Spine
Spine deformities are common in this population and can be grouped as congenital or paralytic in nature (106). The common descriptions of spine deformities are classified as kyphosis, lordosis, and scoliosis.
The probability of development of scoliosis tends to follow the neurologic level. Historically, those with thoracic lesions have an 80% to 100% chance of developing scoliosis, followed by lumbosacral levels, with a 5% to 10% risk. Stratification of spine risk defined by neurologic level makes intuitive sense. Glade et al grouped children into four groups to predict spine deformities: Group 1 is L5 and below, Group 2 is L3-L4, Group 3 is L1-L2, and Group 4 is T12 and above (107). Based on these categories, Group 1 tends to have a low probability of developing spine deformities, Group 2 has a medium risk, and Groups 3 and 4 have a high probability of developing spinal deformities (108). Scoliosis tends to progress most rapidly during growth periods, especially during puberty. The effects scoliosis can have on the individual include changes in sitting balance, abnormal weight distribution and increased risk for pressure ulcers, compromised respiratory capacity, functional changes, pain, body image changes, and impact on ambulation.Treatment of the different spine deformities are grouped into observational, nonsurgical, and surgical. Nonsurgical options include bracing, seating, therapy, and complementary techniques. Spine orthotics and braces used are mainly thoracic lumbar spine orthoses (TLSO) and incorporate three points of pressure to maintain alignment of the spine. Wheelchair seating can be incorporated to optimize spine position using molded systems or lateral support. However, molded seating systems often encourage spinal curve and have to be redone more frequently than those that are noncontoured. Therefore, a TLSO is a good option to encourage the spine to be in as straight a posture as possible, especially during those activities when the pressure on the spine is the greatest.
The pressure on the spine is greatest in sitting, followed by standing, and least in the supine position. Surgical options should be considered when spine curves are above 45 degrees and the child is at an appropriate developmental level.Spinal deformities in this population present some unique challenges. The child with a high lesion in the thoracic area may be born with a congenital kyphosis and Gibbus deformity (Fig. 9.7). These structural abnormalities not only cause seating and mobility issues, but also present the clinician with challenges in maintaining skin integrity. The deformity can affect the development of the chest and has cosmetic implications. Treatment options include conservative management with bracing and seating modification to much more aggressive approaches. Kyphectomy and posterior fusion done at an early age is one option. This surgery generally includes not only bony procedures, but also may include transection of the spinal cord. These surgeries are known for their high complication rate (89%), but have an average kyphosis correction of 81.9 degrees. However, 22% of the cases in this series required shunt revision within six weeks due to surgically induced altered cerebrospinal fluid (CSF) dynamics (109) (Fig. 9.7).
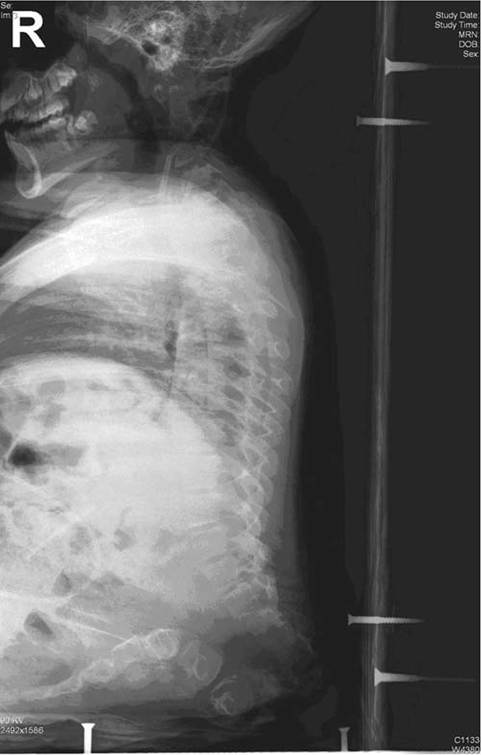
Figure 9.7 Congenital structural kyphosis with a sharply angled curve, or Gibbus deformity, associated with thoracic- level spina bifida.
Once a definite procedure is required, more traditional techniques for spine fusion are done. Surgery timing is based on degree of curvature and is generally considered at 45 degrees. Different approaches for fusion include anterior, posterior, and endoscopic options. Realistic goals of the procedure, along with potential complications, should be discussed prior to surgery. These include improved sitting, reduced pelvic obliquity, impact on functional status, and ambulation.
To maintain ambulation and control pelvic rotation, discussions about fusion to the pelvis are important considerations (110). However, fusion to the pelvis can interfere with sitting. The impact on function and self-perception after surgery remains controversial (111). Complications after surgery are common and include a high risk of infections, pseudoarthrosis, and instrument failure. It has been noted that it takes several months to get back to presurgery ambulation baseline.Newer surgical treatment for neuromuscular scoliosis has evolved over the last decade. Techniques to deal with the growing child have encouraged development of fusionless surgeries. Specific goals of these techniques are to delay definitive surgery until the child has reached a more optimal size, allow chest development and improve lung capacity, and sometimes to avoid surgery. These techniques include growing rods, intervertebral stapling, and use of vertical expandable prosthetic titanium rods (VEPTR) (112,113) (Fig. 9.8).