Cases
Case 1
Signalment/history
A 7-month-old, male German Shepherd Dog presented for generalized lymphadenomegaly.
Clinical examination
The dog appeared alert and in good clinical condition.
CBC and clinical chemistry were unremarkable except for a mild hyperproteinemia (8.63 g/dl [86.3 g/l]). The dog had not traveled outside of southern Italy. FNAs were taken from the popliteal lymph node.Cytologic description of the popliteal lymph node aspirate
Figure 5.83 shows a mixed lymphoid population composed of small lymphocytes, a plasma cell, and few large blasts. Closer magnification (Figure 5.84) reveals a mixed population of small lymphocytes, some with a unipolar cytoplasmic tail (red arrows) suggestive of a T cell origin. Several plasma cells (black arrows) and a large blast are visible. Note the black pigment in the background suggestive of melanin.
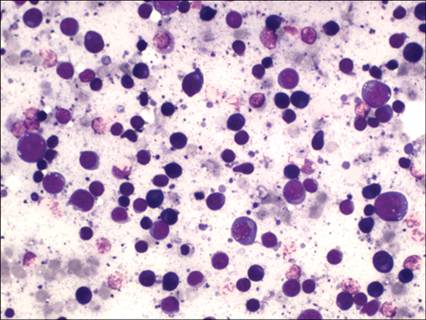
Figure 5.83 Dog, FNA from the popliteal lymph node. Presence of a mixed population composed of small lymphocytes, plasma cells, and few large blasts (May–Grünwald–Giemsa, 400? magnification).
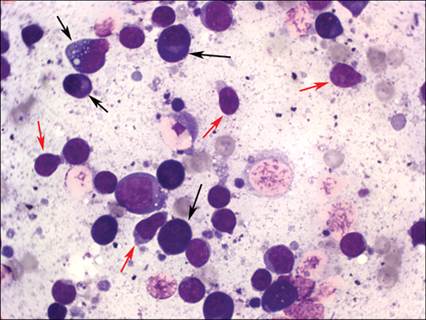
Figure 5.84 Dog, FNA from the popliteal lymph node. A mixed population of small lymphocytes, some with a unipolar cytoplasmic tail (red arrows) suggesting a T cell origin, several plasma cells (black arrows), and a large blast are visible. Note the black pigment in the background suggesting melanin (dermatopathic lymph node) (May–Grünwald–Giemsa, 1,000? magnification).
Cytologic interpretation
Based on the young age, the presence of a plasma cell, hyperplasia, hyperproteinemia, and location (southern Italy), a tentative diagnosis of canine leishmaniasis was made.
Bone marrow was aspirated to search for the causative agent (Figure 5.85). 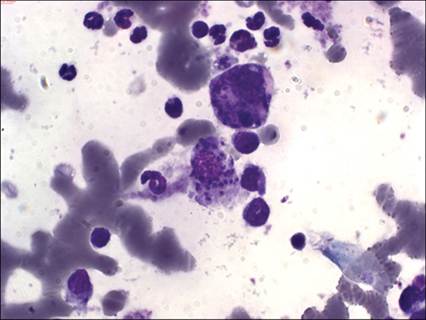
Figure 5.85 Dog, bone marrow aspirate. Two large macrophages containing several Leishmania amastigotes are found. Myeloid hyperplasia is visible in the background (May–Grünwald–Giemsa, 1,000? magnification).
Cytologic description of the bone marrow aspirate
Two large macrophages containing several Leishmania amastigotes are found. Myeloid hyperplasia is visible in the background.
Cytologic interpretation
The final diagnosis was canine leishmaniasis.
Outcome
The dog was treated for leishmaniasis with allopurinol and meglumine antimoniate. Lymphadenomegaly, after a mild remission, persisted. Three months after the first admission, lymphadenomegaly increased and a subcutaneous nodule on the back appeared. An FNA was performed from the nodule and the enlarged lymph nodes (Figure 5.86).
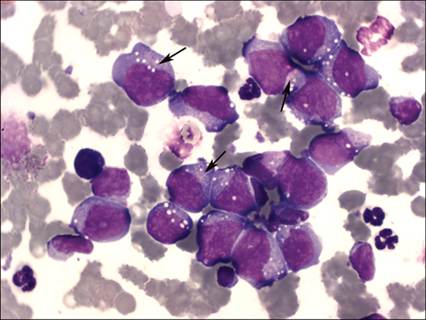
Figure 5.86 Dog, lymph node, FNA. There were several large blast cells with abundant deeply basophilic cytoplasm, often vacuolated, oval to indented nuclei with smooth chromatin, and several prominent nucleoli. Some fine pink/purple granules are visible in the juxtanuclear area (arrows). The same cells were found in the cutaneous lesion (May–Grünwald–Giemsa, 1,000? magnification).
