TYPE I DIABETES MELLITUS (TlDM)
T1DM (Insulin-dependent diabetes mellitus) is the commonest cause of DM in childhood, with well defined diagnosis criteria (Table 22.16). Glucose tolerance test is rarely required in children except in those with obesity or suspected T2DM, to detect impaired glucose tolerance.
Epidemiologically, exact prevalence of T1DM in Indian children is not well established, probably ranging from 0.1/1000/year, lesser than in Scandinavian countries (0.35/1000/year). Most cases are identified at two peaks-first between 5 and 7 years and second during adolescence.Geographical and ethnic variations in prevalence of T1DM are probably related to variable frequency of susceptibility-genes on DQ beta chain of HLA system. Etiopathogenesis: Progressively diminishing insulin secretion due to #946;-cell destruction of pancreas is the etiological hallmark of. T1DM is a multi-factorial disease, with three important contributing factors:
a. Autoimmunity: Considerable evidence indicates autoimmune basis for #946;-cell destruction, as suggested by: (a) presence of islet cell antibodies in 80-90% cases preceding the onset of clinical disease, (b) Lymphocytic infiltration around #946;-cells on autopsy, and (c) association with other autoimmune disorders, e.g. Addison's disease, Hashimoto thyroiditis, pernicious anemia, etc. Several genetic defects involving HLA antigens on chromosome 6 have been identified to increase the risk of autoimmune T1DM.
b. Inherent genetic susceptibility: T1DM is ~100 times more common in cases with homozygous absence of aspartic acid at position 57 of HLA-DQ #946; gene. However, it is also more common in certain genotypes of HLA-DR3 and DR4. Recurrence risk is about 2-7% in siblings or offsprings, while concordance rate in identical twins is 30-50%.
c. Trigger agents: Viral infections (mumps, rubella and Coxsackie's virus), stress and exposure to chemical
TABLE 22.16: Diagnostic criteria for DM
Diabetes mellitus (any one)
• Suggestive symptoms with random BG gt;200 mg/dl
• Fasting BG level gt;126 mg/dl
• 2-hour post-prandial BG level gt;200 mg/dl
• Hemoglobin A1c #8805;6.5% on repeated testing
Impaired glucose tolerance
• Fasting BG level lt;100-125 mg/dl,
• 2-hour post-prandial BG level gt;140-200 mg/dl
BG: Blood glucose toxins are known to trigger #946;-cell destruction via direct damage, unmasking islet cell antigens or shared antigens between organism and #946;-cells.
Early introduction of cow milk has been suggested to increase the risk of T1DM in later life.According to etiology, T1DM is also classified as T1A (Autoimmune) and T1B (Idiopathic), respectively.
Pathophysiology: Insulin, secreted from #946;-cells of pancreas, is the prime regulator of blood glucose levels by its action on liver, muscle and adipose tissue. Quantum of insulin secretion is modulated by many neural, hormonal and substrate-related factors-increased in post-prandial states to augment glucose storage (glycogenesis) as well as diversion for protein and lipid synthesis; and decreased in fasting state to facilitate glycogenolysis and neoglucogenesis by counter-regulating hormones.
Progressive destruction of #946;-cells in T1DM lead to insulin deficiency and consequent metabolic disturbances, which may be sequentially described as:
• Post-prandial hyperglycemia, the earliest biochemical abnormality, due to relative lack of insulin reserve to control post-meal hyperglycemia.
• Fasting/persistent hyperglycemia in more severe cases, due to excessive glucose production in low insulin state.
• Glycosuria, once renal threshold for hyperglycemia (~180 mg/dl) is crossed, leading to osmotic dieresis and consequent features, e.g. polyuria, dehydration, dyselectrolytemia and polydipsia. Glucosuria usually appears when insulin levels drops below 20% of normal.
• Increased secretion of counter-regulating hormones: As insulin also increases cellular uptake of glucose, insulinopenia creates a state of cellular hypoglycemia, leading to increased secretion of counter-regulating hormones, e.g. ACTH, GH, epinephrine and glucagon, which accentuate hyperglycemia.
