Special Considerations for Nerve Conduction Studies
The best normative data for pediatric nerve conduction studies are available for the median, ulnar,

Figure 7.3 Recording electrodes for a median motor nerve conduction study in a small child.
The active electrode is placed over the abductor pollicis brevis on the thenar eminence. The recording electrode is a ring electrode placed on the index finger. The ground electrode is a 6-millimeter silver disc electrode placed on the back of the hand.peroneal, tibial, facial, and phrenic motor nerves and the median, ulnar, and sural sensory nerves. Stimulation of the posterior tibial nerve (recording abductor hallucis brevis) produces a discrete CMAP more commonly than stimulating the peroneal nerve (recording over extensor digitorum brevis). The extensor digitorum brevis (EDB) muscle may be difficult to visualize or palpate in infants. Its CMAP configuration frequently has either an initial positivity or a low broad configuration. In addition, the CMAP amplitude may change substantially with slight changes in position for the active electrode over the extensor digitorum brevis.
The axillary and musculocutaneous motor nerve conduction studies may be helpful in the setting of infantile brachial plexopathy. Care should be taken to minimize volume conduction. Often, the intact side is used for amplitude comparisons.
Evaluations of proximal nerves, such as the axillary spinal accessory musculocutaneous and femoral, are often useful in the evaluation of severe demyelinating neuropathies (Fig. 7.4). The distal latencies of these nerves may be severely prolonged on the setting of severe reductions in the CMAPs of more distal nerves due to conduction block or axon loss.
Percutaneous stimulation of the phrenic nerve is performed with techniques similar to that utilized in the adult, with stimulation performed at the posterior border of the sternocleidomastoid at the level of the thyroid cartilage or alternatively just medial (or occasionally lateral) to the sternal head of the sternocleidomastoid. Recording electrodes may be placed in the fifth to sixth intercostal space 2 cm apart at the anterior axillary line, or alternatively an active electrode may be placed immediately below the costal margin at the level of the nipple with recording electrode at the xiphoid.
The active electrode may need to be moved to adjacent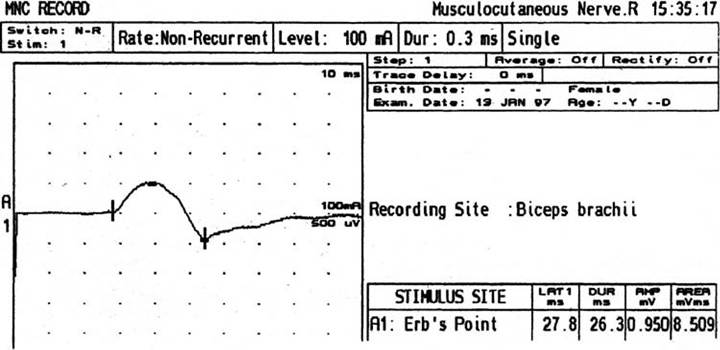
Figure 7.4 Nerve conduction study of the musculocutaneous nerve in Charcot-Marie-Tooth (CMT) type III. The nerve is stimulated at Erb's point and the recording electrode is placed over the biceps brachii. Distal latency is severely prolonged at 27.8 milliseconds. Note the reduced compound muscle action potential amplitude, presumably due to conduction block, and the relative lack of temporal dispersion, which is frequently seen in CMT.
positions to obtain an optimal M-wave (Fig. 7.5). Normative values for phrenic latencies have been reported in children (26,27). The author prefers to use ultrasound visualization of the diaphragm simultaneously with phrenic nerve stimulation to confirm downward deflection of the diaphragm. Volume conduction to the long thoracic nerve may produce a CMAP from the serratus anterior rather than the diaphragm. The downward deflection of the diaphragm spontaneously and with electrical stimulation may be confirmed and distance of diaphragmatic excursion quantitatively measured by ultrasound M-mode.