BACTERIAL INFECTIONS
Bordetella bronchiseptica Infection
Bordetella bronchiseptica is a major pathogen in guinea pigs of all ages. However, disease and mortality occur most often in young guinea pigs, particularly during winter.
In some outbreaks, there may be other identifiable manipulations or environmental factors that appear to precipitate disease. Guinea pigs may harbor the organism in the upper respiratory tract and trachea as an inapparent infection. In enzootically infected colonies, the prevalence of nasal shedders may be relatively high. Infection rates are usually highest in the winter months. Most animals appear to develop solid immunity and eventually eliminate the organism, but a small percentage may remain carriers. The organism is readily transmitted as an airborne infection. It has an affinity for ciliated respiratory epithelium and has been shown to cause ciliostasis in other species. During epizootics of bordetellosis, pregnant sows may die, abort, or produce stillborn offspring. Commercial and autogenous bacter- ins have been used to reduce the incidence of disease. However, it is unlikely that immunization will eliminate the carrier state.Pathology
The external nares, nasal passages, and trachea frequently contain mucopurulent or catarrhal exudate. Consolidated areas of the lung vary from dark red to gray, are cranioventral in distribution, and may involve entire lobes or individual lobules (Fig. 5.12). Mucopurulent exudate is present in affected airways, pleuritis occasionally occurs, and purulent exudate may be present in the tympanic bullae. Histologically, there is an acute to chronic suppurative bronchopneumonia, with marked infiltration by heterophils in airways and alveoli, with obliteration of the normal architecture (Fig. 5.13). Bordetella has also been isolated from a case of pyosal- pinx in the guinea pig.
Diagnosis
The organism can usually be readily recovered on blood agar cultures from the respiratory tract, affected tympanic bullae, and in cases of metritis, the uterus.
Differential diagnoses include acute Streptococcus pneumoniae, Klebsiella spp., or Staphylococcus aureus infections, as well as a systemic Streptococcus equi subsp. Zooepidemicus infection.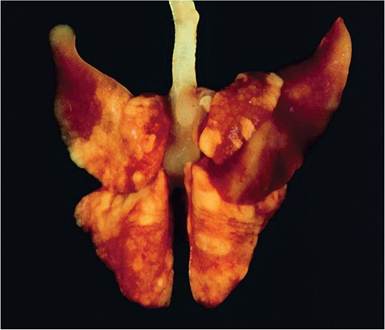
FIG. 5.12. Cranioventral bronchopneumonia in a juvenile guinea pig with acute Bordetella bronchiseptica infection.
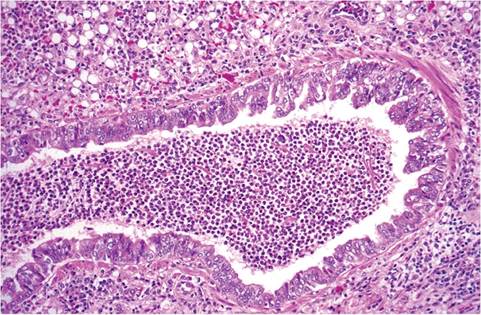
FIG. 5.13. Chronic suppurative bronchitis associated with Bordetella bronchiseptica infection in an adult guinea pig.
Brachyspira spp. Infection: Intestinal Spirochetosis
Intestinal spirochetosis due to infection with Brachyspira spp. (formerly Serpulina) has been observed on multiple occasions in guinea pigs. In 1 report that appeared to involve Brachyspira spp. as the primary pathogen, affected guinea pigs experienced rectal prolapse, sudden death, and diarrhea. Infection spread rapidly within the affected population. Subclinical infection was also observed. Gross findings typically included distention of the cecum and colon, and less commonly duodenum, with greenish-yellow or hemorrhagic liquid and mucus. Histopathology revealed hyperemia, variable necrosis, and mixed leukocyte infiltration in the cecal mucosa with diffuse colonization of cecal and proximal colonic surface mucosa with filamentous bacteria, typical of Brachyspira. Colonization of the duodenum was found in 1 guinea pig. Other reports observed Brachyspira in association with Tyzzer's disease. Brachyspira organisms densely populate end-on to the brush border of intestinal enterocytes, with displacement and reduction of microvilli. Diagnosis can be achieved by observation of the typical morphology and location of organisms or culture. Although the species of Brachyspira has not been identified in guinea pigs, PCR using porcine Bra- chyspira pilosicoli 16S ribosomal sequences is effective for confirming diagnosis in guinea pigs.
Brucella spp. Infection: Brucellosis
Guinea pigs are susceptible to Brucella spp. infection, and have been used as models of brucellosis, but natural cases are rare, since infection requires contamination of feed with animal by-products. Nevertheless, a few infections with Brucella abortus, Brucella melitensis, and Brucella suis have been observed in guinea pigs. In 1 report, a male guinea pig from a commercial vendor had testicular and joint swelling, and a female had abscesses of the liver and pancreas.
