CASES
CASE 1
Signalment
A 15-year-old neutered male Domestic Shorthair cat was presented for a history of dysorexia, weakness, and weight loss for several weeks.
Physical examination
At physical examination, the cat presented poor body condition and generalized amyotrophy.
The main clinical finding was the presence of a spherical large abdominal mass (diameter: 3–4 cm). No particular abnormality was noticed at the heart and respiratory tract auscultation.Investigation
The complete blood count was characterized by a mild leukocytosis (16.1 109/L, RI: 4.0–15.2 109/L) associated with a moderate neutrophilia (14.3 109/L, RI: 1.7–8.8 109/L), lymphopenia (0.7 109/L, RI: 1.2–10.2 109/L), and monocytosis with the presence of reactive monocytes on the blood smear (1.0 109/L, RI: 0.1–0.6 109/L), consistent with an inflammatory process and possible concurrent corticoid stress.
The biochemistry profile was dominated by a mild decrease in total proteins (51 g/L, RI: 55–71 g/L) with a mild decrease in albumin (22 g/L, RI: 27–39 g/L) which could both be more likely due to malnutrition, cachexia, malabsorption, protein loss enteropathy, and/or an inflammatory process; a mild increase in AST (72 U/L, RI: 6–44 U/L) which could be insignificant or due to hepatocellular or muscle damage; and an abnormal level of fPL with a rapid assay suggestive of a probable context of pancreatitis (IDEXX SNAP fPL Test). Electrolytes, ALP, ALT, GGT, and total bilirubin were within the reference interval, and no abnormality was noticed for the urinalysis.
A medical imaging investigation was performed to investigate a possible context of pancreatitis: the abdominal ultrasound revealed a pancreatic enlargement associated with strong and diffuse hypoechogenicity (Figure 8.42).
The surrounding mesenteric fat was hyperechoic, and free fluid was noted around the pancreas. These findings were consistent with acute pancreatic inflammation or diffuse neoplasia. Thoracic radiography revealed a slight thoracic effusion. 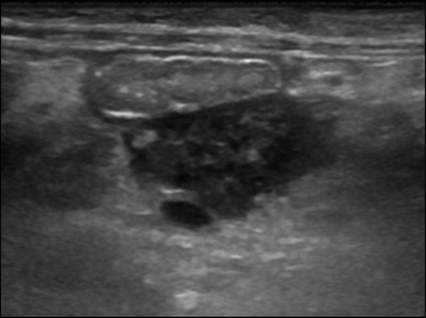
Figure 8.42 Ultrasonography of the pancreas. Pancreatic enlargement associated with diffuse hypoechogenicity and a distinct margin. The duodenum is seen in the near field, and the mesenteric fat appears hyperechoic.
Fine needle aspirates of the pancreas and the abdominal effusion were performed, and slides were stained with a modified May–Grünwald–Giemsa staining. Cytological evaluation of the pancreas revealed a mixed inflammation associated with secondary hyperplasia of acinar pancreatic cells, and at least a marked infiltration by an abnormal and monomorphic population of blastic cells (Figure 8.43). These blastic cells were large in size and presented a high nuclear to cytoplasmic ratio, a deeply basophilic cytoplasm sometimes finely and discretely vacuolated and/or disclosing a pseudo-arcoplasm, and a round and less frequently irregular nucleus associated with a finely reticulated chromatin pattern (Figures 8.43). One or numerous small to large nucleoli, sometimes prominent, were also observed. All these cytological features were consistent with an infiltration by blastic lymphoid cells, and the cytological diagnosis was a high-grade lymphoma. The nucleated cell count of the peritoneal fluid was 4,760 cells/µL and the protein concentration was 16 g/L. The cytological evaluation of the abdominal effusion was characterized by 87% of atypical blastic lymphoid cells, 9% neutrophils, 3% lymphocytes, and 1% macrophages (Figures 8.44 and 8.45). Immunocytochemistry was performed on the abdominal effusion to phenotype the neoplastic cells. The neoplastic population was strongly reactive for BLA36 and negative for CD3, CD79a, and a pancytokeratine (Figures 8.46a, 8.46b and 8.46c).