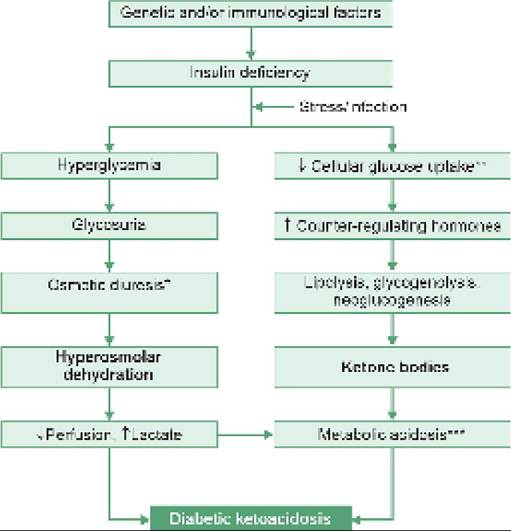
Diabetic ketoacidosis (DKA) is a state of—(a) hyperosmolarity due to hyperglycemia, (b) ketosis due to increased lipolysis and neoglucogenesis leading to accumulation of free fatty acids, which are then diverted to form ketone bodies, i.e. #946;-hydroxybutyrate and acetoacetate, and (c) acidosis due to accumulation of ketoacids and urinary loss of cations, which are excreted in urine along with ketones.
Diabetic coma is the clinical effect of progressive hyperosmolar dehydration, acidosis, electrolyte disturbances and poor glucose uptake by cerebral cells in a state of insulinopenia. A synopsis of mechanisms in diabetic pathophysiology and ketoacidosis/coma is shown in Fig. 22.7.
Clinical manifestations of DM depend on the severity of insulinopenia and rapidity of metabolic derangement. Important initial manifestations are:
• Classical tetrad of polyuria, polydipsia, polyphagia and unexplained weight loss in ~75% cases, though

Fig. 22.7: Pathophysiology of diabetic ketoacidosis
*polyuria and polydipsia. **coma, due to cerebral glucopenia ***with hypokalemia, hypophosphatemia due to urinary loss
with shorter history than in adults (lt; 1 month). Unlike adults, recurrent/persistent pyogenic infections and candidiasis are rare presenting features in T1DM.
• Diabetic ketoacidosis is a presenting emergency 15-70% of newly diagnosed cases, often triggered by a viral infection or other stress factors. Known diabetics, who have defaulted on insulin or developed uncontrolled intercurrent infection, may also present with DKA.
Clinical manifestations begin with recurrent vomiting, polyuria and abdominal pain, rapidly progressing to dehydration, metabolic acidosis (kussmaul breathing), fruity (acetonic) breathy odor, altered sensorium and coma. Important biochemical abnormalities include glucosuria, ketonuria, hyperglycemia, ketonemia and metabolic acidosis.
• Non-ketotic hyperosmolar coma is uncommon in children, presenting as severe hyperglycemia (gt;600 mg/dl) and other features of DKA, except ketosis. Absence of ketosis is attributed to severe hyperglycemia that blunts lipolytic effect of epinephrine. Focal CNS signs, e.g. seizures and hemiparesis are common, due to dehydration and hemoconcentration, leading to thromboembolic complications.
Diagnosis of T1DM depends on diagnostic criteria (Table 22.16), though other investigations are required to assess the severity of metabolic derangements and include:
• Urine examination for glucose and ketones.
• Blood glucose levels: Random estimation is enough in symptomatic cases, while fasting and postprandial levels are needed in asymptomatic/ borderline cases.
• Serum electrolytes and acid-base analysis. Hyponatremia, hypokalemia and hypophosphatemia is common in DKA, apart from metabolic acidosis.
• Investigations for precipitating/co-existing infections.
• Special investigations for confirmation of T1DM etiology, e.g. C-peptide, anti-GAD 65 antibodies etc., are rarely required in practice.
