Pancreatic tumors
Exocrine pancreatic tumors
Exocrine pancreatic adenoma
Definition and prevalence
Adenoma is a rare, incidental lesion, and less frequent than its malignant counterpart (Meuten, 2002; Head, 2003; Charles, 2007).
No evidence of a transformation of a pancreatic hyperplasia through adenoma into adenocarcinoma has been demonstrated (Meuten, 2002). Distinction between pancreatic exocrine adenoma and nodular hyperplasia may be difficult, and is poorly defined in domestic animals (Zachary & McGavin, 2013).Gross anatomy
Grossly, adenomas are solitary, small (rarely more than 5 mm in diameter), beige to fawn, compressive lesions (Meuten, 2002; Head, 2003; Charles, 2007).
Histopathology
Histologically, adenomas are masses which are expansive and compressive, tubular (of ductal origin) or acinar (of acinar cell origin) structures supported by a thin collagenous stroma surrounded by a thin capsule. Cells are cuboidal to columnar, with a variable cytoplasmic content of zymogen granules, and have a regular and round nucleus. Mitoses are rare (Meuten, 2002; Head, 2003; Charles, 2007). Metastasis does not occur, but local compressive growth patterns can result in atrophy of adjacent acini (Meuten, 2002).
Cytology
A cytological diagnosis of pancreatic adenoma is very difficult, since normal and hyperplastic pancreatic tissues are cytologically very similar (Meuten, 2002). The cytologic appearance can also be similar to some well-differentiated adenocarcinomas (Allen, 2021). Cytologic findings should be interpreted along with the ultrasonographic findings (Bjorneby & Kari, 2002). Cytological samples of a pancreatic adenoma are mainly associated with the presence of uniform and non-atypical acinar cells arranged in clusters, which can occasionally display mild anisocytosis and an increase in cytoplasmic basophilia (Bjorneby & Kari, 2002).
Exocrine pancreatic carcinoma
Definition and prevalence
Exocrine pancreatic carcinoma is the most common tumor of the exocrine pancreas (Meuten, 2002), but it remains an uncommon lesion in all species (Priester, 1974; Meuten, 2002; Charles, 2007; Zachary & McGavin, 2013). The incidence of pancreatic adenocarcinoma increases with age of animals, but it has been described in a 3-year-old dog (Priester, 1974). No sex predisposition has been described in cats; this is probably similar in dogs but needs to be confirmed because of some contradictory studies (Priester, 1974; Head, 2003; Pinard et al., 2021). No clear breed predilection has been reported. Airedale terriers may be at higher risk according to one study, but this observation was not confirmed in a more recent study on a series of 23 dogs with exocrine pancreatic carcinoma (Priester, 1974; Pinard et al., 2021). Comorbidities (e.g., diabetes mellitus) are frequent in cats, but they are not so obvious in dogs (Pinard et al., 2021).
Gross anatomy
Carcinomas may consist of a single and discrete or more often multiple, irregular, gray to yellow nodules of variable size with a firm-to-hard consistency. The neoplastic mass can be diffuse or localized in the midportion of the pancreas in dogs, whereas the neoplastic lesion is associated with a more diffuse pattern in cats (Meuten, 2002; Pinard et al., 2021). Lesions with a diffuse pattern lead to consideration of chronic pancreatitis or nodular hyperplasia in the list of differential diagnoses. The cut surface of the tumor is frequently heterogeneous with areas of softening and necrosis, mineralization, or hemorrhage. Invasion of adjacent tissues (e.g., common bile duct and duodenum) and serosal seeding with multiple transcoelomic metastases are common. The most frequent sites of metastasis are mesentery, peritoneum, adjacent gastrointestinal tract, liver, local lymph nodes, and lung, and less frequently spleen, kidney, diaphragm, and skin (Meuten, 2002; Charles, 2007).
