Acute pancreatitis
Definition
Canine and feline acute pancreatitis is characterized by variable degrees of parenchymal pancreatic necrosis often with peripancreatic fat necrosis, in association with neutrophilic inflammation, but without underlying permanent changes such as fibrosis (Watson et al., 2007; Zachary & McGavin, 2013).
Uncommon pancreatic complications of acute pancreatitis are abscesses, pseudocysts, and phlegmon (Charles, 2007; Washabau & Day, 2012).Prevalence and gross anatomy
Prevalence of acute pancreatitis differs according to the authors, depending on different classification systems and inclusion criteria. In a study on 101 dogs randomly selected at necropsy (Newman et al., 2006), neutrophilic inflammation was identified in 32 dogs (32%). In cats, it is uncommon to diagnose lesions of acute pancreatitis alone; however lesions of acute and chronic pancreatitis frequently occur concurrently, with a prevalence ranging from 9.6% (De Cock et al., 2007) to 44% (Forman et al., 2004).
The distribution of lesions of acute pancreatitis can be focal (contained in a localized area), multifocal, or diffuse. Hallmarks of acute inflammatory pancreatic lesions include swelling of the organ due to interstitial or interlobular edema; vascular lesions from hyperemia to petechiae, ecchymosis, or extensive hemorrhages; soft, gray-yellow areas of parenchymal necrosis; white chalky areas of peripancreatic fat necrosis (Figure 8.15) with hyperemic borders; and fibrin exudates on serosa (exudative peritonitis) with loose adhesions between affected portions of the pancreas and adjacent tissues (omentum, mesentery, liver…) (Charles, 2007; Zachary & McGavin, 2013).
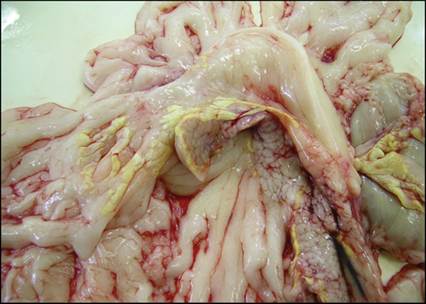
Figure 8.15 Pancreas and omentum from a cat infected by a hypervirulent calicivirus.
The pancreas is moderately hyperemic and the pancreatic lobulation is exaggerated by interlobular edema. Multiple white chalky areas of fat necrosis are seen on the surface of the pancreas and in the omentum mainly close to the pancreas.
Histopathology
Acute elementary inflammatory lesions in the pancreas are consistent with acinar cell necrosis in randomly scattered foci or involving entire lobules, often delineated by a rim of degenerate neutrophils; peripancreatic fat necrosis often with dystrophic mineralization (saponification) (Figure 8.16); interlobular septal neutrophilic infiltrate, edema, and/or fibrin exudates (Figure 8.17); and, most frequently observed in dogs, interstitial hemorrhages (Charles, 2007; De Cock et al., 2007; Zachary & McGavin, 2013). These lesions can occur in variable intensity from case to case.
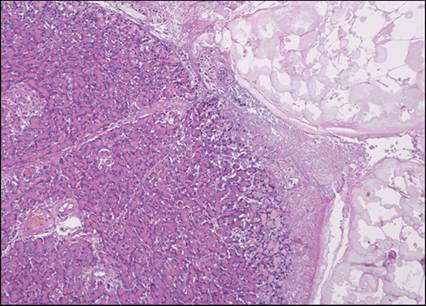
Figure 8.16 Same case as Figure 8.15: pancreas and omentum from a cat infected by a hypervirulent calicivirus. Hypervirulent caliciviruses induce subcapsular coagulative necrosis of the pancreatic exocrine parenchyma with cytoplasmic pallor and nuclear pyknosis. The peripancreatic fat (on the right of the picture) is also necrotic with dystrophic mineralization. There is fibrin exudation between necrotic omental fat and pancreatic parenchyma. Hematoxylin and eosin (?100).
