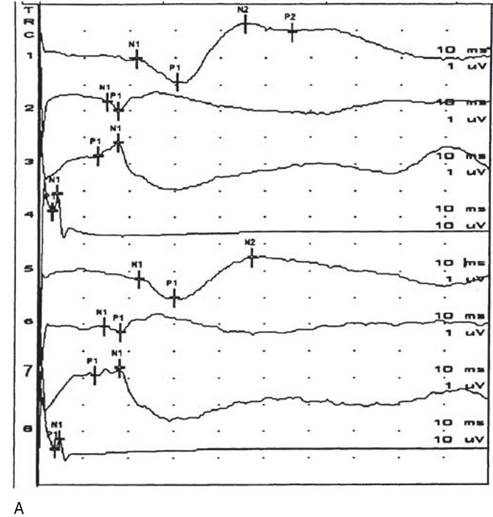
than mixed-nerve somatosensory-evoked potentials (129). However, somatosensory-evoked potentials and dermatomal SSEPs have been shown to add little or no useful prognostic information to the initial physical examination in either complete or incomplete spinal cord injury patient groups (130).
The author has a great deal of experience utilizing somatosensory-evoked potentials in the pediatric intensive care unit to evaluate for spinal cord injury without radiographic abnormality (SCIWORA) (131)
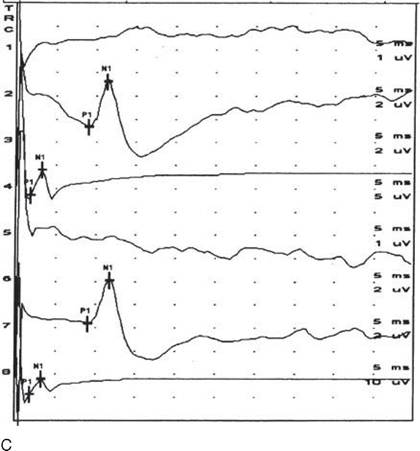
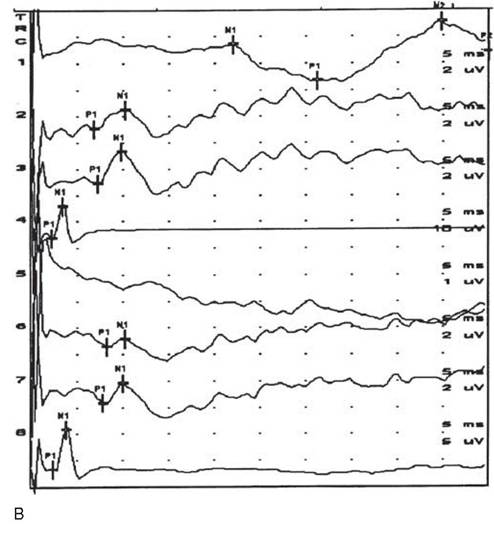
Figure 7.17 Tibial somatosensory-evoked potentials (SSEPs) obtained in the pediatric intensive care unit. Channels 1-4 are responses with left tibial stimulation, and channels 5-8 are responses with right tibial stimulation. Channels 5-8 are responses with right tibial stimulation. Channels 1 and 5 are scalp responses (C2' to Fz); channels 2-7 are spine responses (L2 spine referenced to flank); and channels 4 and 8 are peripheral responses obtained at the popliteal fossa. (A) Normal tibial SSEP study. (B) Abnormal tibial SSEPs in a child with left hemispheric brain injury. Peripheral and lumbar spine (L2 and T12 level) responses are normal bilaterally. The scalp response is normal with left tibial nerve stimulation (channel 1), but absent with with right tibial nerve stimulation (Channel 5). (C) Abnormal tibial SSEPs bilaterally in an awake 4-year-old with low cervical spinal cord injury without radiographic abnormality.
Peripheral (channels 4 and 8) and L2 spine (channels 2 and 7) responses are normal. Scalp responses (channel 2 and 5) are absent as a result of the low cervical spinal cord injury.in the situation where children are comatose or too obtunded to cooperate with the examination, or the child's age precludes a detailed sensory examination. Figure 7.17A shows an example of a normal tibial SSEP, whereas Figure 7.17C demonstrates the impaired posterior column conduction between the lower cervical spinal cord and brainstem with a SCIWORA injury sustained by a 4-year-old child.