Fat necrosis of adjacent omentum or mesentery and adhesions between the pancreas and adjacent tissues are frequently observed (Meuten, 2002; Head, 2003; Charles, 2007; Zachary & McGavin, 2013).Histopathology
Microscopic features of pancreatic carcinoma range from well-differentiated adenocarcinomas, with tubular or acinar patterns (Figure 8.28), to undifferentiated solid carcinomas. In the tubular pattern, glandular structures can be formed by cuboidal or columnar cells, presumed to originate from ducts, with occasional mucus secretion. Persistence of eosinophilic zymogen granules is only observed in well-differentiated tumors (Figure 8.29). Atypia and mitotic index are often correlated to the level of differentiation, with uniformity, regular cellular polarity, low nuclear to cytoplasmic ratio, and a low number of mitoses in well-differentiated carcinomas; and indistinct cellular borders with a high nuclear to cytoplasmic ratio, anisocytosis, anisokaryosis, and a higher number of mitoses in poorly differentiated carcinomas. The amount of supporting stroma is variable, usually greatest and scirrhous in poorly differentiated tumors. Metastatic behavior cannot be predicted by histological morphology as well-differentiated carcinomas can metastasize widely (Meuten, 2002; Head, 2003; Charles, 2007; Zachary & McGavin, 2013).
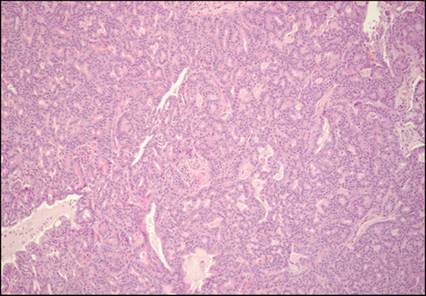
Figure 8.28 Histopathology of a pancreatic exocrine well-differentiated adenocarcinoma from a cat. Neoplastic tissue consists of relatively uniform small acinar to tubular structures with some larger ones, which appear more dilated with an eosinophilic luminal material admixed with cellular debris. Supporting stroma is sparse in this case but can be dense and desmoplastic in poorly differentiated carcinoma. Hematoxylin and eosin (?100).
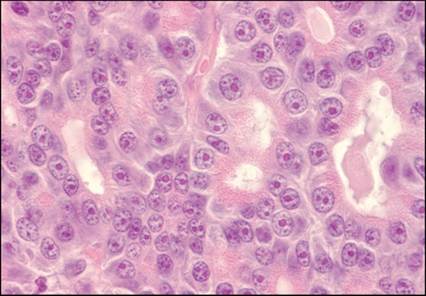
Figure 8.29 Histopathology of a pancreatic exocrine well-differentiated adenocarcinoma from a cat.
Higher magnification from Figure 8.28. Neoplastic cells are cuboidal, forming acini or tubules with a small lumen. Nuclei are uniform, round to oval, with sparse chromatin and bright eosinophilic nucleoli, and are still located basally. Eosinophilic small zymogen granules are recognizable in the apical region of the cytoplasm. Despite the relative uniformity of neoplastic cells, atypical cells are noticed with anisocytosis, anisokaryosis, and multiple nucleoli. Hematoxylin and eosin (?1,000).
Ultrasound
Pancreatic adenocarcinomas are described as hypoechoic nodules or masses with a tendency to develop in the central portion of the gland and invade the adjacent structures and organs (Figures 8.30a and 8.30b) (Penninck and d'Anjou, 2013). Pancreatic enlargement, abdominal effusion, and extra-hepatic biliary obstruction are also common findings with pancreatic adenocarcinomas (Hecht & Henry, 2007). Therefore, it remains challenging to differentiate pancreatic adenocarcinomas from pancreatitis or nodular hyperplasia solely on the basis of the ultrasound findings (Griffin, 2020).
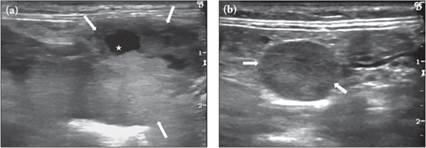
Figures 8.30a,b Sagittal view of the right pancreatic lobe of a 13-year-old cat with pancreatic adenocarcinoma. A voluminous mass (white arrows) is adjacent to the descending duodenum in an overall enlarged hypoechoic and heterogeneous pancreas. Cyst-like lesions (white star) are noted in the pancreatic parenchyma identified as necrotic centers. Enlarged mesenteric lymph node (white arrows) in the same cat.