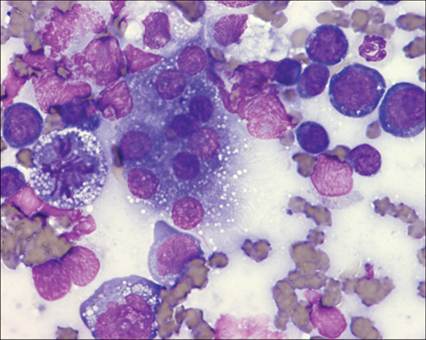
Figure 8.43 Cytology of the pancreas. Mixed inflammation characterized by macrophages and neutrophils and associated with a hyperplasia of acinar pancreatic cells characterized by the presence of a medium to large nucleoli, a moderate anisokaryosis and anisocytosis, and some binucleation of the acinar cells, and the presence of an abnormal population of blastic cells. May–Grünwald–Giemsa (?1,000).
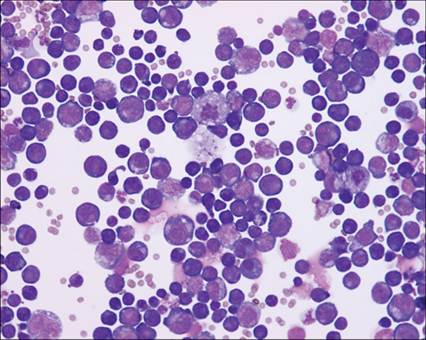
Figure 8.44 Cytology of the abdominal effusion. Presence of numerous and predominant monomorphic blastic cells cytologically similar to the neoplastic cells observed in the pancreas. May–Grünwald–Giemsa (?400).
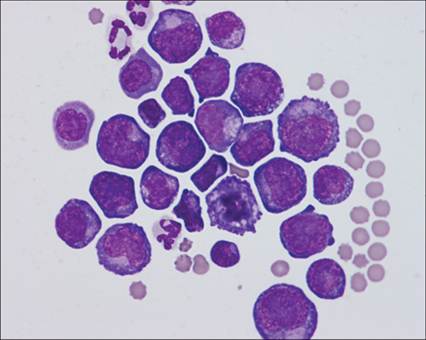
Figure 8.45 Cytology of the abdominal effusion. Presence of predominant round blastic cells consistent with the neoplastic cells observed in the pancreas. These cells are large in size and have a high nucleo-cytoplasmic ratio, a deeply basophilic cytoplasm sometimes disclosing a pseudo-arcoplasm, and a round to irregular nucleus associated with a finely reticulated chromatin pattern with one or numerous small to large nucleoli. May–Grünwald–Giemsa (?1,000).
Based on all of these clinico-pathological findings, a final diagnosis of a B-cell high-grade lymphoma involving the pancreas was made, associated with secondary pancreatitis, even if a histiocytic neoplasm could not be excluded. The pancreatic origin of this lymphoma was suspected since no other solid organ seemed to be involved on medical imaging, but it could not be confirmed as the cat was discharged, and no outcome was available.
This clinical case stresses the fact that cytology is useful and safe to make the distinction between a pure inflammatory process such as pancreatitis and a diffuse neoplastic pancreatic infiltration such as high-grade lymphoma.
CASE 2
Signalment
A 10-year-old neutered female mixed breed dog was presented for a history of weakness, shivering for 3 days, and vomiting and diarrhea for 12 hours after dietary indiscretion. Two years ago, the dog was presented for acute blindness diagnosed as sudden acquired retinal degeneration associated with idiopathic hypertriglyceridemia.
Physical examination
At physical examination, the dog presented good body condition and abdominal distension. The main clinical finding was abdominal pain elicited by abdominal palpation. No particular abnormality was noticed at the heart and respiratory tract auscultation, but mild tachypnea was observed.
Investigation
The complete blood count was characterized by a mild neutrophilia (12.3 109/L, RI: 1.7–8.8 109/L) with a left shift and the presence of reactive monocytes and toxic neutrophils on the blood smear, consistent with an inflammatory process.
The biochemistry profile was dominated by a mild increase in total proteins (71.6 g/L, RI: 48–66 g/L), which could be due to dehydration or an inflammatory process; a mild increase in ALT (80 U/L, RI: 3–50 U/L) and ALP (331 U/L, RI: 22–155 U/L), which could be insignificant or due to hepatocellular damage and cholestasis; an abnormal level of cPL with a rapid assay suggestive of pancreatitis (IDEXX SNAP cPL Test); and an increase in creatinine, which could be suggestive of renal failure. Albumin and total bilirubin were within the reference range. The urinalysis was characterized by a low normal urinary specific gravity (1.024, RI: 1.015–1.050).