Tethered Cord Syndrome. Posterior tibial SSEPs have been shown in some studies to be a sensitive indicator of declining neurophysiologic status and a more sensitive diagnostic tool than the clinical testing of sensation in patients with tethered spinal cord post-myelomeningocele repair (132-135). In addition, improvement of the evoked potentials has been documented subsequent to untethering (132,133,135). In the author's experience, the spine response is often caudally displaced in myelomeningocele. Absent- or reduced-amplitude lumbar spine potentials or prolonged lumbar spine or scalp latencies with tibial nerve stimulation in the setting of normal median somatosensory-evoked potentials (normal spine latencies and amplitudes with median nerve stimulation, normal cervical-to-brain central conduction time, and normal median scalp latencies) have been suggested to be indicators of electrophysi- ogic impairment due to tethered cord syndrome.
In the most comprehensive study to date, 90 children were followed with serial peroneal SSEPs after a repair of their spinal dysraphic lesions with the objective of evaluating whether SSEPs were a useful way of monitoring these children to facilitate early detection of clinically significant retethering. Three hundred and nine studies were performed on these children, yielding a mean of 3.4 studies per patient. The median time between SSEP studies was 13 months. A clinical examination was performed at the time each SSEP was done. There was a false-positive rate of 71% and a false-negative rate of 43%. It was concluded that serial SSEPs do not correlate well with clinical status and are not a useful modality for monitoring patients at risk for retethering (136). The author has followed a large population of children with myelomeningocele for decades and similarly has not found mixed-nerve SSEPs to be useful in the evaluation of secondary tethered spinal cord after myelomeningocele repair.
Intraoperative Spinal Monitoring. There are many reports detailing the usefulness of intraoperative SSEP monitoring during scoliosis surgery (137-140), as well as during other surgical procedures of the spine. The limitation of SSEPs is that they only monitor afferent pathways in the dorsal columns. Over the past decade, intraoperative spinal monitoring has evolved to include monitoring of the motor pathways. The corticospinal tracts are now being routinely monitored intraop- eratively using transcranial electrical stimulation of the motor cortex (141), with motor-evoked potentials recorded from either peripheral motor axons or as a CMAP from innervated muscles. Transcranial electric MEPs to monitor the corticospinal motor tracts are now used routinely in addition to SSEPs for detection of emerging spinal cord injury during surgery to correct spine deformity or resect intramedullary tumors (54,55,56).
Brachial Plexus Injury. The dermatomal SSEP can be a useful supplement to the assessment of the child with a brachial plexus injury (142). The child needs to be awake during the study. The C5 and C6 dermatomal SSEPs are generally most useful in the author's experience. The C5 dermatome is stimulated over the lateral proximal shoulder, using a proximal disk as cathode and distal disk as anode. Intraoperative SSEPs with direct stimulation of exposed nerves may demonstrate incomplete injuries of upper cervical roots, a proximal stump of the ruptured C5 root with functional central continuity (thus, potentially suitable for grafting), or complete root avulsion. Preoperative diagnostic SSEPs, while a useful adjunct to conventional electrodiagnosis, do not enable one to discriminate incomplete cervical root avulsion from intact roots (143).
Demyelinating Diseases. Both SSEPs and brainstem auditory-evoked potentials have been reported to be abnormal in children with or carriers of leukodystrophy (144,145). Peripheral and/or central abnormalities have been documented in metachromatic leukodystrophy, Pelizaeus-Merzbacher disease, Krabbe disease, adrenoleulodystrophy, Canavan disease, Alexander disease, and multiple sulphatase deficiency (146).
Pediatric multiple sclerosis (MS), while relatively rare, does occur in preadolescents and adolescents (147). MRI has been shown to be slightly more sensitive than multimodal-evoked potentials in confirming the clinical diagnosis of childhood MS. However, in suspected or probable MS, both SSEPs and visual- evoked potentials may contribute to the determination of clinical diagnosis because of their capacity to demonstrate asymptomatic involvement in central somatosensory and central optic nerve pathways (148,149).
Acute transverse myelitis often results in severe myelopathy due to inflammation and demyelination. SSEPs have been shown to be abnormal in this condition and may provide prognostic information regarding ultimate outcome (150).
The extent and location of nerve involvement in demyelinating peripheral neuropathies has been evaluated with SSEPs; however, SSEPs do not usually provide necessary additional information to standard nerve conductions. Hereditary motor sensory neuropathy type I shows impaired peripheral conduction in both proximal and distal nerve segments with normal central conduction. AIDP patients have been shown to exhibit prolonged posterior tibial peripheral SSEP latencies in addition to prolonged or absent median F-waves. However, posterior tibial F-wave latencies and median nerve SSEPs were less sensitive studies for the detection of demyelination in AIDP (151). SSEP can detect an abnormality and thus support the clinical diagnosis of Guillain-Barre syndrome in the acute stage when the results of more conventional tests are inconclusive (152).