Cases
CASE 1
Signalment/history
A 9-year-old, spayed female Siamese cat presented for progressive weight loss and diarrhea, with recent onset of anorexia and occasional vomiting.
Physical examination
Thin cat with diffuse muscle atrophy. A large mid-abdominal mass was palpated.
Ultrasound
Loss of the normal definition of the wall layers was present. The intestinal wall was hypoechoic with variable luminal width in the area of the diseased intestine. An ovoid mass was noted at the cranial border of this intestinal mass, which likely represented enlarged lymph nodes involved in the mass. A small amount of peritoneal fluid was also noted at this time.
Cytology
FNA of the mass was performed utilizing a 22-gauge needle attached to a 12 ml syringe. Mild suction was successful in acquiring a diagnostic sample. Wright–Giemsa staining of several slides revealed several aggregates of cohesive-appearing cells (Figures 7.67a, b). Individual cells were ovoid to slightly polygonal in shape. They were often poorly preserved and displayed moderate to marked criteria for malignancy including anisocytosis and increased cytoplasmic basophilia. Many also contained prominent and often multiple nucleoli, and cell borders were occasionally less distinct (Figure 7.67b). Cytoplasmic vacuolation was consistent among the cells, suggesting glandular origin. The cytologic findings were consistent with adenocarcinoma. Similar neoplastic cells were found in an aspirate of an abdominal lymph node, confirming the suspicion of metastasis. Due to a poor prognosis, the cat was humanely euthanized and necropsy was performed.
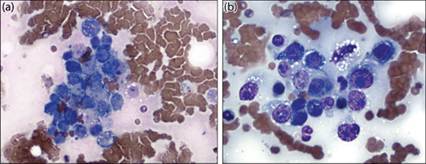
Figures 7.67a,b Intestinal mass from Case 1, feline. (a) Cohesive aggregate of neoplastic cells with moderate to marked criteria for malignancy is present.
(b) Pleomorphism and cell disruption are present among the aggregates (Wright–Giemsa, 500? magnification).
Diagnosis
Intestinal adenocarcinoma.
Necropsy
Gross necropsy revealed the mass to be associated with the mid-intestine (Figures 7.68a, b). Dilatation of the adjacent bowel was found due to annular sclerosis (Figure 7.68c). Metastasis to adjacent structures, including mesentery, omentum, and lymph nodes, was present.

Figures 7.68a–c Intestinal mass from Case 1, feline. (a) Lesion in situ. (b) Mesenteric and lymph node metastases are present. (c) Annular constriction and dilatation are noted on longitudinal sectioning of the intestine. (Courtesy Barry Cooper.)
Histology
Histopathology from the lesion showed invasion of the intestinal wall approaching the serosa. Glandular structures were clearly visible within dense collagenous tissue, confirming the cytologic diagnosis of adenocarcinoma (Figure 7.69).
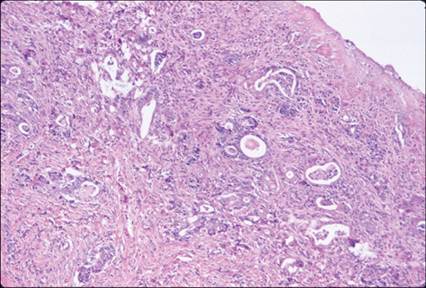
Figure 7.69 Histology of the mass from Case 1, feline. Note the presence of glandular structures (H&E, 40? magnification). (Courtesy Barry Cooper.)
CASE 2
Signalment/history
An 8-year-old, neutered male mixed-breed dog was presented because of recent onset of exercise intolerance and inappetence. Serum biochemistry revealed hypoalbuminemia of 2.1 g/dl (21 g/l) (RI = 2.7–3.9 [27–39]) and an elevated canine-specific pancreatic lipase of >1,000 μg/l (RI = 0–200), prompting an initial, presumptive diagnosis of pancreatitis.
Physical examination
Good body condition and unremarkable findings.
Ultrasound
Mild dilation of the intestines and loss of wall layering were noted. There was also irregular folding of the jejunum at other sites (suggestive of possible irritation). In some regions of the intestine, the adjacent mesentery was hyperechoic.
Cytology
FNA of the irregular region of intestine was attempted utilizing a 22-gauge needle attached to a 12 ml syringe. Wright–Giemsa-stained slides revealed the presence of a mixed lymphoid population, which included several intermediate-sized lymphocytes (Figure 7.70). The cytology was interpreted as consistent with either atypical lymphoid hyperplasia or possible lymphoma. Biopsy of the lesion was recommended.
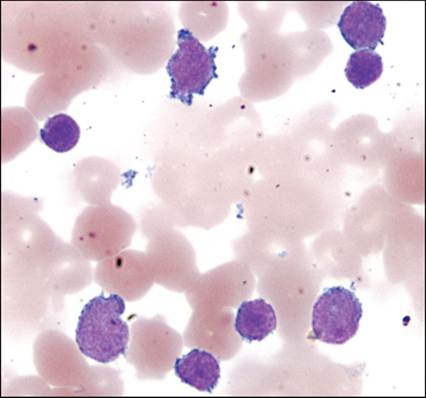
Figure 7.70 Cytology from an aspirate of thickened intestine. Mixed lymphoid cells are present including several intermediate-sized lymphocytes. The sample was interpreted as either lymphoid hyperplasia or lymphoma (Wright–Giemsa, 1,000? magnification).