Cytology
Fine needle aspirates can be useful in the diagnosis of exocrine pancreatic carcinoma (Bennett et al., 2001). It has been reported as a safe procedure even if one suspected case of needle tract seeding has been reported in a cat (Jegatheeson et al., 2020) In human medicine, different studies have investigated the diagnostic performance of pancreatic tissue FNA in cases of well-differentiated pancreatic adenocarcinoma.
These studies have established many cytological criteria such as anisonucleosis, nuclear enlargement, nuclear crowding and overlapping, and nuclear membrane irregularity, in order to optimize the diagnostic performance of the cytology when compared to histology (with 98% sensitivity and 100% specificity) (Lin et al., 2003). Other cytological criteria such as necrosis, hyperchromasia, macronucleoli, chromatin clearing, and mitosis were of more limited diagnostic significance according to this study (Lin & Staerkel, 2003). Unfortunately, no similar study has yet been performed in veterinary medicine. In general, the cytological diagnosis of exocrine pancreatic neoplasia is easier in cases of poorly differentiated neoplasms because of the presence of many anaplastic features. If the pancreatic adenocarcinoma is very well-differentiated and/or associated with an inflammatory context, the cytological diagnosis can be difficult and histopathology is needed to make a definitive diagnosis and to exclude a nodular hyperplasia, adenoma, or a reactive hyperplasia secondary to an inflammatory background (Figures 8.31–8.33) (Jegatheeson et al., 2020). Furthermore, the yield of cytological sample can be dependent on the size and the degree of fibrosis of the neoplastic mass (Bjorneby & Kari, 2002).The background of a pancreatic adenocarcinoma cytological sample is not specific and can be inflammatory, hemorrhagic, and/or necrotic (Borjesson, 2014). The cellularity is commonly high, and the cytological samples reveal many clusters of pancreatic cells organized in an acinar and/or tubular pattern, which can loose their polarity (Figure 8.31) (Bjorneby & Kari, 2002). The cells are often associated with an increased (N:C) ratio, and their cytoplasm can be hyperbasophilic, display vacuolization (also observed in pancreatitis), and be more or less granular according to the degree of differentiation of the tumor (pale pink round granules corresponding to zymogen granules) (Figure 8.32) (Bjorneby & Kari, 2002; Borjesson, 2014).
The nucleus is often enlarged with a coarse or reticular chromatin pattern and often contains one or multiple more or less prominent nucleoli (Figure 8.33) (Bjorneby & Kari, 2002; Borjesson, 2014). Nuclear molding and irregularities can also be visualized (Borjesson, 2014). Finally, the anaplastic features are variable. Moderate to marked anisokaryosis can be observed, but other anaplastic features are possible, especially in cases of poorly differentiated neoplasms (Figures 8.34 and 8.35). Immunocytochemistry and other diagnostic testing may be necessary to differentiate poorly differentiated exocrine pancreatic adenocarcinoma and other neoplasms such as endocrine pancreatic tumor or secondary metastatic carcinoma. 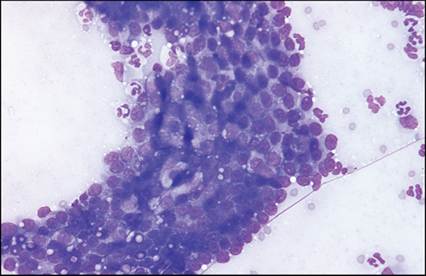
Figure 8.31 Aspirate of a well-differentiated pancreatic adenocarcinoma from a cat (same case as in Figures 8.28 and 8.29). Presence of a large pseudo-tubular structure composed of neoplastic pancreatic cells associated with an inflammatory background. The pancreatic cells are medium-sized with an increased nuclear to cytoplasmic ratio and a cuboidal shape; their cytoplasm is sometimes vacuolated (small clear and discrete vacuoles). Anisokaryosis is mild. May–Grünwald–Giemsa (?400).
