Bone growth, remodeling, and repair
Bone growth
As bone grows, there is constant internal and external remodeling that takes place in the epiphyseal plate. The epiphyseal plate remains constant in size since new cartilage is produced in the zone of proliferation, while a similar amount of cartilage is removed in the zone of resorption due to the action of osteocytes.
The resorbed cartilage is replaced by spongy bone produced by osteoblasts found between the zone of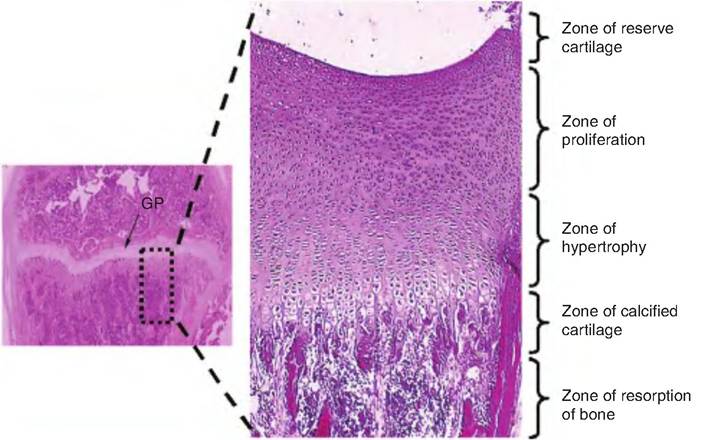
Fig. 6.8. Epiphyseal plate. The area between the diaphysis and epiphysis is the growth plate (GP), and it is characterized by distinct zonation as shown in this longitudinal section.
resorption and the diaphysis. As the cells in the proliferative region divide, an increase in length of the bone occurs as the epiphysis is moved away from the diaphysis.
The width of bone is increased by appositional growth of bone that occurs between the cortical lamellae and the periosteum as bone resorption occurs on the endosteal surface of the outermost region of the bone. As bones elongate, they are constantly remodeling, which involves resorption of bone in some areas concomitant with deposition in other areas.
Eventually, new cartilage production ceases. The cartilage that is present in the epiphyseal plate is converted to bone until no more cartilage exists. This is termed epiphyseal closure, and growth of the bone is complete. The only remaining cartilage is at the articular (i.e., regions where bones form joints) surfaces on the bone. The epiphyseal plate now becomes the epiphyseal line.
The major hormone controlling bone growth in young animals is growth hormone that is released from the anterior pituitary gland. Excessive secretion of growth hormone can cause gigantism, whereas hyposecretion can cause dwarfism.
Thyroid hormones also play an important role in bone development. The action of these hormones is discussed in Chapter 12.Bone remodeling and repair
While bone may appear to be dormant after animals reach adulthood, this is not true. In fact, bone remains very active and is constantly being broken down (resorbed) and replaced in response to various physical or hormonal changes. This constant breakdown by osteoclasts and formation by osteoblasts is termed remodeling and occurs at both the periosteal and endosteal surfaces.
The breakdown of bone by osteoclasts is called bone resorption. In this process, osteoclasts first bind tightly to the surface of the bone (either the endosteum or periosteum), forming a leakproof seal. The osteoclasts release lysosomal enzymes and acids into this sealed region, which then digest the collagen fibers and organic matrix while the acid digests the minerals. The tight seal of the osteoclast to the bone surface prevents leakage of the enzymes and acids to undesired areas. The digested components are engulfed by the osteoclasts via endocytosis, packaged into vesicles, translocated across the osteoclast by the process of transcy tosis, and released by exocytosis into the interstitial space whence the material is absorbed into the capillaries. The canal that is formed establishes the future Haversian system. Eventually, the osteoclasts are replaced by osteoblasts that rebuild the bone.
Hormonal control
The control of bone homeostasis is poorly understood. Since bones are a major calcium storage site, calcium homeostasis plays an important role in bone mineralization (Fig. 6.9). The two hormones involved in calcium homeostasis are parathyroid hormone (PTH), produced by the parathyroid glands, and calcitonin, from the parafollicular cells (C cells) of the thyroid gland. PTH is released in response to low-plasma ionic
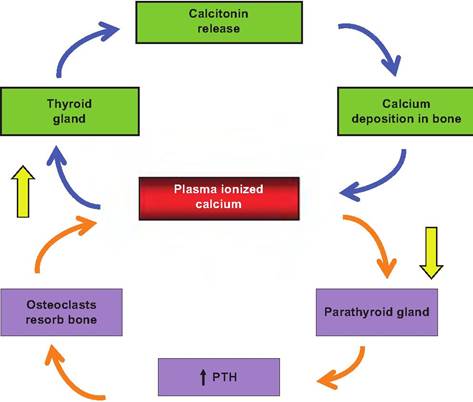
Fig. 6.9.