Campylobacter spp. Infection
Pregnant guinea pigs have been used to test the aborto- facient capacity of human and animal Campylobacter isolates, and experimentally infected guinea pigs have been reported to develop diarrhea. Naturally occurring subclinical infection with Campylobacter jejuni has been documented in laboratory guinea pigs.
Chlamydophila caviae Infection: Guinea Pig Inclusion Body Conjunctivitis
Chlamydophila caviae is relatively widespread in conventional colonies and pet guinea pigs. In enzootically infected colonies, clinical signs are absent, although the organism may be demonstrable in conjunctival smears. Guinea pigs 4-8 weeks of age are most frequently infected with the organism in such herds, and most adults are likely to be seropositive under these circumstances. Young seronegative animals, when introduced into a colony that is enzootically infected with C. caviae, may then develop the typical clinical disease.
Transmission is primarily by direct contact. In addition to conjunctival lesions, rhinitis and urogenital tract infections may occur. Abortions and lower respiratory tract disease have been attributed to the organism, although lung lesions may be complicated by concurrent Streptococcus or Bordetella infections. Sows with genital infections can transmit C. caviae to their offspring and infected boars can sexually transmit the organism to sows.
Pathology
The conjunctiva become reddened and swollen (Fig. 5.14), with serous to purulent exudate.
Conjunctival smears stained with the Giemsa method will reveal sloughed epithelial cells containing intracytoplasmic inclusions (Fig. 5.15) with a scattering of heterophils and lymphocytes. Genital infections in sows involve the cervix, with minimal inflammation, and oviducts, which may develop salpingitis. Inclusions are
FIG. 5.14. Guinea pig with acute Chlamydial conjunctivitis and swelling of the eyelids.
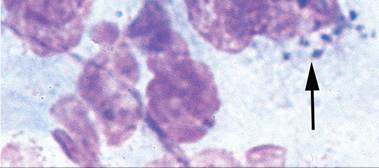
FIG. 5.15. Conjunctival swab from a case of Chlamydial conjunctivitis. Note the intracytoplasmic inclusions (arrow).
diagnostic, but may be difficult to demonstrate, particularly if preparations are smudged or there are numerous bacteria in the smear. The demonstration of antigen in conjunctival or cervical smears by immunohistochemistry using specific antibody or PCR analysis are more sensitive and reliable methods. Serology has been used to detect antibody to the organism. Bacterial culture of conjunctival swabs is recommended in an effort to differentiate guinea pig inclusion body conjunctivitis from other bacterial conjunctivitides. Possible transmission of C. caviae to a human contact has been reported, and rabbits and other species have been found to be infected with C. caviae.
Citrobacter freundii Infection
On occasion, C. freundii has been associated with septicemia in guinea pigs. An epizootic of C. freundii septicemia with high mortality has been reported in guinea pigs. Pneumonia, pleuritis, and enteritis were observed, and C. freundii was isolated from lung, liver, spleen, and intestine at necropsy. No predisposing factors or possible sources of the infection were identified. Citrobacter spp. and C. freundii have also been isolated from various lesions in hysterectomy-derived, barrier-maintained guinea pigs.
Clostridium difficile and Clostridium perfringens Enterotoxemia: “Antibiotic Toxicity,” Enterotoxemia
Guinea pigs are susceptible to C.
difficile and C. perfrin- gens typhlocolitis as a consequence of enteric dysbiosis, as well as Tyzzer's disease caused by Clostridium piliforme. Clostridium difficile is often associated with a syndrome known as “antibiotic toxicity,” in which antibiotics perturb normal microflora, allowing overgrowth of toxin-producing Clostridia.Following treatment of guinea pigs with certain antibiotics, up to 50% or more may develop a profuse diarrhea, with high mortality within 1-5 days. In guinea pigs, Gram-positive organisms such as streptococci and lactobacilli predominate in the small and large intestine. However, when a narrow-spectrum antibiotic with antibacterial activity against Gram-positive bacteria, such as penicillin, bacitracin, or ampicillin, is administered per os or parenterally, striking changes occur in the gut flora. Antibiotics such as ampicillin and penicillin are excreted, at least in part, in the bile, which explains their profound effects on the bacterial flora of the gut, even after parenteral administration. Following the administration of a single intramuscular dose of 50,000 units of penicillin, there was an estimated 100fold decrease in cultivable Gram-positive bacteria within 12 hours, followed by up to a 10,000,000-fold increase in Gram-negative bacteria. A high incidence of bacteremia due to Escherichia coli has also been observed in treated animals. In addition, clostridial overgrowth also occurs. Following treatment with penicillin or ampicillin, large numbers of C. difficile have been recovered from animals with diarrhea, and C. difficile enterotoxin has been demonstrated in the intestinal contents following treatment with penicillin. This organism is normally not present in intestinal contents of guinea pigs. Antibiotic treatment causes sufficient disruption of the gut flora (dysbiosis) to permit the proliferation of a pathogenic organism not normally recoverable from this species. The problem can be prevented by treating with broader spectrum antibiotics.