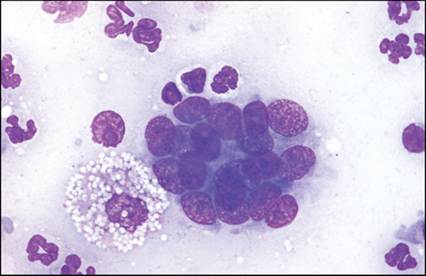
Figure 8.32 Aspirate of a well-differentiated pancreatic adenocarcinoma from a cat (same case as in Figures 8.28 and 8.29). Higher magnification from Figure 8.31. Inflammatory background composed of many neutrophils and a few foamy macrophages associated with the presence of a small acinar structure composed of acinar pancreatic neoplastic cells. The neoplastic cells are medium-sized and are characterized by a polygonal to cuboidal shape associated with a high nuclear to cytoplasmic ratio. The cytoplasm of these cells is basophilic and slightly granular, and the nuclei are round to ovoid and associated with a reticular to coarse chromatin pattern and one small to medium and round to angular nucleolus. Anisokaryosis is mild to moderate, and nuclei are overlapped. The presence of the inflammatory background can make the cytological diagnosis of exocrine pancreatic adenocarcinoma difficult in this case. May–Grünwald–Giemsa (?1,000).
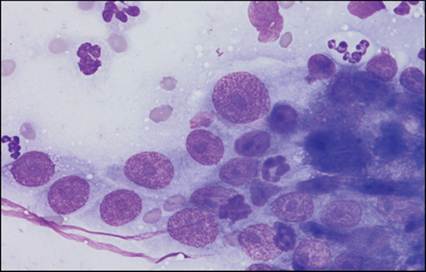
Figure 8.33 Aspirate of a well-differentiated pancreatic adenocarcinoma from a cat (same case as in Figures 8.28 and 8.29). Higher magnification from Figure 8.31 and 8.32. Inflammatory background composed of many neutrophils associated with the presence of some atypical and loosely cohesive acinar pancreatic cells. The neoplastic cells are medium- to large-sized and are characterized by a polygonal to cuboidal shape associated with a high nuclear to cytoplasmic ratio. The cytoplasm of these cells is slightly basophilic and poorly granular, and the nuclei are round to ovoid and associated with a reticular to coarse chromatin pattern and one medium to large and prominent nucleolus. Anisokaryosis and anisocytosis are marked. These more atypical pancreatic cells facilitate the cytological diagnosis of adenocarcinoma in this case associated with a marked inflammatory context. May–Grünwald–Giemsa (?1,000).
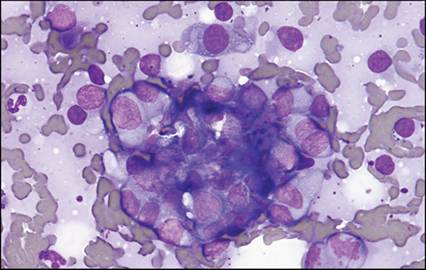
Figure 8.34 Aspirate of an anaplastic pancreatic adenocarcinoma from a cat. Bloody background associated with some naked nuclei, some inflammatory cells consisting of neutrophils and fewer lymphocytes, macrophages and mast cells, and some solid clusters of medium to large atypical and anaplastic acinar pancreatic cells organized in a pseudo-acinar pattern. These atypical cells are characterized by a round, cuboidal to polygonal shape and a high to medium nuclear to cytoplasmic ratio and disclose some criteria of malignancy, with a marked anisokaryosis, some binucleations, and an abnormal mitotic figure. May–Grünwald–Giemsa (?400).
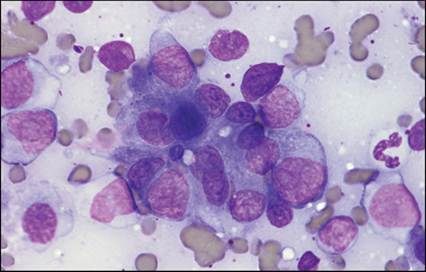
Figure 8.35 Aspirate of an anaplastic pancreatic adenocarcinoma from a cat. Higher magnification from Figure 8.34. Bloody background associated with a large acinar structure composed of very atypical and poorly differentiated acinar pancreatic cells. The neoplastic cells are medium- to large-sized and are characterized by a round to cuboidal outline with clear to indistinct cell borders, a high to medium nuclear to cytoplasmic ratio, and a basophilic and slightly granular cytoplasm. The nuclei are round to ovoid, and associated with a finely stippled to lacy chromatin pattern and the presence of one or numerous small to large, and sometimes prominent, nucleoli. May–Grünwald–Giemsa (?1,000).