Possibility of DKA should always be considered in a child with acute onset of unexplained vomiting and progressive coma and diagnostic criteria for DKA include:
• Hyperglycemia with BG levels gt;200 mg/dL
• Metabolic acidosis (pH lt; 7.3) with serum bicarbonate lt;18 mEq/L
• Ketonemia (#946;-hydroxybutyrate gt; 3 mmol/L) or moderate/severe ketonuria (#8805; 2+)
D/D of DM includes other cause of hyperglycemia, e.g. drugs/poisonings, acute coma and renal glucosuria, e.g. Fanconi syndrome. T1DM should also be differentiated with T2DM or MODY, discussed later.
Management of T1DM presenting with DKA may be divided into 3 phases:
a. Emergency phase for management of DKA.
b. Transitional phase to normalise metabolic control.
c. Maintenance phase for long-term control of hypoglycemia.
Management of cases presenting without DKA begins with transitional phase only.
A. Emergency management of DKA aims to correct dehydration, dyselectrolytemia and acidosis as well as to initiate insulin therapy, with following steps:
1. Quick biochemical evaluation for initial severity of hyperglycemia, acidosis and electrolyte disturbances. Severity of DKA is classified as follows, to decide the need for further fluid therapy—(a) mild: pH lt; 7.3 and/or serum bicarbonate lt;18 mEq/L, (b) moderate: pH lt; 7.2 and/or serum bicarbonate lt; 15 mEq/L, and (c) severe: pH lt; 7.1 and/or serum bicarbonate lt;10 mEq/L.
2. IV fluid and electrolyte therapy, tailored with following principles:
- Amount of fluid is calculated as maintenance plus deficit.
Maintenance requirement is calculated as per body weight by Holiday-Segar formula (100 ml/kg for first 10 kg, 50 ml/kg for next 10 kg and 20 ml/kg for remaining kg), while deficit requirement is calculated based on severity of DKA, i.e. 5% (50 ml/kg), 7% (70 ml/kg) and 10% (100 ml/kg) for mild, moderate and severe DKA respectively. Deficit is corrected slowly over 24 to 48 hours.- Rate of infusion: IV fluid therapy should begin with an initial bolus of 10-20 ml/kg over 30-60 min, followed by remaining calculated fluids over next 23 hours. In patients with shock, 20 ml/kg boluses may be given rapidly.
- Type of fluid: Rapid correction of hyperglycemia and hyperosmolarity may precipitate cerebral edema due to movement of fluids into intracellular space. Hence, normal saline or Ringer lactate must be used for first-hour correction, followed by N/2 saline till resolution of DKA. Dextrose containing fluids must be used when BG levels drop lt;250 mg/kg, to prevent insulin-induced hypoglycemia.
- Potassium supplementation: Total body potassium is depleted in DKA due to its extracellular movement and urinary loss in acidosis. Correction of hydration and acidosis along with insulin therapy leads to return of K+ back into the cells, with hypokalemia. Potassium should be added in IV fluids (40 mEq/L) after first hour, after documenting urine output or normal/low serum potassium. Potassium phosphate and acetate preparations, though not easily available, are preferred over potassium chloride preparations, as chloride excess may aggravate acidosis.
- Bicarbonate therapy: Acidosis is usually corrected with fluid and insulin replacement. Bicarbonate therapy is generally contraindicated even in severe DKA, as it can worsen outcomes by causing paradoxical CNS acidosis. Bicarbonate use may be considered only in case of life-threatening hyperkalemia or unusually severe acidosis causing impaired cardiac contractility.
- Phosphate supplementation: Phosphate levels reduce in DKA due to osmotic diuresis, dilution following fluid resuscitation and insulin-mediated shift into intracellular compartment.
Hypophosphatemia may rarely cause seizures, arrhythmias and rhabdomyolysis. Hence, use of potassium phosphate may be beneficial, wherever available, particularly in case of severe acidosis, with serum phosphate levels lt; 1 mg/dl.- Sodium supplementation: while hyponatremia is common in DKA, no specific treatment is required except the use of normal saline for initial fluid therapy.
