Wheelchairs and Seating
The degree of limitation in mobility varies across a broad range for people with physical disabilities (4). Over the years, technology related to wheelchair seating and mobility has enhanced the opportunities for people with disabilities.
Many more options exist to match technology with the user than ever before.In order to begin the process of matching the child's needs to a particular wheelchair, it is recommended that a thorough evaluation be made. Many factors contribute to deciding on a particular seating and mobility system for the pediatric population. These include growth, specific disability, medical interventions, and prognosis of future functional and cognitive abilities. Assess the particular needs of the child, collect medical and surgical history, and perform a physical assessment. A multidisciplinary team approach usually works best. Once the assessment is performed, educate the family on various wheelchairs relative to the child's goals. If possible, simulate the child in as close to the recommended equipment as possible. Finally, determine the particular seating objectives for the child as well as the type of mobility base (22).
Every child has a unique set of challenges that will dictate how his or her rehabilitation needs will be met. Proper seating provides stability and support, decreases the likelihood of postural deformities, and enhances upper extremity control. Within a wheelchair seating system, maintaining proper body alignment is achieved by using various seating and positioning components (23). Seating systems, including both the seat and the back, can be linear, contoured, or molded. Of the three, linear seating systems provide adjustability that allows the seating system to grow as the child grows. Linear seating systems are the least conforming to a person's body, but they are the easiest to fabricate and most adaptable as the person's orthopedic needs change.
The basic materials consist of plywood for the base, foam (which can vary in density) for comfort and pressure relief, and a covering, usually Lycra, Rubatex or Dartex. Positioners such as laterals, abductors, and adductors are easy to mount on these systems.Contour systems, in contrast to linear systems, conform closer to the actual shape of one's body. When recommending a contour system, close attention should be given to the growth rate and potential medical interventions, as the shape of the contour may not be an appropriate choice. Custom molded systems provide maximal support and should be considered for children with fixed deformities. Molded systems do not change as the child grows, unless remolding is performed, which is potentially time-consuming and costly. Although this system aids in controlling tone and nicely contours to most deformities, it has the reverse effect of limiting the amount of freedom children have in their seating system.
For patients who lack sensation, a variety of cushions exist that assist in alleviating pressure, which will decrease the likelihood of skin breakdown. Cushions fall under several categories, including foam, gel, air, and water (Table 6.4). Cushions should provide pressure relief under bony prominences, provide a stable support surface for the pelvis and the thighs, and function effectively in different climates. They should be lightweight, especially if a person is transferring independently or is a self-propeller, and be durable. Each type of cushion has advantages and disadvantages.
Pressure mapping systems are tools used by clinicians to measure interface pressures between two surfaces, such as a seated person and the cushion he or she is sitting on. (See an example of a pressure mapping system by Vista Medical at http://www. pressuremapping.com/.) A visual output on a computer monitor allows easy viewing and understanding. Using this tool allows clinicians to “diagnose” potential causes of skin ulcers as well as to select a cushion that will provide the most appropriate pressure relief for that patient.
Positioning Components
Within a wheelchair seating system, maintaining proper body alignment is achieved by using various
Cushion Types
| FOAM | GEL | AIR |
| Lightweight | Lightweight | Provides extremely |
| Provides a | Provides a stable | good pressure |
| stable base of | base of support | relief |
| support | Various densities | Lightweight |
| Various densities | available that can | Can be unstable |
| available that | improve pressure- | Requires careful |
| can improve | relieving qualities | monitoring and |
| pressurerelieving qualities Heavy Conforms to individual shape | Heavy Conforms to individual shape | maintenance |
6.4
positioning components. Evidence supports that children with cerebral palsy should be fitted for wheelchairs that place them in a functional sitting position (17). Lateral supports can be used to encourage midline trunk position when trunk control is poor. They may also be used to partially correct or delay the progression of scoliosis. Chest harnesses assist in stabilizing the trunk by anterior support as well as by preventing forward trunk flexion.