Endocrine pancreatic tumors
Definition and prevalence
Pancreatic islet cell tumors are rare in domestic animals (Charles, 2007). The neoplasms most frequently related in pancreatic islets are those derived from β islet cells, named insulinoma. They are often endocrinologically active, resulting in hyperinsulinism and related hypoglycemia, regardless of the neoplasm malignancy (Charles, 2007). Non-β islet cell neoplasms, mainly secreting gastrin, glucagon, somatostatin, or pancreatic polypeptide (Meuten, 2002; Charles, 2007; Cruz Cardona et al., 2010), have been reported very infrequently in dogs and cats. The macroscopic pathology as well as histopathology of these different tumors is quite similar, characteristic of an endocrine origin. Only immunohistochemistry permits the differentiation of the exact cellular lineage by identifying the hormone synthesized, even if one or more pancreatic hormones can be secreted by the tumor (Minkus et al., 1997; Meuten, 2002; Head, 2003; Charles, 2007; Zachary & McGavin, 2013). Multihormonality of a tumor is not correlated with its biological behavior. The median reported age is 9 to 10 years for canine insulinoma. Medium to large breed are overrepresented, and no sex predilection has been reported (Minkus et al., 1997; Bailey, 2007; Goutal et al., 2012). Insulinoma is less commonly described in cats, but the prevalence also increases in older cats (Bailey, 2007). Siamese may be overrepresented, but the few reported cases in cats do not allow us to establish a breed predilection (Bailey, 2007).
Islet cell adenomas (benign insulinoma) and carcinomas (malignant insulinoma) are both encountered in domestic animals, with malignant tumors being more frequent than benign ones (Head, 2003; Charles, 2007; Zachary & McGavin, 2013). The behavior and metastatic potential of insulinoma cannot generally be reliably foretold by histological and particularly cytological features, since anaplastic features are frequently mild and inconsistent (Bjorneby & Kari, 2002; Andreasen et al., 2010). Metastases are frequent, involving especially regional lymph nodes and the liver, and are reported in approximately half of cases of canine insulinoma (Caywood et al., 1979; Bailey, 2007; Madarame et al., 2009).
Gross anatomy and histopathology
Table 8.2 summarizes similarities and differences between islet cell adenomas and carcinomas (Charles, 2007) (Meuten, 2002; Head, 2003; Zachary & McGavin, 2013).
Table 8.2 Gross morphology and histopathology characteristics of islet cell neoplasia
| Islet cell adenoma | Islet cell carcinoma | ||
| Gross morphology | Similarities | Usually single but sometimes multiple, sharply demarcated from surrounding tissues, firm, yellow-gray to purple nodular tumors | |
| Differences | Small (1 to 3 cm in diameter), spherical, and homogeneous nodules | Larger than adenomas Multilobular appearance +/– extensive invasion into adjacent parenchyma Necrosis and hemorrhage Metastasis in lymph nodes, liver, omentum, and mesentery | |
| Histopathology | Similarities | Cords, nests, trabeculae, pseudoacinar pattern Delicate fibrovascular stroma with numerous small capillaries Cells are cuboidal to polyhedral, or columnar, with an abundant, finely granular, pale eosinophilic cytoplasm Mitoses infrequent | |
| Differences | Thin fibrous capsule Irregularly shaped ducts and small nests of exocrine pancreatic acinar cells, particularly towards the periphery | Infiltration through the capsule and into adjacent parenchyma by neoplastic cells = the most important feature of malignancy Cells are less uniform in size and shape (anisocytosis, anisokaryosis) | |
| (1–4) | |||
| 1. Charles JA. Pancreas. In: M.; GM, editor. Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, Fifth edition. Philadelphia: Elsevier Saunders; 2007. | |||
| 2. Zachary JF, McGavin D. Pathologic Basis of Veterinary Disease: Elsevier Health Sciences; 2013. | |||
| 3. Meuten DJ. Tumors in domestic animals. Ames, IA: Iowa State Press; 2002. | |||
| 4. Head KW. Histological classification of tumors of the alimentary system of domestic animals: Published by the Armed Forces Institute of Pathology in cooperation with the American Registry of Pathology and the World Health Organization Collaborating Center for Worldwide Reference on Comparative Oncology; 2003. | |||
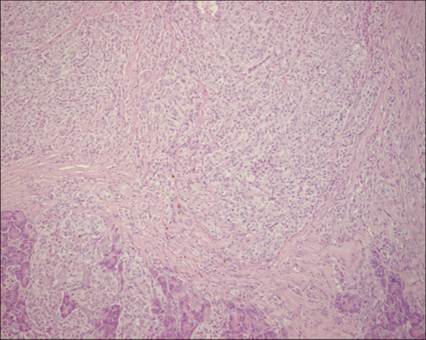
Figure 8.36 Histopathology of a malignant insulinoma (islet cell carcinoma) from a dog. Low-power view of a pancreatic islet cell tumor infiltrating the surrounding exocrine parenchyma through a dense band of fibrous tissue (capsule). Neoplastic cells are arranged in small cords and nests supported by a thin fibrovascular stroma. Hematoxylin and eosin (?100).