Cytologic description of an enlarged lymph node
There are several large blast cells with abundant deeply basophilic cytoplasm, often vacuolated, oval to indented nuclei with smooth chromatin and several prominent nucleoli. Some fine pink/purple granules are visible in the juxtanuclear area. The same cells are found in the cutaneous lesion.
Cytologic interpretation
A final diagnosis of high-grade lymphoma was made. Immunophenotyping was not performed but the morphologic aspect of the cells (abundant cytoplasm, indented nuclei, juxtanuclear azurophilic granules) suggests a possible T-cell lineage.
Discussion
Due to the rapid deterioration of the dog’s condition, the owners elected for euthanasia.
The association between canine leishmaniasis and canine lymphoma is not rare in endemic areas (Foglia Manzillo et al., 2008) but reports are anecdotal and there are no specific studies to clarify if a higher prevalence of lymphoma is present in dogs with leishmaniasis. Possible pathogenic mechanisms for this are debated since either canine leishmaniasis could lead to persistent immune stimulation, thus promoting neoplastic transformation, or lymphoma could induce immunosuppression, which might promote the onset of leishmaniasis (Kopterides et al., 2007). In the present case, after a re-evaluation of the slides, a few neoplastic cells were already present in the first cytologic smear; therefore concurrent occurrence of the two diseases being merely coincidental cannot be excluded. The two cytologic patterns were superimposed in the first presentation and the detection of the causative agent directed therapy toward the infectious disease. The antiprotozoal therapy could have exacerbated the underlying lymphoma.
CASE 2
Signalment/history
A 6-year-old, male Boxer was brought to a private veterinary clinic with a huge wound in the cervical area.
Clinical examination
The dog appeared alert and generalized lymphadenomegaly was detected. Blood samples for CBC and clinical chemistry revealed a moderate nonregenerative, normocytic normochromic anemia (PCV = 25.4% [0.25 l/l]), and a moderate neutrophilia (PMNs = 14 ? 103/μl) with a left shift. Circulating lymphocytes were within reference intervals (4.2 ? 103/μl). Clinical chemistry was unremarkable.
Diagnosis and initial treatment
A diagnosis of septic suppurative pyodermatitis, probably due to trauma, was made and antibiotic therapy was administered with amoxycillin and clavulanic acid. After 15 days, the clinical condition improved and the neutrophil count returned to within the reference interval, but lymphadenomegaly persisted and the lymphocyte count increased to 7.1 ? 103/μl.
Peripheral lymph nodes (prescapular and popliteal) were biopsied using an FNA technique (Figures 5.87 and 5.88). 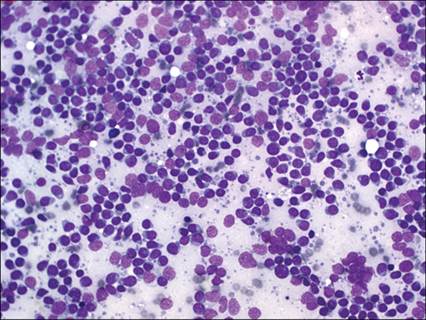
Figure 5.87 Dog, prescapular lymph node, FNA. Homogeneous population composed of small/medium lymphoid cells is found. Some ruptured cells are also seen in the background, suggesting increased fragility. Note the absence of mitotic figures (May–Grünwald–Giemsa, 400? magnification).
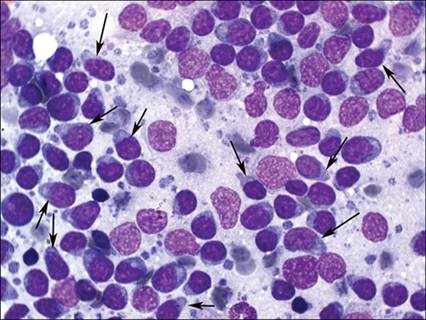
Figure 5.88 Dog, prescapular lymph node, FNA. Many of the cells (arrows) show small, unipolar cytoplasmic tails giving the characteristic hand-mirror shape (May–Grünwald–Giemsa, 1,000? magnification).