A medical imaging investigation was performed to investigate a possible context of hepatic, renal diseases, and pancreatitis: the abdominal ultrasound revealed a pancreatic enlargement associated with strong and diffuse hypoechogenicity. The surrounding mesenteric fat was hyperechoic. These findings were consistent with acute pancreatic inflammation. The abdominal ultrasound also revealed a homogeneous enlarged liver and hyperechoic kidneys suggestive of diffuse vacuolar hepatopathy in the context of idiopathic hypertriglyceridemia and chronic renal failure, respectively.
Fine needle aspirates of the pancreas were performed, and slides were stained with a modified May–Grünwald–Giemsa staining. Cytological evaluation of the pancreas revealed a neutrophilic inflammation associated with a severe hyperplasia of acinar pancreatic cells (Figure 8.47). Neutrophils were sometimes degenerated and a few spumous macrophages were also observed. Based on all of these clinico-pathological findings, a final diagnosis of acute pancreatitis was made. After 3 days of supportive care, the dog improved and was discharged. The follow-up performed 1 month later showed an alert dog with stability of the chronic renal disease.

Figure –c 8.46a Immunocytochemistry of the abdominal effusion. The neoplastic cells are strongly positive with BLA36 (a) and negative for CD3 (b) and pancytokeratin (c) and are consistent with a B-cell high-grade lymphoma even if a histiocytic neoplasm could not be excluded (?1,000).
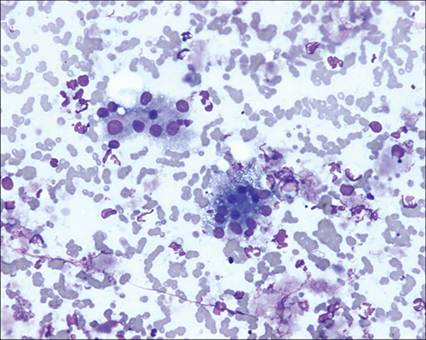
Figure 8.47 Cytology of the pancreas. Neutrophilic inflammation characterized by neutrophils associated with a hyperplasia of acinar pancreatic cells characterized by the presence of anisokaryosis and anisocytosis of the acinar cells. May–Grünwald–Giemsa (?400).
CASE 3
Signalment/history
A 5-year-old, female, Jack Russell dog was presented for a history of acute vomiting, diarrhea, and hematochezia. One month ago, the dog presented an event of acute vomiting and diarrhea simply resolved with symptomatic treatment.
Physical examination
The dog was presented in moderate body condition. The main clinical findings were marked icterus, a left apexial systolic murmur of grade I/V, and abdominal pain elicited by abdominal palpation.
Investigation
The complete blood cell count was characterized by a moderate leucocytosis (22.51.109/L; RI: 5.05–16.76) related to a neutrophilia (18.4.109/L; RI: 2.95–11.64), a monocytosis (1.32.109/L; RI: 0.16–1.23), and an eosinophilia (1.60.109/L; RI: 0.06–1.23).
The biochemistry profile was dominated by a severe increase in ALT (4062 U/L; RI: 8–60), AST (>1083 U/L; RI: 0–50), ALP (19329 U/L; RI: 30–230), and GGT (97 U/L; RI: 0–11) activities, and a marked increase in total bilirubin (38.5 mg/L; RI: 0.0–9.0), which were suggestive of hepatocellular damage and cholestasis. Urea, creatinine, glucose, and a panel of electrolytes were within reference intervals. Urinalysis was characterized by a low normal urinary specific gravity (1.015; RI: 1.015–1.050), pH equal to 8, and significant bilirubinuria (« +++ ») and possible proteinuria (« ++ ») according to dipstick analysis. Proteinuria had not been confirmed by a urinary protein to creatinine ratio.
An abdominal ultrasound mainly revealed a dilatation of the gallbladder, choledocal channel, and the rest of the biliary tract associated with the presence of a stone, many changes in the right lobe of the pancreas associated with a mass in relation to the duodenal papilla, and then a moderate pancreatic adenopathy. These findings were consistent with post-hepatic cholestasis and a possible neoplasia of the pancreas probably extended to the nearby lymph node.
A laparotomy was performed to explore the biliary tract and pancreatic anomalies, and to try to investigate more accurately the pancreatic mass. It confirmed all previously noticed changes in the biliary tract and the presence of an infiltrating and diffuse mass (size: 2 ? 1 ? 1 cm), in the area of the duodenal papilla but for which the origin was finally macroscopically uncertain, pancreatic, or duodenal. Surgical removal of this mass was impossible, and so FNA and biopsy of the mass and a biopsy of the enlarged pancreatic lymph node were performed to make a diagnosis.
