Spinal Cord
Tethered cord refers to an abnormal attachment of the spinal cord at its distal end (27). Under normal circumstances, the conus medullaris ascends from its distal position to the L1 to L2 vertebral level during the first year of life (37).
Focal abnormalities— including thickened and shortened filum terminale, supernumerary fibrous bands, persistent membrane reunions, dural sinus, diastematomyelia, entrapment by lumbosacral tumors, and adhesions in the scar tissue of the repaired myelomeningocele—interfere with this process (27). All children born with spina bifida have a low-lying cord on magnetic resonance imaging, and approximately one-third develop neurologic, urologic, or orthopedic complications or symptoms (38) (Fig. 9.2).Tethering of the spinal cord is the second most common cause of neurologic decline in a child with myelomeningocele (38). The most common clinical signs or symptoms of a tethered cord include spasticity in the lower extremities, decline in lower extremity strength, and worsening scoliosis. Other signs and symptoms that strongly suggest tethering of the spinal cord include back pain, changes in urologic function, changes in gait, and development of lower extremity contractures. In patients who are suspected of having a symptomatic tethered cord, the function of their shunt needs to be evaluated prior to proceeding forward with surgical management (39).
The reported functional outcome of surgical management of a tethered cord is variable. One study reported improvements in gait in almost 80% of patients following untethering, whereas other studies report improvement in as few as 7% (40). (Note: All cords tether to some extent following repair.) Less than 20% of children with a tethered cord experience back pain. However, this is the symptom most likely to improve with surgery (30,41).
Diastematomyelia is a postneurulation defect that results in a sagittal cleavage of the spinal chord, most commonly affecting the lumbar and thoracolumbar levels of the spinal cord.
It is more common in females (42,43). Diastematomyelia may have both neurologic and orthopedic presentations. Orthopedic symptoms include scoliosis, Sprengel's deformity (especially when associated with Klippel-Feil sequence), hip subluxation, and lower extremity limb-length discrepancies (43,44).Associated Central Nervous System Malformations
| Spinal cord Tethering Distal focal abnormalities Thick, short filum terminale Supernumerary fibrous bands Lumbosacral tumors (lipoma, fibrolipoma, fibroma dermoid, epidermoid cyst, teratoma) Bony vertebral ridge Diastematomyelia, diplomyelia, split cord | Cerebellum Arnold-Chiari type II malformation Elongated vermis, inferior displacement Herniation into cervical spinal canal Abnormal nuclear structures Dysplasia, heterotopia, heterotaxia Ventricular system Hydrocephalus Aqueductal stenosis, forking, atresias |
| Brainstem Arnold type II malformation Kinking, inferior displacement of medulla Herniation into cervical spinal canal Abnormalities of nuclear structures Dysgenesis, hypoplasia, aplasia, defective myelination Hemorrhage, ischemic necrosis Syringobulbia | Forebrain Polymicrogyria Abnormal nuclear structures Heterotopia (subependymal nodules) Heterotaxia Prominent massa intermedia Thalamic fusion Agenesis of olfactory bulbs and tracts Attenuation/dysgenesis of corpus callosum |
9.1

Figure 9.2 T2-weighted magnetic resonance image of tethered cord. There is tethering of the spinal cord with conus seen down to the L5 vertebral level, heterogeneous signal intensity characteristics, and areas of fibrofatty tissue.
A
Neurologic symptoms include gait abnormalities, asymmetric motor and sensory deficits of the lower extremities, and neurogenic bladder and bowel (45).
Symptoms of diastematomyelia may present in childhood or, less commonly, in adulthood (46).It is not uncommon for individuals to develop syringomyelia—a tubular cavitation in the spinal cord parenchyma extending more than two spinal segments (47). Syringomyelia is present in up to 40% of individuals with myelomeningocele (48). The syrinx may be located anywhere along the spinal cord, medulla, or pons, but is most common in the cervical region (23,24,49). Magnetic resonance imaging (MRI) is used to detect syringomyelia (50) (Fig. 9.3).
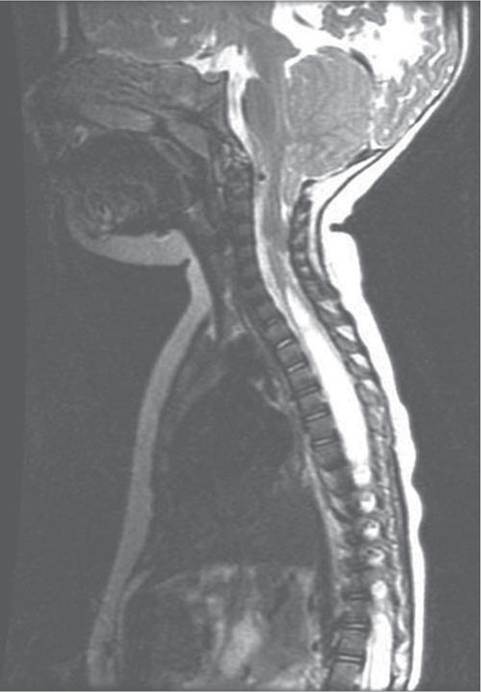
Often, a syrinx is of little clinical significance; however, if a patient develops decreasing function above the level of their lesion, syringomyelia must be considered in the differential diagnosis. Although shunt malfunction and cord tethering are more common complications, symptomatic hydromyelia may explain a slower-than-expected progression through gross motor and fine motor developmental milestones or a decrease in strength/function. Early progression of scoliosis above the initial neurologic level may be the earliest sign of a syrinx. A shunt malfunction
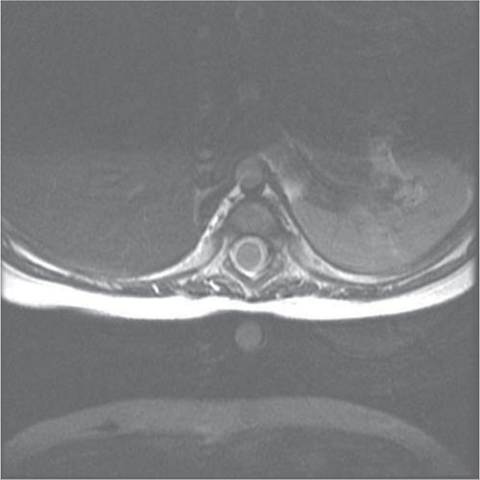
B
Figure 9.3 T2-weighted magnetic resonance image showing sagittal (A) and axial (B) views. There is a large syrinx present, beginning at the mid portion of C6 and extending to L4.
may contribute to a symptomatic syrinx, and shunt function should be evaluated. Placement of a syrin- gopleural shunt may be necessary to decompress the syrinx.