- Monitoring of these cases involve serial blood glucose and electrolyte levels, review of fluid intake/output chart and clinical monitoring, specially for signs of cerebral edema.
3. Insulin therapy should begin only after an hour of fluid therapy, which itself with reduce BG levels rapidly. Early insulin therapy may lead to drastic fall in plasma osmolality, hypokalemia and increased risk of cerebral edema.
Only regular insulin is used in DKA beginning with continuous IV infusion @ 0.05-0.1 U/kg/hr to accelerate movement of glucose into the cells. A separate IV cannula should be used for the insulin drip, and the tubing should be flushed before starting the infusion to saturate all sites. To prevent rapid fall in BG, DW 5% should be added in IV fluids once the BG levels falls to 250-300 mg/dL.
If hypoglycemia still occurs, the dextrose concentration may be increased to 10% or 12.5% rather than stopping insulin, as the main function of insulin administration in DKA is to suppress ketoacidosis. Glucose concentration must be adjusted to ensure that BG levels do not fall faster than 90-100 mg/hr.
Oral feeds must be started as early as possible, to prepare the patient for transitional phase.
B. Transitional phase begins after: (a) correction of acidosis and hypokalemia, (b) return of blood glucose levels lt;300 ml/kg, and (c) establishment of adequate oral intake.
Management of children presenting without DKA also begins with this phase, which aims to:
• Identify and treat the precipitating cause of DKA.
• Adjust the dose of regular insulin as per oral intake.
• Educate patient/parents about self-monitoring, selfinsulin injection and symptoms of hypoglycemia (insulin shock).
Insulin therapy in this phase involves replacement of IV insulin with SC injections of regular insulin 0.1-0.25 U/kg 6-8 hourly immediately before meals along with simultaneous pre-meal and 2-hour post-meal BG monitoring for next 2-3 days. 24-hour regular insulin requirement at the end of this adjustment forms the basis for doses of subsequent long-term insulin therapy.
C. Long-term management aims to provide near normal control of hyperglycemia, while avoiding hypoglycemia. Life-long subcutaneous insulin therapy is essential in all cases of T1DM, along with dietary control. Oral hypoglycemic agents are not effective in these cases. Attempts to replace parenteral insulin with oral insulin therapy or pancreatic transplant, etc. are still in experimental stage. Important principles of long-term management include:
• Insulin therapy: Old generation pork/beef insulins have been now replaced by recombinant human insulins with different onset and duration of action (Table 22.17), In DKA as well as in conditions of
TABLE 22.17: Classification of insulin preparations according to the onset and duration of action
stress, e.g. infection, surgery, etc. only rapid-acting or short-acting insulins must be used to permit quick adjustment of doses.
- Basal-bolus regimen is the preferred choice for insulin therapy in children without DKA, involving a single daily dose of long-acting Insulin (basal) along with multiple (3-4) doses of short/rapid acting insulin every day (bolus). Fixed dose combinations of short + intermediate acting insulins must be avoided in children.
Continuous subcutaneous infusion by an external insulin pump, is the preferred alternative to basal- bolus regimen, which uses only rapid-acting insulin delivered at a predetermined rate with additional boluses at meal time. Closed-loop hybrid systems to monitor BG levels using subcutaneous sensors and adjust the insulin dose automatically are also approved for use in children.
- To being with, pre-pubertal children generally require 0.7-1.0 IU#8725;kg/day of Insulin, while higher doses are needed (1-2 IU#8725;kg#8725; day) in adolescents. In basal-bolus regimen, 30-50% of total calculated daily dose must be given as a basal long-acting analog (Glargine, Detemir, Degludec) for smoother 24-hour control, while the remaining dose must distributed among pre-meal boluses of short-acting insulin (Lispro, Aspart) to prevent post-meal surge in BG levels.
- Subcutaneously insulin must be injected via special syringes or pre-filled pens over abdomen, thigh, buttocks or upper arm. Sites should be rotated periodically to avoid local lipodystrophy.
- BG monitoring before each meal is advised to decide the insulin dose based on dietary carbohydrate counting to achieve good glycemic control.