Cytologic evaluation
There was a hemorrhagic, markedly necrotic, and slightly inflammatory background (Figure 8.48). The cellularity was high and the cells of interest were fragile; many naked nuclei (sometimes atypical) were also observed (Figure 8.49). The sample mainly revealed an abundant and predominant population of atypical cohesive cells, which were organized in many clusters with tubular, papillary, and acinar patterns (Figures 8.50 and 8.51). These epithelial cells were of medium-large size to giant, often associated with a moderate to high N:C ratio. Their cytoplasm was mainly polarized, granular (pale pink round granules suggestive of zymogen granules), and hyperbasophilic and so suggestive of acinar pancreatic cells, and their nucleus was round to oval, often polarized, and with a coarse to reticular chromatin pattern and one or two small to large nucleoli (Figures 8.51 and 8.52). These cells were also occasionally microvacuolated. Anaplastic features were frequently observed: marked anisocytosis and anisokaryosis, binucleation, macronucleolation, giant cells, and some mitotic figures (Figures 8.52 and 8.53). All these cytological features were highly suggestive of pancreatic adenocarcinoma. The histopathological examination of the mass and the enlarged lymph node confirmed a pancreatic adenocarcinoma with extension to the pancreatic lymph node (Figures 8.54 and 8.55). The same neoplastic tissue compatible with a pancreatic carcinoma was also observed replacing the lymphoid pulp in the nodal biopsy.
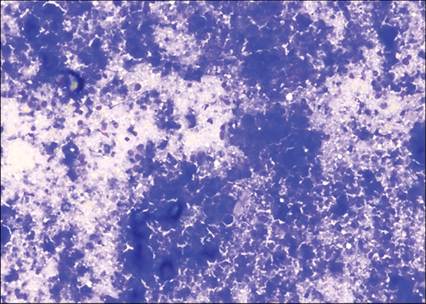
Figure 8.48 Cytology of pancreas. Necrotic background mainly associated with coagulation necrosis, damaged cells in cohesive clusters, and some calcified debris appearing as three-dimensional refractile material (May–Grünwald–Giemsa, 200? magnification).
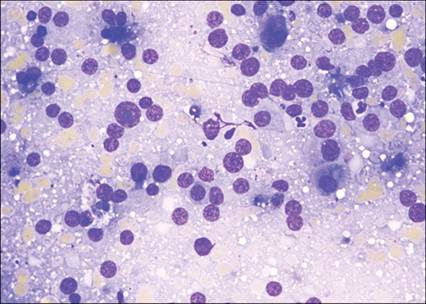
Figure 8.49 Cytology of pancreas. Hemorrhagic and necrotic background with many naked nuclei. Naked nuclei showed sometimes atypical features: gigantism, macronucleoli, and multiple nucleoli (May–Grünwald–Giemsa, 500? magnification).
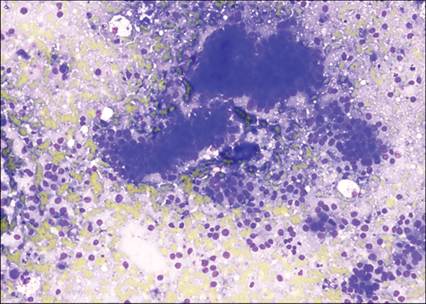
Figure 8.50 Cytology of pancreas. Abundant population of cohesive cells mainly organized in clusters with tubular, papillary, and acinar patterns. The epithelial cells were medium to large size, and round to polygonal, with a medium to high N:C ratio (May–Grünwald–Giemsa, 200? magnification).
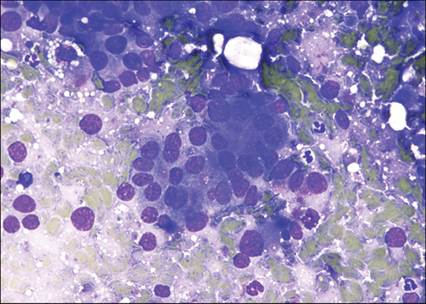
Figure 8.51 Cytology of pancreas. Epithelial cells of interest organized in clusters with acinar patterns. These cells were medium to large size, with a round to polygonal shape, and with a clearly polarized nucleus, and displayed a medium to high N:C ratio. Their cytoplasm was granular (pink round granules suggestive of zymogen granules) and hyperbasophilic and so suggestive of acinar pancreatic cells, and their nucleus was round to oval, and with a coarse to reticular chromatin pattern and one or two small to large nucleoli (May–Grünwald–Giemsa, 500? magnification).
