Hips
The development of the hip and associated problems is related to the neurologic level. Broughton found that by age 11 years, children with thoracic-level lesions had a 28% risk for dislocation, L1-L2 had a 30% risk, L3 had a 36% risk, L4 had a 22% risk, and L5 had a 7% risk.
The development of hip flexion contractures was highest in the thoracic- and high lumbar-level lesions (114). Children with thoracic-level lesions have no muscle influence on hip stability and may or may not develop hip dislocation. These children tend to frog-leg (hip abduction and external rotation) when lying down and develop contractures of the hip flexors and external rotators. In addition, the tensor fascia lata becomes contracted and may need to be surgically lengthened if it affects positioning. Children with high lumbar lesions have an imbalance of muscle activity around the hip joint. The active hip flexors and adductors (L1-L2) with unopposed abduction and extension tend to result in persistent coxa valga and development of acetabular dysplasia. These forces can result in hip subluxation and dislocation. This process occurs not only in the higher lumbar levels, but also in the mid- and lower lumbar segments. Weak or absent hip extension and abduction are directly related to hip dislocations. Unilateral hip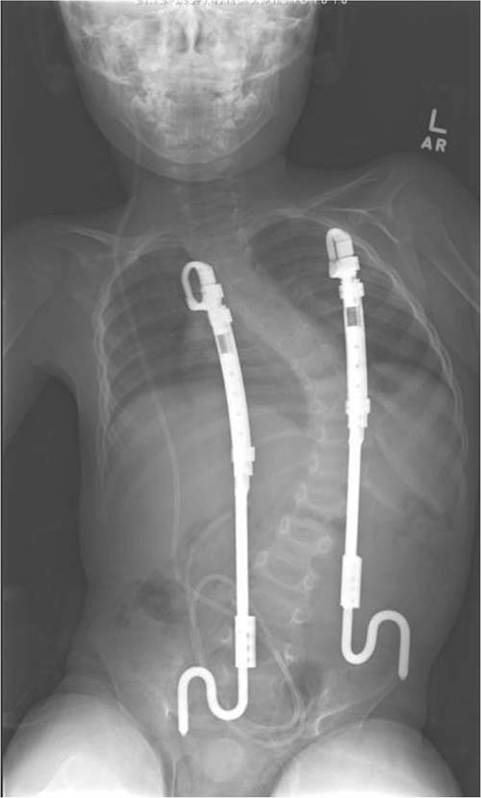
Figure 9.8 Child with spina bifida and scoliosis treated with vertical expandable prosthetic titanium rib (VEPTR). Note the spinal dysraphism with increased intrapedicle width and ventriculoperitoneal shunt.
dislocations tend to cause pelvic obliquity, and surgery has been advocated. Bilateral hip dislocations generally do not require surgical interventions. Heeg et al found that it was more important to have a level pelvis and good range of motion for ambulation then to have located hips (115).
Hip flexion contractures can be treated with soft tissue releases. Nonsurgical interventions include lying prone for 30 minutes daily. Other soft tissue surgeries designed to correct muscle imbalances have been employed. Transfers of the iliopsoas to the greater trochanter in association with adductor releases are designed to improve the hip abduction and flexion motion. Osseous surgeries may need to be done to correct acetabular dysplasia and rotational deformities (Fig. 9.9).

Figure 9.9 Bilateral hip dysplasia. Note the dysplastic acetabulum, femoral head migration, and broken Shenton's line. Ventriculoperitoneal shunt is in place.
More on the topic Hips:
- Hips
- Musculoskeletal System
- Physical Examination
- Feet
- Orthoses
- Heterotopic Ossification
- Spinal Muscular Atrophy II
- First aid for dislocation
- NEURAL TUBE DEFECTS
- GENETIC DISORDERS