- Further modifications in basal dose depend on state of glycemic control, which should be monitored at least twice a day (pre-breakfast and pre-dinner) by glucostix in blood (Table 22.18).
• Diet: Strict dietary regulations are neither practical nor desirable in T1DM children, though it is preferable to follow certain dietary principles:
- Total caloric intake should be same as for a normal child, given as a mixture of carbohydrates (55%), fats (30%) and proteins (15%). High-fiber diet facilitates better control.
- At least 70% of carbohydrates must be given as complex starch. Refined sugar/carbonated beverages should be avoided and safety of artificial sweeteners, e.g. saccharin and aspartame, is not established in children.
• Exercise: No exercise restriction is necessary, though some cases may develop hypoglycemia during/after exercise due to increased glucose demands and/or
Basal insulin: Long acting, bolus Insulin: short acting *If vigorous physical activity expected in evening
increased insulin absorption from the injection site. It is advisable to consume additional carbohydrate- rich food items before strenuous exercise, and keep a glucose/candy or sugar-cube handy in event of hypoglycemia. In planned exercise, previous insulin dose may be reduced by 10%.
• Monitoring is an essential part of management in DM and may be divided into three components— (a) self-monitoring, (b) periodic BG monitoring, and (c) monitoring of long-term glycemic control.
- Self-monitoring is the basic tool to assess diabetic control, which requires proper parental counseling and training for regular pre-meal (and ideally postmeal too) capillary BG monitoring with glucometer. A target fasting BG of 90-130 mg#8725;dl, post-prandial BG of 140-160 mg/dl or average bed-time BG of 110-150 mg/dl is considered as optimum.
To reduce the number of pricks, continuous glucose monitoring systems (CGMS) are also available, which once fixed, function for 14 days and come with a reader which flashes the glucose reading.
- Periodic BG testing in hospital is desirable only if self-monitoring is not reliable or in poorly controlled cases. Random blood glucose levels are of no use in assessment of control.
- Long-term glycemic control is best monitored with glycosylated Hb (HbA1c) levels-a fraction of Hb, which is non-enzymatically attached to glucose in peripheral blood. Formation of HbA1c is an irreversible reaction and as the life span of RBCs is ~120 days, HbA1c levels reflect status of glycemic control in preceding 3 months. HbA1c levels of lt;7% are recommended as the indicator of optimum long-term glycemic control in children. HbA1c measurements are advisable every 3-4 months.
• Psychological support to child and family is as important as the medical treatment to ensure proper compliance and quality of life in DM.
Special issues in management of IDDM:
Honeymoon period: After initial stabilization of DKA, ~75% children show progressive reduction in their insulin requirements during next few weeks/ months (honeymoon period) before rising again. This phenomena indicates some residual #946;-cell function and insulin secretion during this period, as measured by C-peptide levels. Exact cause of DKA in these cases despite residual #946;-cell function is unclear, probably relates to sudden rise in counter-regulatory hormone levels during stress events, e.g. infections, which couldn't be compensated by borderline insulin levels.
Somogyi phenomenon denotes early-morning hypoglycemic episodes on insulin therapy, followed by hyperglycemia/glucosuria with/without ketonuria after 4-5 hours. It is believed to be due to outpouring of counter-regulatory hormones in response to early morning insulin-induced hypoglycemia. Treatment involves reduction of night time Glargine (basal insulin) dose by 10-15% to prevent early morning hypoglycaemia. Dawn phenomenon denotes early-morning hyperglycemia, not preceded by hypoglycemia (d/d Somogyi phenomenon). It is probably due to waning effect of evening insulin or normal nocturnal surge in GH/steroid secretion and must be treated by increasing night time Glargine by 10-15%.
As the treatment of somogyi and Dawn phenomena is exactly opposite, it is important of differentiate between the two, by measuring BG levels at 3, 4 and 7 AM. Absence of hypoglycemia in first two samples rules out Somogyi phenomenon.
Brittle diabetes denotes wide fluctuations in BG levels despite frequent adjustments in insulin doses. These cases may be treated by increasing frequency of insulin administration or by changing the type of insulin.