Although antibiotic treatment is the most common precipitating factor in dysbiosis leading to clostridial enterotoxemia, C. difficile has also been found to cause enterotoxemia in the absence of such treatment, and enterotoxemia has also been found to be associated with C. perfringens, type A. Regardless of precipitating factors (antibiotic, nutritional, other stressors) of dysbiosis, the pathogenesis of enterotoxemia is the same: overgrowth of toxin-producing Clostridia. Clostridium perfringens has been isolated from cases of enterotoxemia in ex-germ- free guinea pigs that had incompletely stabilized gut microflora.
Pathology
The cecum is often atonic and dilated with fluid and gaseous content. The cecal mucosa is edematous and frequently hemorrhagic (Fig. 5.16). Microscopically, there may be necrosis or mucosal hyperplasia with mononuclear cell infiltration in the lamina propria of the terminal ileum. In the cecum, there is degeneration and sloughing of enterocytes, edema of the lamina propria, and leukocytic infiltration. Focal hepatic and splenic infarction has been associated with acute infection with C. perfringens type A.
Diagnosis
A history of recent antibiotic treatment or other causes of dysbiosis and the typical gross and microscopic changes
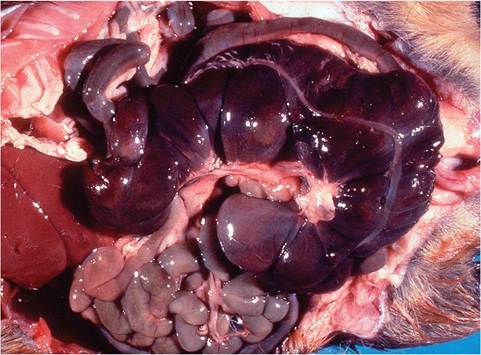
FIG. 5.16. Acute typhlitis in a guinea pig following treatment with narrow-spectrum antibiotic treatment. The cecum is hemorrhagic and distended with liquid digesta and gas.
should provide an accurate provisional diagnosis. Bacteriology and assay of cecal contents for clostridial toxins are recommended. Differential diagnoses include Tyzzer's disease, acute coccidiosis, cryptosporidiosis, viral enteritides, and bacterial enteritides.
Clostridium piliforme Infection: Tyzzer’s Disease
Guinea pigs, like all of the other species covered in this book, are susceptible to Tyzzer's disease caused by C. piliforme. Although in other species Tyzzer's disease typically involves intestine, liver, and heart, some reported cases in young guinea pigs have found lesions that were confined to the intestinal tract. In young guinea pigs inoculated orally with C. piliforme, lesions were observed in the ileum, large intestine, and liver by 4 days postinoculation. Bacilli were demonstrated in the gut lesions at 4-10 days and in the liver at 8-10 days postinoculation. Vertical transmission has been reported to occur in a hysterectomy-derived, gnotobiotically reared guinea pig. Necrotizing ileitis and typhlitis, frequently with transmural involvement, are typical findings in cavian Tyzzer's disease. Hepatic lesions, when present, are characterized by focal coagulation necrosis in periportal regions, with variable heterophil infiltration. Fascicles of intracellular bacilli are best demonstrated by the Warthin-Starry or Giemsa stains. Brachyspira sp. has been found in association with C. piliforme infections in guinea pigs in some outbreaks of Tyzzer's disease.
Corynebacterium spp. Infection
Corynebacteria appear to be a part of the normal flora of guinea pigs, but have also been occasionally associated with diseases, including Corynebacterium pyogenes septicemia in a guinea pig, and pulmonary infection by Corynebacterium kutscheri in a guinea pig during an epizootic of streptococcal disease. In addition, Corynebacterium renale was a common isolate from urine or bladder in guinea pigs with urinary calculi.
Escherichia coli Infection: Colibacillosis
As in rabbits, E. coli is not normally present in the gut of healthy guinea pigs, but has been associated with enteritis and septicemia in poorly managed colonies. Infection may be fatal, particularly in weanling animals. Necropsy findings included intestinal distention with fluid and gas, peritoneal exudation, splenomegaly, and multifocal hepatitis. Pure cultures of E. coli were obtained from blood, peritoneal fluid, and other organs. This bacterium has also been isolated from cases of mastitis and cystitis. Escherichia coli septicemia has also been found in association with clostridial enterotoxemia.
Klebsiella pneumoniae Infection
Epizootics of acute infections due to K. pneumoniae have been reported on rare occasions. Patterns of disease vary from acute septicemia to acute necrotizing bronchopneumonia, with pleuritis, pericarditis, peritonitis, and splenic hyperplasia. Klebsiella oxytoca and K. pneumoniae have been isolated from miscellaneous inflammatory lesions in guinea pigs, including mastitis.