Surgical findings
An 8 cm section of jejunum containing a circumferential, firm, yellowish 2.5 cm thickened region with omental adhesions was identified and resected (Figures 7.71a, b). Numerous plaque-like and pedunculated additional lesions in the adjacent jejunum, proximal duodenum, and omentum were also present and biopsied. Mildly enlarged mesenteric lymph nodes were appreciated and biopsied. The spleen was also mildly enlarged and therefore resected and submitted for histopathology.
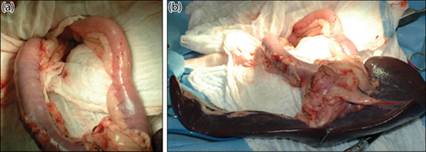
Figures 7.71a,b Intestinal mass and splenomegaly in the dog in Case 2. (a) The small intestine contains multifocal regions of thickening. (b) A larger pedunculated mass of the jejunum is present and adherent to the spleen, which is mildly enlarged.
A peripheral blood sample was obtained at the time of surgery. The dog had a mild anemia and mild leukocytosis due to a left shift neutrophilia. Additionally, a population of atypical intermediate-sized lymphocytes comprising approximately 11% of the nucleated cell population was identified (Figure 7.72). These cells were approximately 50% larger than neutrophils and contained oval, occasionally clefted or scalloped nuclei with smooth chromatin and indistinct nuclei.
They were surrounded by small amounts of basophilic cytoplasm which, on close examination, contained fine eosinophilic granules consistent with granular lymphocytes. 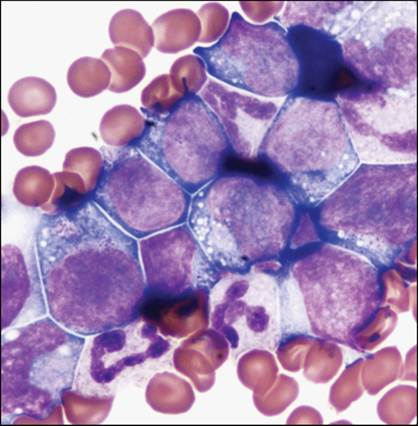
Figure 7.72 Peripheral blood smear from the dog in Case 2. Note the population of intermediate-sized atypical lymphoid cells. Cells typically contain fine eosinophilic granules consistent with granular lymphocytes (Wright–Giemsa, 1,000? magnification).
Diagnosis
Lymphoma – intermediate, granular type.
Histology
Histopathology of the intestine showed diffuse mucosal infiltration by a homogeneous population of small to intermediate-sized lymphocytes with condensed chromatin and a thin rim of indistinct cytoplasm (Figure 7.73). The cells were prominent within the superficial epithelium but not obviously epitheliotropic within the gastric glands. Neoplastic cells infiltrated the submucosa and, to a lesser degree, the muscularis. Mitotic activity was generally low. Similar lymphoid cells were found disrupting and effacing normal splenic and lymph node architecture, confirming visceral spread.
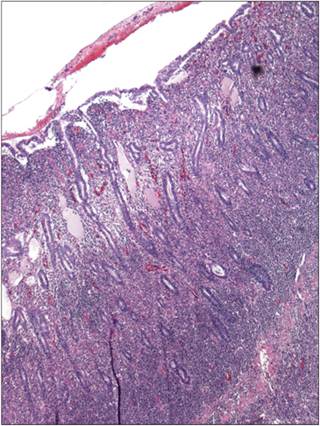
Figure 7.73 Histology of intestine from the dog in Case 2. The normal epithelial architecture is effaced by a population of small to intermediate-sized lymphoid cells. Neoplastic cells infiltrate the submucosa and the muscularis (H&E, 40? magnification).
Based on the cytologic morphology and the likelihood of a T-cell phenotype (likely CD8+, granular form), additional immunostaining for CD3 and CD79 was not pursued.
CASE 3
Signalment/history
A 3-year-old, spayed female Border Collie was presented for evaluation of chronic diarrhea, decreased appetite, and vomiting. Diarrhea was unresponsive to a diet trial, antibiotics, steroids, or probiotics. Defecation was progressively frequent with small volume bouts of liquid stool production upwards of 14 times per day.
Serum biochemistry revealed increased hepatic enzyme and total bilirubin values.Physical examination
Severely thickened and irregular rectal mucosa and painful upon rectal exam. She was febrile (104.6F/40.3C). Generalized, peripheral lymphadenomegaly was also noted.
A rectal scraping was performed during rectal examination and direct smears of the material were made.
Cytology
Frequent mixed inflammatory cells including macrophages, lymphocytes, and occasional neutrophils were identified among a few small aggregates of colonic epithelium. Numerous small, round yeast organisms were identified among the inflammatory cells with frequent phagocytic activity noted by macrophages (Figure 7.74a–c). Erythrocytes and mixed bacteria were present consistent with hemorrhage and fecal material, respectively.
alt=fig7.74.jpg>
Figures 7.74a–c Cytology from a rectal scraping from a dog with chronic small bowel diarrhea and lymphadenopathy (Wright–Giemsa, 1,000? magnification). (a) Macrophages contain small, intracellular yeast-consistent organisms. Several lymphocytes are also identified. (b) Large numbers of small, circular yeast are found among disrupted cells. (c) A small raft of vacuolated colonic epithelial cells is found. Increased cytoplasmic basophilic along with several multinucleated cells are consistent with reactivity secondary to fungal colitis.
Diagnosis
Pyogranulomatous colitis secondary to Histoplasma capsulatum infection.
The patient was euthanized with no additional staging or treatment (case history and images courtesy of Angela Royal).