Hormonal control of plasma ionic calcium concentration. An increase in plasma ionic calcium concentration results in the release of calcitonin from the thyroid gland. Calcitonin stimulates calcium deposition in bone. In contrast, a decrease in plasma ionic calcium concentration stimulates the release of parathyroid hormone (PTH) from the parathyroid glands, which promotes osteoclast activity resulting in an increase in plasma ionic calcium levels.calcium levels, while calcitonin is released when plasma ionic calcium levels rise.
If resorption is excessive, bones become weak, such as in osteoporosis. Abnormally predominant deposition can produce anomalies such as bone spurs. Estrogens are known to reduce bone resorption whereas PTH promotes bone resorption. The decrease in estrogen level associated with menopause is linked with a weakening of the bones.
Repair of fractures
Fractures can be classified in several ways:
• Bone end alignment. If the bone ends remained aligned following a fracture, it is called a nondisplaced fracture. Displaced fractures occur when the bone ends are out of alignment.
• Degree of break. If the break is all the way through the bone, it is termed a complete fracture; if not all the way through, it is an incomplete break.
• Orientation of the break. If the break is parallel to the long axis, it is a linear fracture; if it is perpendicular to the long axis, it is a transverse fracture.
• Skin penetration. If bone protrudes through the skin, it is an open, or compound, fracture. A nonprotruding break is called a closed, or simple, fracture.
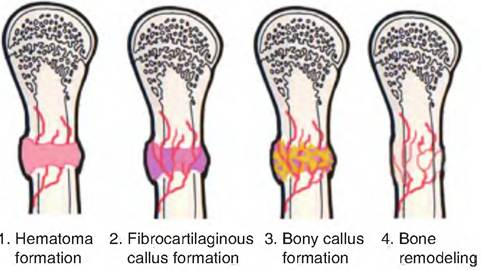
Fig. 6.10. Steps in fracture repair.
The repair process for a fractured bone involves four steps (Fig. 6.10):
1. Hematoma formation. As a result of a fracture, the blood vessels tear, causing the formation of a hematoma, a mass of clotted blood, at the fracture site.
Bone cells begin to die and the site shows the classic signs of inflammation, that is, pain, swelling, redness, and loss of function.2. Fibrocartilaginous callus formation. Capillaries grow into the hematoma from which phagocytic cells invade and remove the debris. Fibroblasts and osteoblasts migrate into the fractured area from the periosteum and endosteum. The fibroblasts form collagen fibers, which serve to span the space in the break, thus connecting the two ends. As the fibroblasts differentiate into chondroblasts, they secrete cartilage matrix. Finally, osteoblasts close to the capillaries begin forming spongy bone; those found further away secrete a bulging cartilaginous matrix. This entire mass, called a fibrocartilaginous callus, spans the fractured area.
3. Bony callus formation. Bone trabeculae begin to appear as a result of the actions of the osteoblasts converting the fibrocartilaginous callus into a bony callus made of spongy (or woven) bone. Bony callus formation continues until the two ends of the bone are firmly attached.
4. Bone remodeling. Remodeling begins during bony callus formation and continues until the bony callus is complete. Excess material is removed from both the periosteal and endosteal area, and compact bone is formed along the shaft. Normally, the final product has the same shape as the original bone.
Response to mechanical stress
Bone deposition can occur not only in response to a bone injury, but also when additional strength is needed. This can occur in response to new physical
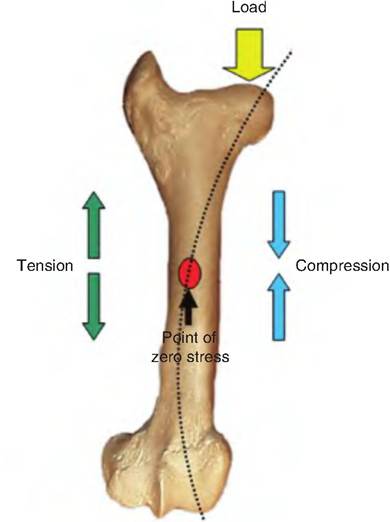
Fig. 6.11. Mechanical stress on bone. Using the femur as an example, the bone is acted upon by the load of the body weight. This load is transmitted through the bone as indicated by the dashed arc. This causes compression on one side of the bone while stretching the other side. These two forces sum to zero in the middle of the bone, creating the point of zero stress.
pressures placed on the bone as would take place if the bone is bearing weight at a different angle. Wolff's law states that a bone grows or remodels in response to forces placed on the bone. Such forces include weight bearing on the bone or muscles pulling on the bone. Since such forces are generally off-center, they tend to bend the bone. In response, the compact bone thickens on one side while thinning on the other side through the remodeling process. Spongy bone forms in the middle since mechanical forces acting on the bone sum to zero in this region (Fig. 6.11).
Nutrients necessary for bone deposition
Bone deposition requires vitamin C for collagen synthesis, vitamin D for calcium absorption in the gut, and vitamin A for bone deposition and removal, in addition to calcium, phosphorus, magnesium, and manganese.