Lawsonia intracellularis Infection: Adenomatous Intestinal Hyperplasia
Multiple species of animals, including guinea pigs, are susceptible to L. intracellularis enteric disease, which has previously been attributed to intracellular Campylobacter-like organisms. Grossly visible segmental thickening with microscopic evidence of epithelial hyperplasia of the duodenum was observed in a guinea pig on steroid treatment. Cagemates of the index case had acute enteritis without hyperplasia, but all had typical intracyto- plasmic Lawsonia-like organisms in small intestinal mucosal epithelium. An outbreak of diarrhea among 2 adults and 5 juvenile guinea pigs with weight loss, diarrhea, and mortality was also reported in Japan. Grossly, the jejunal and ileal mucosa was thickened and rugose. Histopathology revealed mucosal hyperplasia with intracellular organisms that were interpreted to be Campylobacter (Lawsonia). Organisms were observed in immature crypt epithelial cells by electron microscopy. The changes observed were similar to those seen in Lawsonia-associated enteritis in hamsters and rabbits. Warthin-Starry silver staining of tissue sections are diagnostic, revealing a typical distribution of intracellular L. intracellularis within the apical cytoplasm of infected enterocytes (see Hamster Chapter 3, “Fig. 3.16” and Rabbit Chapter 6, “Fig. 6.39”).
Leptospira spp. Infection: Leptospirosis
There are approximately 20 species of saprophytic and pathogenic Leptospira, among which Leptospira interrogans is the most common pathogenic species that infects animals and humans. Within this species are approximately 200 serovars, names of which are often used as

FIG. 5.17. Multifocal pulmonary hemorrhages in a guinea pig with disseminated leptospirosis. (Source: Reprinted from Zhang, Y., et al.
BMC Infectious Diseases. Zhang, Y., Lou, X.-L., Yang, H.-L., Guo, X.- Y., He, P. & Jiang, X.-C. (2012) Establishment of a leptospirosis model in guinea pigs using an epicutaneous inoculations route. BMC Infectious Diseases 12:20. )
species names, such as Leptospira pomona and Leptospira icterohemorrhagica. The guinea pig is commonly used as a model of leptospirosis, but natural infection is rare. Wild cavies (C. aperea) were found to have a high prevalence of L. pomona infection in association with infected cattle in Argentina. Natural infection among domestic guinea pigs, presumably through exposure to wild rats, has also been documented in Europe. Affected animals were jaundiced with disseminated hemorrhages. Mucous membranes and skin are the primary modes of entry, and guinea pigs have been shown to be readily susceptible to infection through abraded skin. Regardless of the route of infection, there is a rapid bacteremia resulting in disseminated infection, with multifocal hemorrhages in the skin, lungs (Fig. 5.17), serosa, kidneys, and perirenal tissue (Fig. 5.18). Microscopic lesions, in addition to hemorrhage and edema, include focal hepatic necrosis, and renal tubular necrosis with hematuria. Bacteria with typical spirochetal morphology can be visualized in tissues with silver stains and immunohistochemistry, and confirmation can be achieved by culture or PCR.
Listeria monocytogenes Infection: Listeriosis
Guinea pigs are used as a model of maternal-fetal listeriosis because of the similarity of their placentation to that of humans. Experimental oral infection of pregnant guinea pigs has been shown to result in abortion and stillbirth as well as focal hepatic lesions, with isolation of organisms from placenta and variably from fetuses. Naturally occurring listeriosis is a rare entity in guinea pigs, but when it does occur, it has been shown to be manifest as conjunctivitis or multisystemic disease. An outbreak with up to
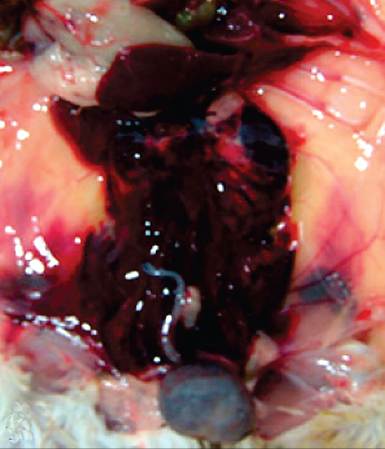
FIG. 5.18. Acute perirenal hemorrhage in a guinea pig with leptospirosis. (Source: Reprinted from Zhang, Y., et al. BMC Infectious Diseases. Zhang, Y., Lou, X.-L., Yang, H.-L., Guo, X.-Y., He, P. & Jiang, X.-C. (2012) Establishment of a leptospirosis model in guinea pigs using an epicutaneous inoculations route. BMC Infectious Diseases 12:20. )
80-100% mortality has been documented following feeding of contaminated cabbage. The intestine appears to be an important site for Listeria colonization. Experimental studies have shown that following oral inoculation, L. monocytogenes rapidly colonized the liver, with a second wave of dissemination to the mesenteric lymph nodes. Intestinal mucosa was found to be a niche for bacterial replication, with shedding into the intestinal lumen, reinfection of Peyer's patches, and trafficking of infected immune cells to the liver and mesenteric lymph nodes.