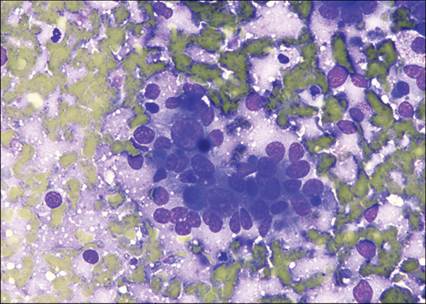
Figure 8.52 Cytology of pancreas. Acinar pancreatic cells organized in clusters with acinar patterns. These cells were medium to very large in size, with a round to polygonal shape, and with a polarized nucleus, and displayed a medium to high N:C ratio. Their cytoplasm was moderately granular and hyperbasophilic. Their nucleus was round to oval, and with a coarse to reticular chromatin pattern and one or two small to giant nucleoli. The cells showed marked atypical features: marked anisokaryosis and anisocytosis, and macronucleolation (May–Grünwald–Giemsa, 500? magnification).
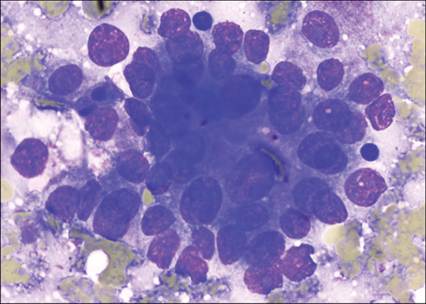
Figure 8.53 Cytology of pancreas. Acinar pancreatic cells organized in clusters with acinar patterns. These cells were medium to very large in size, with a round to polygonal shape, and with a polarized nucleus, and displayed a medium to high N:C ratio. Their cytoplasm was granular (pink granules) and hyperbasophilic. Their nucleus was round to oval, and with a coarse to reticular chromatin pattern and one or two small to large nucleoli. The cells showed marked atypical features: marked anisokaryosis and anisocytosis, some binucleation and macronucleolation (May–Grünwald–Giemsa, 1,000? magnification).
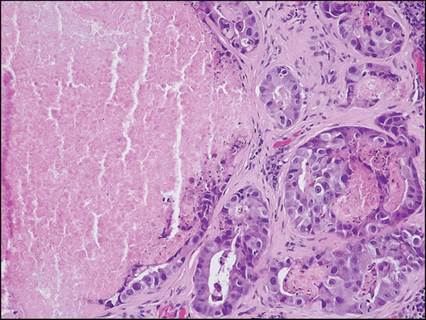
Figure 8.54 Biopsy of pancreas. The pancreatic mass consisted of anastomosed tubulo-acinar structures with variable distended lumens, supported by an abundant fibrous stroma, infiltrated by some lymphocytes, plasma cells, and neutrophils. An eosinophilic, granular necrotic material was frequently observed within neoplastic distended lumens. Tubules and acini were lined by a cuboidal to pyramidal, unicellular to multifocally stratified, severely atypical, neoplastic epithelium (Hemalun–Eosin, 200? magnification).
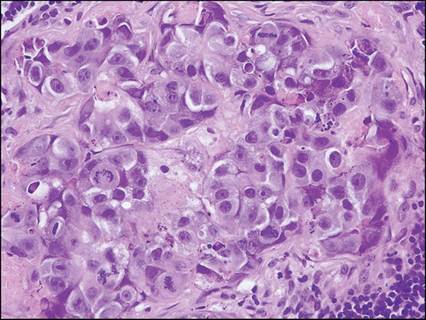
Figure 8.55 Biopsy of pancreas. Neoplastic cells, arranged in tubules or acini with a small central lumen containing necrotic hypereosinophilic debris, were large, cuboid to pyramidal, with a parabasal to basal nucleus and an abundant finely granular to rarely microvacuolated, amphophilic cytoplasm. Nuclei were round to oval, with a variably condensed chromatin, one large to several small basophilic nucleoli. Anisocytosis and anisokaryosis were marked to severe, and mitoses were numerous, and often atypical (Hemalun–Eosin, 400? magnification).
Diagnosis
Based on clinico- and histopathologic findings, a final diagnosis of pancreatic adenocarcinoma disseminated at least to the pancreatico-duodenal lymph node was made.
Outcome
Given the poor prognosis, a symptomatic and palliative treatment was decided by the owners. The dog was finally humanely euthanized 2 months later.