Cytologic description
The sample from the prescapular lymph node contains a homogeneous population of small/medium lymphoid cells. Some ruptured cells are also seen in the background, suggesting increased fragility. Note the absence of mitotic figures. At higher magnification, most of the cells show a small, unipolar cytoplasmic tail, giving the characteristic hand-mirror shape.
Cytologic interpretation
Based on the cytologic appearance, a diagnosis of possible low-grade T-cell lymphoma (small clear cell lymphoma) was made. Differentials include paracortical hyperplasia. FNA biopsy was performed and the material collected was put in 1 ml RPMI 1640 medium for flow cytometry. Peripheral blood and a bone marrow aspirate were sampled for staging potentially neoplastic cells. Histologic biopsy via tru-cut was also taken.
Figure 5.89 shows histograms from multicolor flow cytometry of the lymph node aspirate. A prevalent population of medium-sized lymphoid cells scored positive for CD3, CD5, CD21, CD8, and CD4 and negative for CD45. This pattern is considered conclusive of low-grade T-cell lymphoma (T-zone). Peripheral blood was infiltrated by 35% of CD5+CD45− cells.
Neoplastic cells were also found at a high percentage in bone marrow (28%) but, since severe blood contamination was present, it was impossible to define correctly the percentage of infiltration. 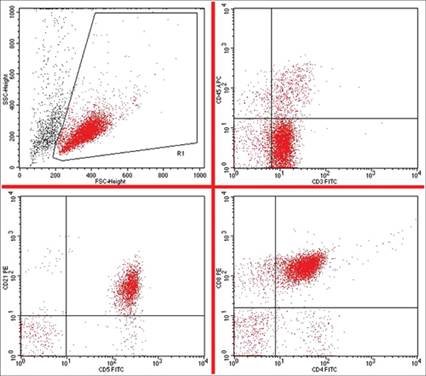
Figure 5.89 Multicolor flow cytometry of the lymph node aspirate. A prevalent population of medium-sized lymphoid cells scored positive for CD3, CD5, CD21, CD8, and CD4 and negative for CD45. This pattern is considered conclusive of low-grade T-cell lymphoma (T-zone). Peripheral blood was infiltrated by 35% of CD5+CD45− cells. Neoplastic cells were also found at a high percentage in bone marrow (28%) but, since severe blood contamination was present, it was impossible to define correctly the percentage infiltration.
Outcome
A final diagnosis of low-grade T-cell (small clear cell) lymphoma, corresponding to T-zone lymphoma in the WHO classification, was made. Histopathology confirmed the T-zone pattern and the dog was treated with chlorambucil and prednisone. Lymphadenomegaly resolved and the dog was alive and in good health 3 months after admission (complete remission).
Discussion
Low-grade T-cell lymphoma is a quite common lymphoma subtype arising from the T-zone. Cytology samples show a classical pattern of small cells with slightly basophilic cytoplasm (small clear cell), low mitotic index, and rare plasma cells. Neoplastic cells often show unipolar cytoplasm (hand-mirror shape). Cytology alone cannot differentiate this lymphoma subtype from paracortical hyperplasia and histology is typically suggested. Recently, a characteristic flow cytometric pattern has been described and this could help to differentiate this subtype on fine needle biopsy (Martini et al., 2015; Seelig et al., 2014). Neoplastic cells showed an aberrant lack of CD45 (pan leukocyte marker), a classical T-cell signature (CD3+CD5+), and aberrant expression of CD21, generally considered a B-cell marker. This aberrant expression has been also demonstrated via gene expression profiling (Frantz et al., 2013).
T-zone lymphoma is generally considered an indolent lymphoma with a long survival (Ponce et al., 2004; Valli et al., 2006) but this may be influenced by staging and clinical condition.CASE 3
Signalment/history
A domestic shorthair, female spayed, 5-year-old cat was presented to clinical visit with depression and occasional regurgitation.
Clinical examination
The cat appeared depressed but alert. A moderate dyspnoea was found. Complete blood cell count (CBC) and clinical biochemistry were unremarkable. Serology for feline leukemia virus (FeLV) and feline immunodeficiency virus (FIV) scored negative. Imaging revealed a huge mass in the cranial mediastinum compressing mainly the left lung. A moderate pleural effusion was also present. Effusion was collected in EDTA and submitted for cytology (Figure 5.90). Fine needle aspiration biopsy was taken and used to prepare some cytologic slides (Figure 5.91) and put in RPMI-1640 medium for flow cytometry (Figure 5.92).