Pathology
In a natural outbreak, guinea pigs had grossly visible multifocal white nodules up to 2-4 mm in the cecum (Fig. 5.19) and liver (Fig. 5.20), with smaller foci in the stomach, small intestine, mesenteric lymph node, spleen, and uterus. Focal myocarditis has also been observed following experimental infection. Microscopically, lesions in various organs consisted of focal necrosis with mixed leukocytic infiltration and numerous Grampositive bacteria. Some of the guinea pigs had suppurative bronchopneumonia. Another report described conjunctivitis in a group of hairless guinea pigs, without systemic dissemination.
Diagnosis
Definitive diagnosis is best achieved by culture. Isolation of Listeria is enhanced when tissues to be cultured are held at 4°C for several days before inoculating culture plates. PCR methods have also been used for rapid diagnosis. Differential diagnoses include agents causing disseminated hepatic and enteric foci, including Clostridium piliforme, Salmonella spp., or Yersinia pseudotuberculosis.

FIG. 5.19. Natural case of listeriosis in a guinea pig. Note multifocal white nodules on the cecal wall. (Source: D. Driemeier.)
Mycobacterium spp. Infection: Tuberculosis
Although guinea pigs are highly susceptible to tuberculosis experimentally, natural disease is rare. Natural infections with both Mycobacterium tuberculosis and Mycobacterium bovis have been observed in guinea pigs, presumably incurred through human exposure. Lesions included enlarged bronchial lymph nodes with central caseation, as well as disseminated tubercles in lung, spleen, liver, and other lymph nodes (cervical, portal, inguinal, and prescapular). Most lesions featured caseation necrosis and stained positive for acid-fast bacilli.
Mycoplasma spp. and Acholeplasma spp. Infections
A number of cell wall-deficient bacteria, known as mol- licutes, infect cells of the respiratory and urogenital tracts of guinea pigs. Their taxonomy is in flux, as
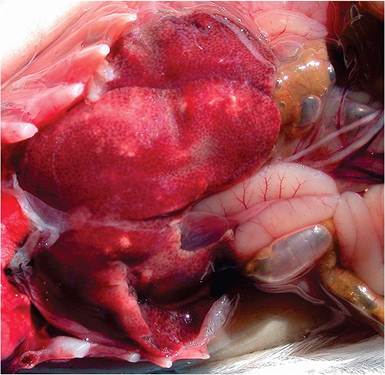
FIG. 5.20. Natural case of listeriosis in a guinea pig. Note the multifocal hepatic nodules. (Courtesy D. Driemeier.)
they do not appear to be a phylogenetically coherent group. Guinea pig isolates include Mycoplasma caviae, Mycoplasma Cavipharyngis, Mycoplasma pulmonis, Achole- plasma granularum, Acholeplasma laidlawii, and Achole- plasma cavigenitalium. Although some have been recovered coincidentally from diseased tissue, their pathogenicity is questionable.
Pasteurella multocida Infection: Pasteurellosis
Disease associated with P. multocida is rare in guinea pigs. It has been reported to cause sporadic mortality in a colony of guinea pigs, with fibrinopurulent pneumonia, pleuritis, pericarditis, peritonitis, and conjunctivitis. Disease manifestations resembled those of S. pneumoniae.
Pseudomonas and Aeromonas Infection
In a single report, pulmonary botryomycosis in 2 guinea pigs was attributed to Pseudomonas aeruginosa infection. Sulfur granules were present within the focal suppurative pulmonary lesions. An outbreak of septicemic disease in which Aeromonas (formerly Pseudomonas) caviae was isolated has been documented, and Koch's postulates were fulfilled with this isolate.
Salmonella spp. Infection: Salmonellosis
Salmonellosis in guinea pigs was once very common, but is now rare among laboratory guinea pigs due to current standards of husbandry and hygiene. It continues to be a threat to pet guinea pigs that are fed contaminated greens. There are 2 major species of Salmonella— Salmonella enterica and Salmonella bongeri—and numerous serotypes. Salmonella enterica serotype Typhimurium and S. enterica serotype Enteritidis are the most common isolates from guinea pigs, but a number of other serotypes have been documented to infect guinea pigs. Outbreaks of salmonellosis spread rapidly within a population. Guinea pigs of all ages and strains are susceptible, but young weanlings and sows around farrowing time are particularly at risk. Inapparent carriers may occur. Recovered animals may shed the organism intermittently in the feces. Ingestion of contaminated feces or feed is considered to be the usual source of infection, but the conjunctiva has been shown to be an important portal of entry as well.