Positioning belts are used for pelvic alignment and stabilization. An improperly placed pelvic positioner is more detrimental than no positioner at all. The standard angulation of a pelvic positioning belt is at a 45-degree angle to the sitting surface (4).
Subasis bars are used primarily for high-tone patients. Proper placement and position of the bar is critical to the success of the product. Improper positioning can potentially lead to skin breakdown.Additional positioners include abductor pads that reduce or prevent increased adduction and assist in providing proper leg alignment. It should be remembered that abductors are not to be used to block a child from “sliding” out of the wheelchair. This may cause injury to the perineal area (1). Adductors decrease hip abduction and assist in providing proper leg alignment. Shoe holders and ankle positioners help control increased extension or spasms in the lower limbs and correct or prevent excessive internal or external foot rotation.
Head position is important for many reasons, including proper visual input, control of tone, and proper alignment for feeding and swallowing. Headrests provide support and positioning for a patient with poor head control due to low tone, active flexion, or hyperextension. They provide posterior and, if necessary, lateral support. They also furnish safety in transport. The size and shape of the headrest depend on individual needs. Total head support can be achieved with the same headrest that allows the child to freely move his or her head to explore his or her environment.
When proper seating and positioning components are in place, pediatric wheelchairs provide users with the opportunity to explore and experience the world around them. It encourages social integration as well as enhances the level of involvement in various school and home activities. The majority of wheelchairs can be divided into two main categories: dependent mobility and independent mobility. These categories represent the level of functional mobility the child can achieve. Strollers, recliner wheelchairs, and t ilt-in-space wheelchairs typically make up the types of chairs recommended for people who need a temporary means of mobility or who are incapable of independent mobility.
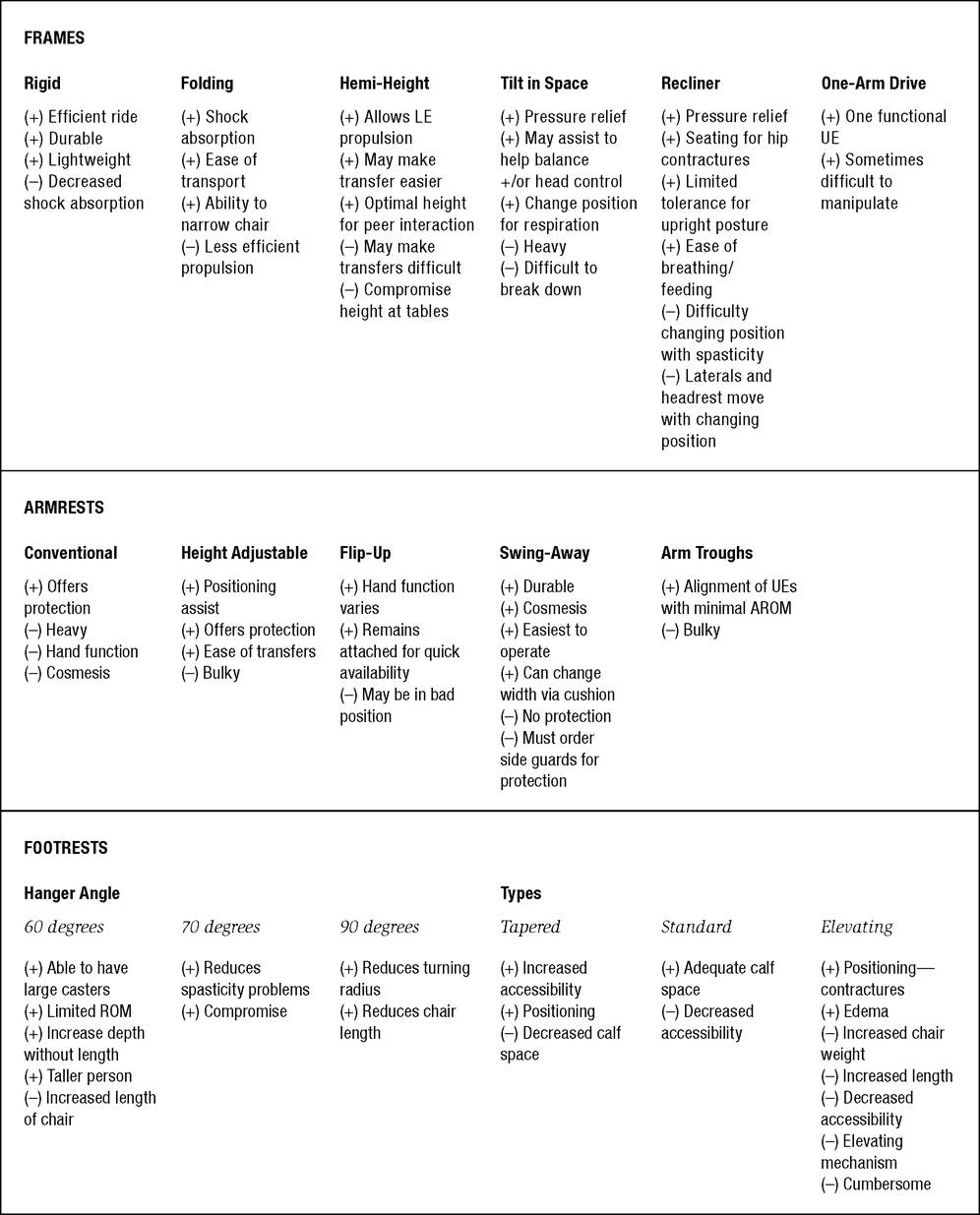
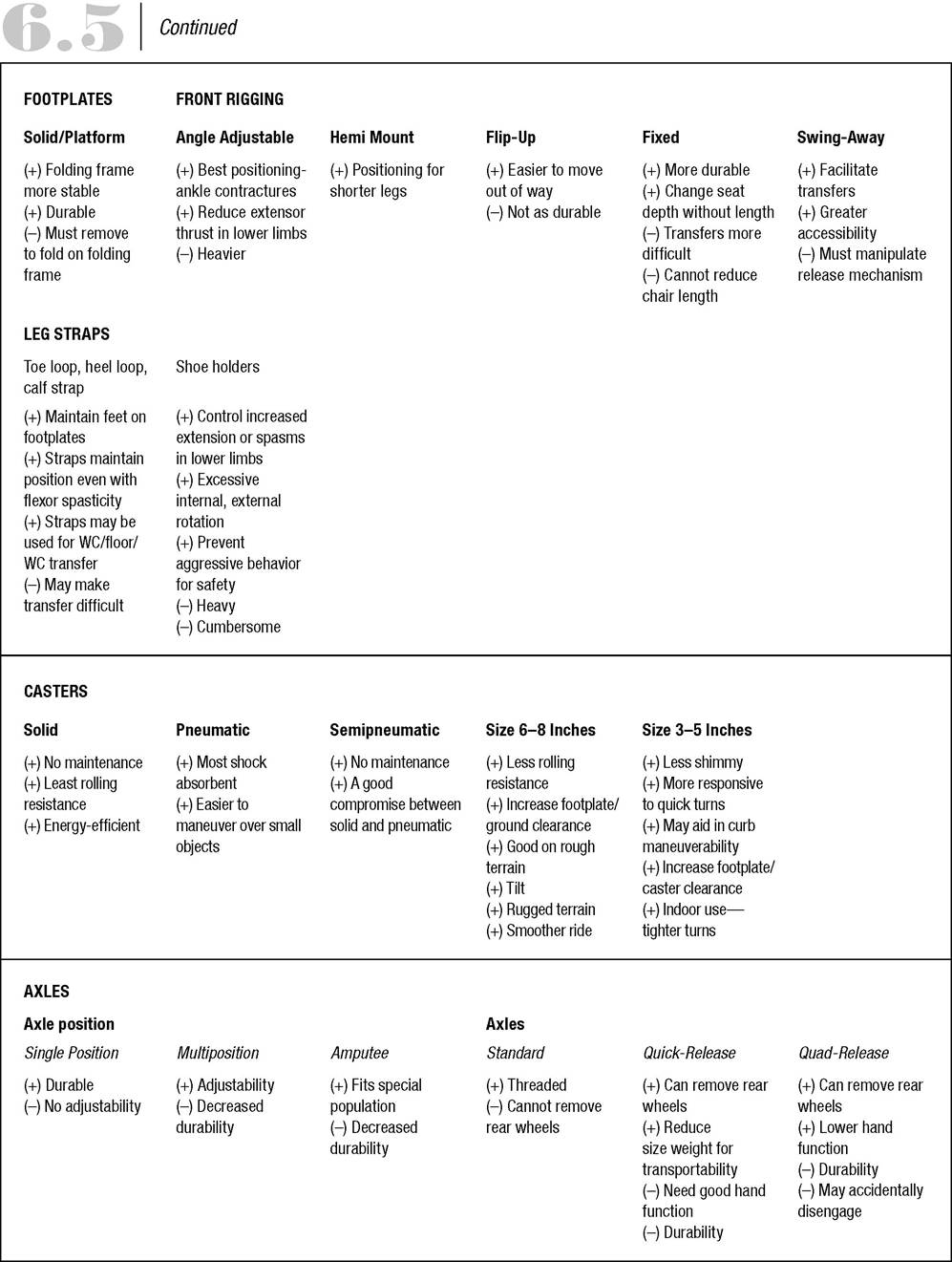
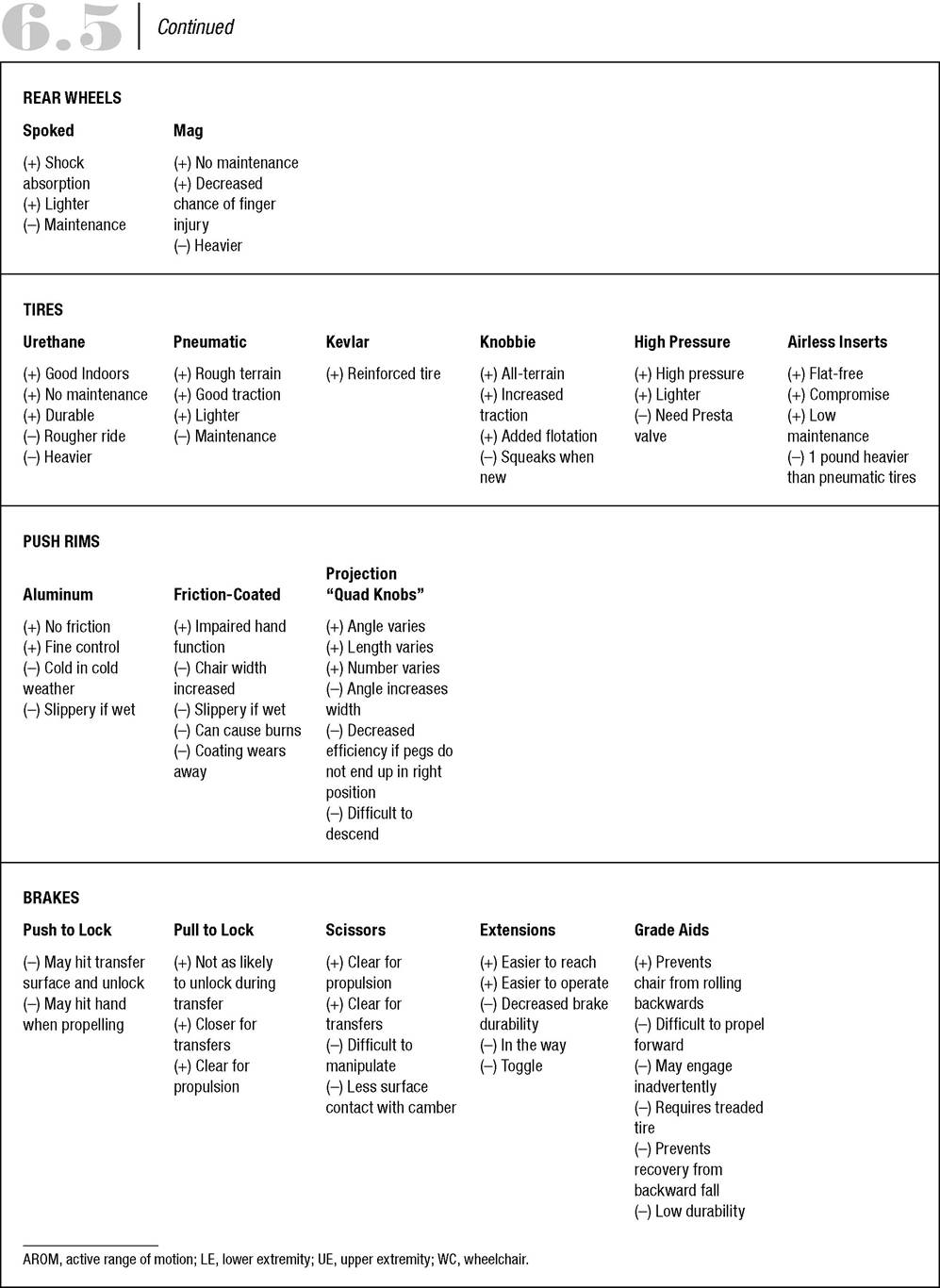
Tilt-in-space chairs, such as the Quickie IRIS (see Web site for additional information: http://www.sunrisemedical.com), are recommended for people who need moderate to maximum positioning when there is little tolerance for an upright position. A reduction of pressure readings at the ischial tuberosities with tilt and recline positioning was shown as a general trend in a study by Pellow (15. Tiltin-space chairs provide pressure relief by redistributing body weight. The