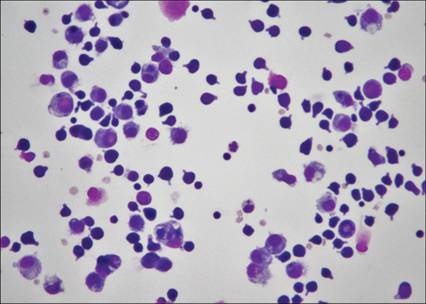
Figure 5.90 Cat, pleural effusion, cytocentrifuged sample. The predominant cells are small to medium-sized lymphocytes (May-Grunwald-Giemsa, 400x magnification).
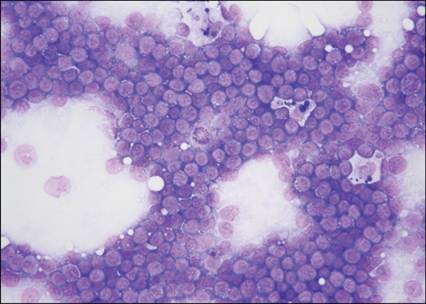
Figure 5.91 Cat, cranial mediastinal mass, FNA. Many medium- lymphocytes and low numbers of phagocytic macrophages are present (May-Grunwald-Giemsa, 400x magnification).
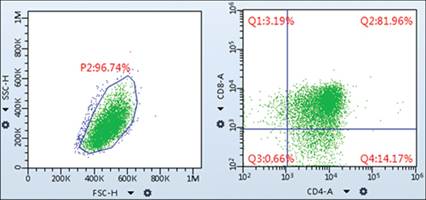
Figure 5.92 Flow cytometric analysis of cells from a cranial mediastinal mass in a cat. Over 80% of the lymphocytes are double positive for CD4 and CD8 (Q2).
Cytologic description
Pleural effusion showed a good cellularity (3,500 wbc/ul) composed by a mixed population of medium/small lymphocytes, sometimes with scarce cytoplasm and fine cytoplastic tails and several macrophages, often in cytophagia. Occasional mitosis, sometimes also atypical, were found in lymphoid cells (Figure 5.91).
Cytology of the mediastinal mass showed a highly cellular sample composed by a prevalent population of medium-sized lymphoid cells, with scarce cytoplasm, round nuclei with decondensed chromatin and often a visible single nucleolus. Mitosis were often visible. Several macrophages, often in phagocytosis of cellular debris, were also visible (Figure 5.91).
Flow cytometry revealed a homogeneous population of T cells composed showing in more than 80% a double positive CD4+CD8+ phenotype (Figure 5.92).
Cytologic and flow cytometric interpretation
Effusion and mediastinal mass revealed a highly prevalent population composed by small to medium lymphocytes showing a double positive CD4+CD8+ T phenotype. This population may be consistent with either neoplastic T lymphomatous cells or normal thymocytes in the context of a non-lymphoid neoplasia. Main differential includes T mediastinal lymphoma and thymoma. Other T cell subpopulations (double negative CD4–CD8– thymocytes, CD4+CD8– T-helper, or CD4–CD8+ T-cytotoxic) were scarce and represent less than 20% of cells.
Outcome
PARR and histopathology were suggested for differential diagnosis. The owners refused further sampling for histology but allowed PARR on the cytological slides already available. Unfortunately, due to the rapid deterioration of symptoms, they elected for euthanasia few days later before receiving the results of PARR analysis. Necropsy was not permitted. PARR analysis revealed a monoclonal rearrangement for T cells consistent with T-cell lymphoma.
Discussion
Lymphoma and thymoma are the main differential for large masses in the mediastinum in cats and dogs. In lymphoma the neoplastic expansion is due to lymphoid component, likely from the thymus or the mediastinal lymph nodes, while in thymoma neoplastic cells often derived from the epithelial component of thymus and lymphoid population represent a non-neoplastic polyclonal component often accompanying some subtypes of the tumor. Finding just a population of small to medium lymphocytes with minimal atypia is not a rare event and cannot differentiate between the two diseases. However, clinical and therapeutic approaches strongly differ between lymphoma (chemotherapy) and thymoma (surgery and eventually radiotherapy). In dogs the majority of mediastinal lymphoma show a clonal expansion of T-helper (CD4+CD8–) or T-cytotoxic (CD4–CD8+) lymphocytes. Occasionally also double negative (CD4–CD8–) or B-cell lymphomas may be found while double positive (CD4+CD8+) lymphomas are quite rare. Flow cytometry using double labeling for CD4/CD8 may assist the differential diagnosis between canine mediastinal lymphoma and thymoma by demonstrating an expansion of one of the above mentioned lymphocyte subsets. According to some studies (Lana et al., 2006b) finding more than 10% of double positive CD4+CD8+ thymocytes is highly supportive of canine thymoma, but this approach is unfortunately useless in cats, since most feline mediastinal lymphomas show a double positive phenotype (Bernardi et al., 2020). PARR and histopathology are mandatory to solve differential in cats, however some cytological and immunophenotypic aspects may help to drive diagnosis of lymphoma vs thymoma:
1. Finding more than 60% lymphoid cells with a phenotype other than double positive CD4+CD8+ is diagnostic of lymphoma.
2. Finding a prevalence of large-sized cells, irrespectively from the phenotype is suggestive of lymphoma.
3. Finding a mixed population of T lymphoid cells with different phenotypes (CD4+,CD8+, CD4+CD8+, and CD4–CD8–) is suggestive of thymoma.
CASE 4
Signalment/history
A 6-year-old, male neutered domestic short-haired cat was evaluated for a history of weight loss and vomiting.
Clinical examination
The cat was bright, alert, and responsive. He was mildly dehydrated but no other abnormalities were detected during physical examination. CBC and clinical chemistry data were unremarkable. He tested negative for feline leukemia and immunodeficiency viruses (FeLV/FIV). An abdominal ultrasound detected a 7 cm ? 5 cm mass in the stomach with loss of gastric wall layering. A FNA biopsy was collected from the mass.
Cytologic description
Most slides contained low to large numbers of lysed nuclei and a large amount of blood. One of the more highly cellular slides contained moderate numbers of intact large lymphocytes (Figure 5.93). The large lymphocytes had a scant to small amount of basophilic cytoplasm and often contained several small, clear, distinct, cytoplasmic vacuoles. The nucleus was eccentrically located and round with stippled chromatin and a large, prominent nucleolus. Nuclei were approximately 20 micrometers in diameter. Low numbers of nondegenerate neutrophils and macrophages were present. Rare small lymphocytes were seen. No gastric epithelial cells were observed.
alt=fig5.93.jpg>
Figure 5.93 FNA from a gastric mass in a 6-year-old, male neutered, domestic short-haired cat. Several ruptured cells are present. The majority of intact cells are large lymphocytes with scant basophilic cytoplasm that contains several small, clear, cytoplasmic vacuoles (Wright–Giemsa, 1,000? magnification).
Cytologic interpretation
The FNA is consistent with lymphoma. Immunophenotyping was recommended. Flow cytometric analysis could have been used for immunophenotyping if a new sample was obtained and placed in media; however the owner was reluctant to place the cat under anesthesia to collect a fresh sample. Immunocytochemistry was not recommended due to the paucity of intact cells in the slides that were evaluated cytologically. Therefore, PARR was performed.
Outcome
PARR results indicated T-cell receptor gene amplification was polyclonal and B cell receptor gene amplification was clonal. Therefore, there was a clonal population of large B cells in the sample, supportive of a diagnosis of large B-cell lymphoma in this cat.
Discussion
The most common gastric tumor in cats is lymphoma (Gualtieri et al., 1999). The majority of cats with gastric lymphoma also have neoplastic lymphocytes in other organs and/or abdominal lymph nodes. Most cats with gastric lymphoma that do not have involvement of other sites are diagnosed with a high-grade, large B-cell lymphoma (Gustafson et al., 2014). In a retrospective study of 16 cats with gastric lymphoma (Gustafson et al., 2014), the median age of diagnosis was 12.8 years. Dehydration and vomiting were the most common clinical signs. The CBC and chemistry data were often unremarkable and cats were negative for FeLV/FIV. The median overall survival time in cats receiving varied forms of chemotherapy was 171 days, whereas cats that did not respond to chemotherapy had an extremely short median survival time (33 days). In contrast, cats with low-grade, small-cell lymphoma involving the gastrointestinal tract typically respond better to chemotherapy and have significantly longer survival times (Lingard et al., 2009).
Large B cells with a distinctive vacuolated morphology are not uncommon to observe in FNAs from cats with lymphoma. Subjectively, this morphology tends to occur in aspirates from affected organs (e.g. renal and gastrointestinal lymphomas) more than aspirates from enlarged lymph nodes.