Aside from the dangers of interspecies spread, the zoonotic potential must be emphasized. A recent outbreak of salmonellosis occurred in the United States among humans consuming contaminated guinea pig meat. Strict hygienic measures and the culling of all contact animals have been used to eliminate the organism from an infected colony.
Pathology
Clinical signs include depression, conjunctivitis, abortions, and sudden death in young guinea pigs. Diarrhea is often not experienced. A mortality rate of 50% is common, but has been known to reach 100%. Gross lesions include pinpoint to several millimeter diameter pale foci on the liver and spleen. Mesenteric lymph nodes may be enlarged and splenomegaly frequently occurs. Necrotic miliary foci may also be present in other viscera, including lung, pleura, peritoneum, and uterus. Lesions may be absent in peracute cases. Histopathologic lesions feature multifocal granulomatous hepatitis, splenitis, and lymphadenitis, with infiltration by histiocytic cells and heterophils. Focal suppurative lesions may also occur in lymphoid tissues of the intestinal tract.
Diagnosis
Culture of the organism from heart blood, spleen, and feces is best accomplished with media selective for Salmonella. In the absence of bacteriology, the characteristic paratyphoid nodules seen in organs such as liver and spleen are useful morphologic criteria. Differential diagnoses include C. piliforme, S. pneumoniae, Yersinia enterocolitica, and L. monocytogenes.
Staphylococcus aureus Infections: Staphylococcosis
Staphylococcus aureus is largely an opportunistic pathogen in guinea pigs. Guinea pigs are known to have a high prevalence of subclinical nasal colonization with S. aureus, which also readily contaminates the animals' environment. Guinea pigs have been found to be carriers of the same phage types as their human handlers. Diseases that are related to S. aureus include pododermatitis, exfoliative dermatitis, pneumonia, mastitis, and conjunctivitis.
Pododermatitis
Pododermatitis (bumble foot) is frequently associated with coagulase-positive S. aureus infections in a number of species, including guinea pigs. Predisposing factors include trauma due to defective or rusty cage wire, and poor sanitation. The plantar surfaces of the forefeet typically are swollen, painful, and encrusted with necrotic tissue and clotted blood. In some advanced cases, amyloid deposition has been observed in the spleen, liver, adrenals, and islets.
Staphylococcal Dermatitis: Exfoliative Dermatitis
Staphylococcal dermatitis (exfoliative dermatitis) has been observed in guinea pigs infected with coagulasepositive S. aureus, characterized by alopecia and erythema in the ventral abdominal region, with exfoliation of the epidermis. There was an age-related variation in mortality that was negligible in adults and relatively high in young animals, particularly those born to affected dams. Skin lesions usually regressed in survivors within 2 weeks, with subsequent new hair growth. At necropsy, there was erythema and hair loss, with dull red scabs and cracks in the epidermis, particularly along the ventral abdomen and the medial aspect of the extremities. On microscopic examination, there was marked epidermal cleavage, with parakeratotic hyperkeratosis and minimal inflammatory response. Staphylococcus aureus was isolated from the lesions in the majority of affected animals, and the disease was reproduced in young guinea pigs inoculated with S. aureus isolated from an affected animal. The organism was also isolated from the upper respiratory tract and pharynx of many of the affected animals and from clinically normal guinea pigs. Abrasions of the skin may have been an important predisposing factor, resulting in colonization and invasion of the epidermis. This condition was reported to occur most frequently in strain 13 guinea pigs.
Streptobacillus moniliformis Infection
Streptobacillus moniliformis, the agent of rat bite fever, has been isolated from a few cases of cervical lymphadenitis, abscesses, and from a young guinea pig with pyogranu- lomatous bronchopneumonia. Suppurative lesions contained caseous to creamy exudate and were similar to those associated with streptococcal infections.
Streptococcal Infections
A number of different Streptococcus spp. are important pathogens in guinea pigs, particularly S. equi subsp. zooepidemicus, and S. pneumoniae. In addition, Streptococcus pyogenes has been reported as a pathogen in guinea pigs. Streptococcus spp. are termed alpha-hemolytic when grown on blood agar and colonies turn the underlying agar dark or greenish, as is the case with S. pneumoniae. When termed beta-hemolytic, the colonies completely lyse the surrounding agar, as is the case with S. equi, Streptococcus equisimilis, and S. pyogenes. Furthermore, beta-hemolytic streptococci are differentiated by their cell wall carbohydrate antigens into Lancefield groups. Guinea pigs are known to be infected with Lancefield group A (S. pyogenes) and group C (S. equi, S. equisimilis) streptococci.