tilt also can assist the caregiver in properly positioning the child in the wheelchair by allowing gravity to assist. Positioning strollers, such as the KidKart Xpress and the KIMBA (Fig. 6.3) are typically used for younger children in whom independent mobility is less of an issue. Most strollers are also easily transportable.Independent mobility can be achieved by using a manual wheelchair or a power wheelchair. Functional abilities and mobility goals dictate the type of wheelchair recommended. Manual wheelchairs can range from providing minimal support to complete postural support. Manual wheelchairs are lightweight in nature and have a multitude of features that can be adjusted or added to enhance efficient and effective use. Table 6.5 offers a comparative look at the various wheelchair components. Although this is a list of manual wheelchair components, many features can be considered for power wheelchairs as well.
Power wheelchairs provide independent mobility when manual wheelchairs cannot be used. Independent mobility is believed to be essential for perceptual-motor and social skill development. Self-produced locomotion also is believed to have an impact on cognition, communication, and psychosocial development (11). Technological advances in electronics have enabled people with severe physical disability to operate a motorized wheelchair. Power wheelchairs can incorporate unique features that enhance function critical

Figure 6.3 OttoBock KIMBA.
to health maintenance, as well as social development. The children who received power mobility had significantly greater improvement in receptive language on the Beck Depression Inventory (BDI) and in socialfunction functional skills and self-care caregiver assistance on the Pediatric Evaluation of Disability Inventory (PEDI) than the children who did not use power mobility (12). Power wheelchairs have pediatric sizes that are capable of raising the child from a seated to a standing position (for an example, see the Permobil Web site at http://www.permobilus.com), as well as elevating in the seated position using a “seat elevator.”
Some power wheelchairs lower to floor level to allow the child to socially interact with peers. However, there may be constraints to using a power wheelchair. The family may not have the means to transport the wheelchair, or the power wheelchair cannot be used in the home due to limited physical space and accessibility. Funding may also prohibit the ability to acquire a power wheelchair. Another option for powered mobility for children may lie in three- or four-wheeled scooters. Scooters are usually less expensive than a power wheelchair, but do not offer a great deal of positioning options. Although choices are limited for pediatricsized scooters, several do exist that can accommodate small children.
6.5
Wheelchair Characteristics