Hypoglycemic episodes (Insulin shock) are common in diabetics, due to honeymoon phase, Somogyi phenomenon, insulin overdose, fasting and strenuous exercise. These cases present with signs of sympathetic overactivity followed by neuroglycopenic symptoms, e.g. excessive sweating, palpitation, trembling and altered sensorium due to outpouring of counter-regulating hormones. Unlike DKA, hypoglycemic coma develops within few minutes and parents should be trained to recognize and treat it with immediate glucose consumption.
Infections in diabetics: Intercurrent infections or illnesses may destabilize glycemic state in T1DM, with higher risk of developing hyperglycemia and ketoacidosis despite vomiting and poor oral intake. General guidelines to manage a sick day in diabetic children are as follows:
• Do not omit the insulin dose but reduce it as per BG levels, if necessary.
• Monitor BG levels and urine ketones more frequently, at least every 4 hours.
• If BG levels exceed 300 mg/dl anytime, give additional dose of regular/rapid insulin equal to 10% of total insulin dose.
• If BG drops lt;100 mg/dl anytime, give sugar water and omit longer-acting insulin, replacing it with frequent doses of regular/rapid acting Insulin as per BG monitoring.
• Hospitalize if develops vomiting, oliguria, breathlessness or drowsiness.
Surgery in diabetics: During major surgeries, it is advised to provide continuous IV insulin infusion along with potassium-containing normal saline or N/2 saline with Dextrose 5% during intraoperative and immediate post-operative period. Patient may be switched back to original schedule after oral intake is established. However in minor surgeries, it is enough to give regular morning dose on the day of surgery and an additional dose of SC 0.25 U/kg regular insulin after surgery.
Late complications: Short stature and delayed puberty are commonest problems in IDDM, recognized during childhood. With improving survival, other late complications are also being increasing recognized after gt;15-20 years of diagnosis, e.g. retinopathy and lenticular opacities, nephropathy and neuropathy. Development of complications is directly related to status of long-term glycemic control. Rare complications include osteopenia, limited joint mobility syndrome and Mauriac syndrome (severe short stature with delayed puberty, waxy skin and hepatomegaly)
All cases of TDM should be monitored for hypertension during each visit and annually for nephropathy, retinopathy, neuropathy and dyslipidemia from 10 years of age onwards. They must also be assessed for thyroid disease (every 1-2 years) and celiac disease (at 2 and 5 years age).
Other uncommon but important forms of DM in children are as follows:
Type II diabetes (T2DM) or non-insulin dependent diabetes mellitus is the commonest type of DM in adults, due to relative insulin resistance with or without variable degree of insulin deficiency. Once considered as rarity in childhood, incidence of T2DM has shown dramatic rise in adolescents during recent years, probably due to rising incidence of obesity that blunts the insulin response. While detailed discussion of T2DM is beyond the scope of this book, important differences between T1DM and T2DM are given in Table 22.19.
Maturity onset diabetes mellitus is a heterogeneous group of autosomal dominant defects in #946;-cell functions with impaired insulin secretion in response to hyperglycemia (not the insulin resistance).
TABLE 22.19: Type I vs. Type II diabetes mellitus
Diagnostic criteria for MODY essentially include:
• History of DM in at least three generations, confirming vertical transmission of AD defect, and
• Onset or diagnosis of disease before 25 years of age.
Various mutations have been identified so far for MODY, the common ones being:
• MODY-2, involving glucokinase genes at chromosome 7p, which presents with mild chronic hypoglycemia or impaired glucose tolerance; and
• MODY-1 or-3, involving HNF-4 gene at chromosome 20q or HNF-1 gene at chromosome 12q respectively, both presenting with progressively severe diabetes and vascular complications.
Some other forms of Diabetes due to secondary causes e.g. cystic fibrosis-related diabetes (CFRD), fibrocalculous pancreatic diabetes (FCPD), drug-induced diabetes, and lipodystrophic diabetes are also recognized.
22.8