Streptococcus equi subsp. Zooepidemicus Infections: Cervical Lymphadenitis, Septicemia
The lay term for this infection is “lumps,” since this organism commonly causes cervical lymphadenitis. The organism may be carried in the nasopharynx and conjunctiva as an inapparent infection. Sows have been shown to be more susceptible to disease than males, and there is a strain-related variation in susceptibility. Steroid treatment does not appear to increase susceptibility to the disease. Lymphadenitis has been produced consistently in guinea pigs inoculated sublingually with S. equi subsp. zooepidemicus. The usual route of invasion appears to be via abrasions in the oral mucosa, but inhalation, skin abrasions, and invasion of the genital tract at farrowing are other possible portals of entry. The disease has also been produced in young guinea pigs by inoculation of the intact nasal and conjunctival mucous membranes. Following penetration of the oral mucosa and invasion of the underlying tissue, the organism is likely transported to the draining cervical lymph nodes via the lymphatics. The pyogenic organisms then proliferate, producing a chronic suppurative inflammatory process.
Pathology
Affected adults usually have lesions confined to the regional lymph nodes. In the localized form of the disease, there is bilateral enlargement of the cervical lymph nodes. The nodes are freely movable, firm to soft, and frequently nonfluctuant, and they contain thick purulent exudate (Fig. 5.21). Localized abscessation involving other sites such as mesenteric lymph nodes is an infrequent finding. Retroorbital abscessation, accompanied by exophthalmus, is another possible manifestation of the disease. Otitis media may also occur. Occasionally, there is an acute systemic form of the disease, particularly in younger animals. In this case, fibrinopurulent bronchopneumonia, pleuritis, and pericarditis may be present at necropsy. On rare occasions, arthritis and abortions have been attributed to S. equi subsp. zooepidemicus infections. Microscopically, changes present in the cervical lymph nodes are those of a chronic suppurative lymphadenitis with central necrosis, peripheral fibrosis, and marked infiltration with heterophils. In the acute systemic form, fibrinopur- ulent pericarditis, focal myocardial degeneration, focal hepatitis, and acute lymphadenitis may be evident on histologic examination.
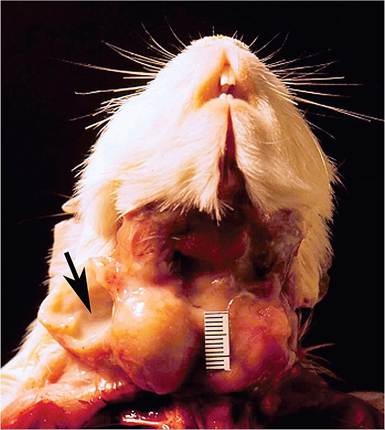
FIG. 5.21. Bilateral suppurative cervical lymphadenitis in a guinea pig infected with Streptococcus equi subsp. zooepidemicus. Note the purulent exudate (arrow) in the incised lymph node.
Diagnosis
The typical beta-hemolytic streptococci can usually be recovered from affected tissues, except in some cases of chronic lymphadenitis of some duration. Differential diagnoses in the acute systemic form of the disease include S. pneumoniae, S. pyogenes, and acute B. bronchiseptica infection. Cervical lymphadenopathy must also be differentiated from lymphoma, which frequently involves the cervical lymph nodes.
Streptococcus pneumoniae Infection: Diplococcal or Pneumococcal Infection
Pneumococcus (aka diplococcus) infections can be an important cause of disease and mortality in enzootically infected guinea pig colonies. Streptococcus pneumoniae is a lancet-shaped, Gram-positive encapsulated coccus that occurs in pairs and short chains. Capsular polysaccharide type 19 is most frequently isolated from guinea pigs. Type 4 has also been identified. Serotypes isolated from guinea pigs are identical to human isolates. The possibility of interspecies transmission is, therefore, feasible, but not proven.
Pneumococcal infections have been recognized to occur in guinea pigs for decades. In enzootically infected colonies, up to 50% of the animals may be subclinical carriers, with colonization of the upper respiratory tract. Transmission is primarily by aerosols. Epizootics occur most often during winter months, and younger animals and pregnant sows are particularly at risk. Other predisposing factors include changes in environmental temperature, poor husbandry, experimental procedures, and inadequate nutrition. During epizootics, high mortality, abortions, and stillbirths may occur. The organisms do not produce toxins but are protected from phagocytosis primarily through their abundant polysaccharide capsules. Many pneumococci can activate the alternate complement pathway; thus complement activation may be the important stimulus for the early tissue changes.
Pathology
Clinical signs are varied, including listlessness, nasal and ocular discharge, torticollis, dyspnea, abortions, and stillbirth. At necropsy, lesions include upper respiratory exudation, otitis media, fibrinopurulent pleuritis, pericarditis, peritonitis (Fig. 5.22), and marked consolidation of affected lobes of lung. Microscopic changes are those of an acute bronchopneumonia with fibrinous exudation and polymorphonuclear cell infiltration. Thrombosis of pulmonary vessels may occur in acute cases. Infiltrating cells may be elongated and fusiform, forming pallisading patterns within affected airways and alveoli. Splenitis, fibrinopurulent meningitis, metritis, focal hepatic necrosis, lymphadenitis, and ovarian abscessation have also been observed. Streptococcus pneumoniae- associated suppurative arthritis and osteomyelitis have also been reported to occur in guinea pigs with borderline vitamin C deficiency.