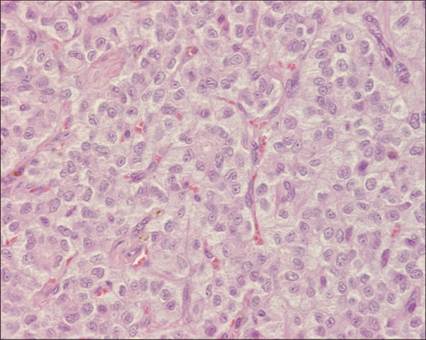
Figure 8.37 Histopathology of a malignant insulinoma (islet cell carcinoma) from a dog. Higher magnification from Figure 8.36. Neoplastic cells are uniform, arranged in small nests supported by fine connective tissue septa containing numerous small capillaries. These cells are cuboidal to polyhedral, with an abundant, pale eosinophilic, finely granular cytoplasm, characteristic of neuroendocrine cells. Nuclei are ovoid, frequently indented, with a stippled chromatin. Hematoxylin and eosin (?400).
Ultrasound
Ultrasonography has low sensitivity to detect canine insulinoma (Robben et al., 2005; Polton et al., 2007) and depends on numerous factors such as the size and the distribution of the lesions, the operator’s experience, equipment quality, animal conformation, and intestinal content (Penninck and d'Anjou, 2013). Insulinoma are usually nodular, lobular, or spherical and hypoechoic compared with the surrounding tissues (Goutal et al., 2012; Vanderperren et al., 2014) but as expected, ultrasonographic findings are non-specific (Figure 8.38).
class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7426/image/image416.jpg" alt=fig8.38.jpg>
Figure 8.38 Sagittal view of the area of the left lobe of the pancreas in a 12-year-old dog. A solitary homogeneous mass of 2 cm in diameter (white arrows) was noted next to the great curvature of the stomach (arrow-head) and adjacent to the splenic vein (black arrow). Pancreatic endocrine tumor was identified histopathologically.
Cytology
Insulinoma has similar cytological features as other endocrine tumors. The cellularity of malignant insulinoma is commonly higher than its benign counterpart and islet cell hyperplasia (Bjorneby & Kari, 2002). Cytological samples are mainly characterized by abundant naked nuclei on a slightly basophilic background corresponding to the cytoplasm of damaged neoplastic cells. The monomorphic cells are incohesive, individually or loosely clustered (sometimes associated with a pseudo-acinar pattern) (Figure 8.39). The neoplastic cells are of small to medium size and frequently display indistinct cytoplasmic borders, but can be round, ovoid to polygonal shaped (Figures 8.40a and 8.40b). The cytoplasm is slightly basophilic and can be associated with many small punctuate and clear vacuoles (Andreasen et al., 2010; Borjesson, 2014). The nucleus is sometimes eccentrically placed, leading to a plasmacytic appearance of neoplastic cells, and can be associated with one small and indistinct to prominent nucleolus (Bjorneby Kari, 2002; Andreasen et al., 2010; Borjesson, 2014). The chromatin pattern is reticular, coarse to finely clumped. Minimal cellular atypia is commonly observed, such as mild to moderate anisokaryosis and binucleation. The minimal cellular atypia cannot allow one to determine the malignancy of the tumor, in other words, its biologic behavior, and histopathology is commonly necessary. Furthermore, immunohistochemistry can be necessary to differentiate endocrine and exocrine tumors in some cases and to determine the subtype of the endocrine tumor and so distinguish the β- and non-β islet cell neoplasms. In the case of insulinoma, the neoplastic cells predominantly secrete insulin, but other pancreatic hormones can also be secreted in lesser amounts (somatostatin, gastrin) (Madarame et al., 2009). Osseous metaplasia has been described in one case of canine insulinoma (Pieczarka et al., 2014).