FIG. 5.22. Acute fibrinopurulent peritonitis in a young guinea pig
infected with Streptococcus pneumoniae.
Diagnosis
Direct smears of Gram-stained inflammatory exudate should reveal the typical Gram-positive diplococci. Using blood agar or enrichment media, the organism should be recoverable from affected tissues (S. pneumoniae is more fastidious in growth requirements than are most other streptococci). Differential diagnoses include acute septicemia due to S. equi subsp. zooepidemicus, and acute B. bronchiseptica infections.
Streptococcus spp. Infections: Hemorrhagic Septicemia
Septicemic S. pyogenes infection has been reported to cause high mortality in a colony of adult, suckling, and weanling guinea pigs. The disease particularly involved adults. Animals were seen to bleed from the nose, mouth, and vagina. Necropsy revealed necrohemorrhagic and fibrinopuru- lent pneumonia with abscessation, hemopericardium, hemothorax, petechiation of heart and kidneys, and suppurative metritis. Culture of lung and other organs yielded S. pyogenes. A nearly identical syndrome, which also featured gastrointestinal hemorrhages, was associated with a beta-hemolytic group C streptococcus. The authors suggested that the organism was related to S. equisimilis. Differential diagnoses for disseminated hemorrhagic lesions include leptospirosis and hypovitaminosis C.
Yersinia pseudotuberculosis Infection: Pseudotuberculosis, Yersiniosis
Spontaneous outbreaks of disease and mortality due to Y. pseudotuberculosis are relatively rare. Inapparent carriers may occur. In the acute form of the disease, miliary, creamcolored nodules are present in the intestinal wall and liver
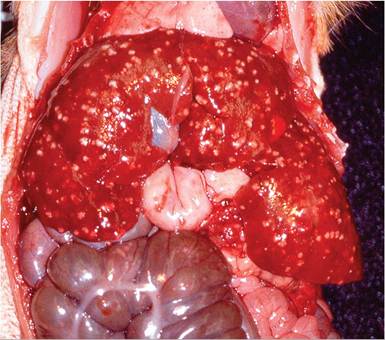
FIG. 5.23. Yersinia pseudotuberculosis infection. Note the multiple pale nodules in the wall of the cecum and throughout the liver. (Source: D. Agnew, Michigan State University, East Lansing, Michigan. Reproduced with permission from D. Agnew.)
(Fig. 5.23), with enteritis and mucosal ulceration, particularly in the terminal ileum and cecum. Pulmonary involvement may result in acute pneumonia. In the subacute and chronic forms of the disease, miliary to caseous lesions may be present in mesenteric lymph nodes, spleen, liver, and lung. Recovery and identification of the organism are necessary to confirm the diagnosis. Infection arises through contamination of feed (especially greens) by infected wild birds and rodents.
Miscellaneous Bacterial Syndromes
Otitis Media
Middle ear infections frequently go undetected clinically in the guinea pig. Careful examination of the tympanic bullae should be performed as a routine procedure at necropsy in order to detect subclinical cases. The otosclerosis associated with chronic middle ear infection may be detected antemortem by radiographic examination. Otitis media appears to be more common in colonies harboring pathogens in their upper respiratory tract. Organisms isolated from these cases include S. pneumoniae, S. equi subsp. Zooepidemicus, B. bronchiseptica, and P. aeruginosa, among others.
Bacterial Mastitis
Mastitis occurs sporadically in colonies of guinea pigs, particularly in sows during early lactation. Cases are usually sporadic and are not particularly contagious. The offspring may be unaffected. Affected glands are red to purple, enlarged, firm, congested, and edematous on the cut surface. In sows with acute mastitis, lesions are characterized microscopically by mild degeneration to necrosis of ductal epithelium, with marked heterophil infiltration in ducts and alveoli, with a scattering of inflammatory cells in the interstitium. In chronic cases, there may be marked interstitial fibrosis, with mononuclear cell infiltration and obliteration of the normal architecture in severely affected areas. In 1 study, bacteria most frequently isolated (in decreasing order of frequency) were E. coli, K. pneumoniae, and S. equi subsp. zooepidemicus.
Bacterial Conjunctivitis
Aside from Chlamydophila, organisms isolated from cases of bacterial conjunctivitis include S. equi subsp. zooepi- demicus, S. pneumonia, Salmonella spp., E. coli, S. aureus, P. multocida, Corynebacterium spp., and Actinobacillus spp, among others. In addition to culture, conjunctival smears should always be examined to ensure that there is not a concurrent chlamydial infection.