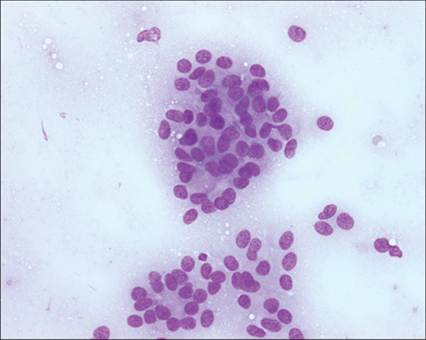
Figure 8.39 Aspirate of a malignant insulinoma (islet cell carcinoma) from a dog. Medium-power view of a pancreatic islet cell tumor characterized by some naked nuclei and loosely cohesive monomorphic medium-sized cells, organized in a pseudo-acinar pattern. Their cytoplasmic borders are very indistinct, and the rare intact cells have a cuboidal to polygonal shape. The cells display a moderate to high nuclear to cytoplasmic ratio, and minimal cellular atypia are observed. May–Grünwald–Giemsa (?400).
Non-epithelial tumors
Primary nonepithelial tumors originating in the pancreas are rare and include fibroma, fibrosarcoma, hemangiosarcoma, liposarcoma, and nerve sheath tumors (Meuten, 2002; Head, 2003; Charles, 2007).
Secondary tumors
The pancreas may be invaded by direct extension from neoplastic diseases originating in contiguous organs such as alimentary lymphoma (Figure 8.41) and digestive (gastric or intestinal) carcinoma or may be involved in multicentric systemic disease (e.g., lymphoma, malignant histiocytosis) and disseminated malignancies through metastasis (Hayden et al., 1993; Meuten, 2002; Swann et al., 2002; Head, 2003; Charles, 2007). Distinguishing primitive pancreatic carcinoma from metastases of cholangiocellular or gastrointestinal carcinoma should be challenging on cytology and even on biopsies (34).
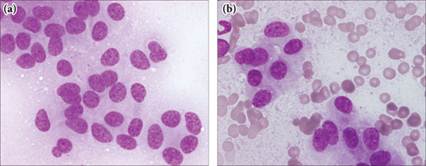
Figures 8.40a,b Aspirate of a malignant insulinoma (islet cell carcinoma) from a dog. Higher magnification from Figure 8.39. The monomorphic neoplastic cells are medium sized with a medium to high nuclear to cytoplasmic ratio, sometimes delimited by very indistinct cytoplasmic borders (8.40a) and characterized by a polygonal shape (8.40b). Cytoplasm is slightly basophilic, and nuclei are round to ovoid, sometimes eccentrically placed, with reticular to finely clumped chromatin. The main minimal cellular atypias observed are mild to moderate anisokaryosis and some binucleations. May-Grünwald Giemsa (x1000).
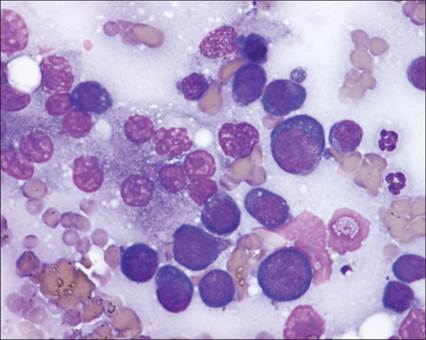
Figure 8.41 Aspirate of a pancreatic lymphoma. Presence of some hyperplastic acinar pancreatic cells associated with many round blastic cells. These blastic cells are large-sized and present a high nuclear to cytoplasmic ratio, a deeply basophilic cytoplasm, and a round to irregular nucleus associated with a finely reticulated chromatin pattern with one or numerous small to large nucleoli. These cells are highly suggestive of a high-grade lymphoma. May–Grünwald–Giemsa (?1,000).