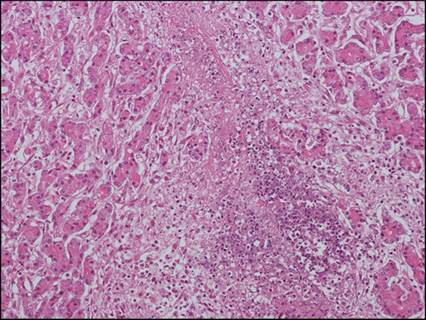
Figure 8.17 Acute suppurative pancreatitis from a cat. Pancreatic lobules are separated by interlobular collection of degenerated neutrophils (suppuration) with fibrin exudates. Pancreatic exocrine acini are separated by intralobular edema. Hematoxylin and eosin (?200).
In cats, two distinct acute entities are recognized: acute pancreatic necrosis (or acute necrotizing pancreatitis), in which parenchymal and fat necrosis are the major components with varying amounts of inflammation, hemorrhage, and mineralization, and acute suppurative pancreatitis that differs from the former by the intensity of neutrophilic inflammation which is the predominant feature, and less parenchymal necrosis (Hill et al., 1993; Charles, 2007; Washabau & Day, 2012).
Ultrasound
Changes observed in cases of acute pancreatitis are related to pancreatic edema, hemorrhage, and necrosis as well as focal peritonitis and fat saponification (Figure 8.18) (Nyland et al., 2002; Larson, 2016). Sonographic appearance is variable based on the severity and the duration of the inflammation (Penninck and d'Anjou, 2013). An enlarged, ill-defined, irregularly shaped, and strongly hypoechoic organ is usually observed. However, severe pain, free abdominal fluid, excessive gas within the gastrointestinal tract, and abnormal peristalsis can make it difficult to perform the examination. In dogs, the right lobe tends to be more commonly affected, whereas in cats, the body and the left lobe are more often involved. Ultrasonographic changes in cats are often more subtle and of later onset than in dogs (Hecht & Henry, 2007; Penninck & d'Anjou, 2013; Penninck et al., 2013).
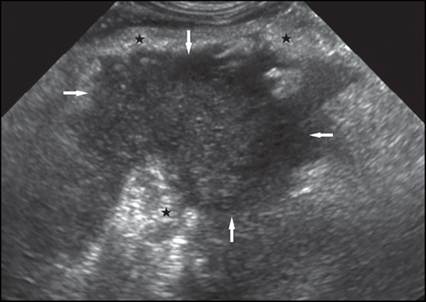
Figure 8.18 Sagittal view of the right cranial abdomen of a dog with acute pancreatitis. An enlarged hypoechoic pancreas (white arrows) surrounded by hyperechoic and bright mesenteric fat (black stars) can be seen dorsally to the descending duodenum.
Cytology
The cellularity associated with acute pancreatitis is higher than in chronic pancreatitis. Aspirates reveal a neutrophilic infiltrate with intact and degenerating neutrophils (Figure 8.19). Exocrine pancreatic epithelial cells may be present and show some degree of hyperplastic change (Figures 8.20 and 8.21); rare ductal epithelial cells may also be observed (Bjorneby & Kari, 2002; Cordner et al., 2015). Necrotic background is often present (Figure 8.22). Calcified debris may also be found (Figure 8.23) (Bjorneby & Kari, 2002; Cordner et al., 2015). Mixed inflammatory cells can sometimes be noted with large foamy or phagocytic macrophages in addition to the neutrophils. Note that foamy macrophages can be observed in acute or chronic pancreatitis aspirates.
In some cases, only necrotic material can be found without any exocrine pancreatic epithelial cells or intact inflammatory cells. 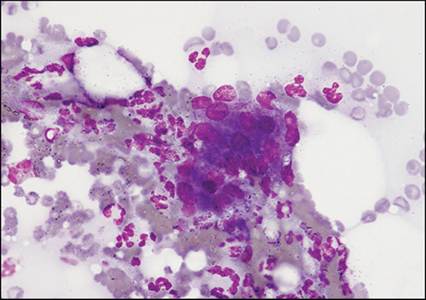
Figure 8.19 Aspirate of acute pancreatitis from a dog. The specimen is characterized by a hemorrhagic background, many nondegenerate neutrophils, and a cluster of exocrine pancreatic epithelial cells showing moderate anisokaryosis. May–Grünwald–Giemsa (?400).
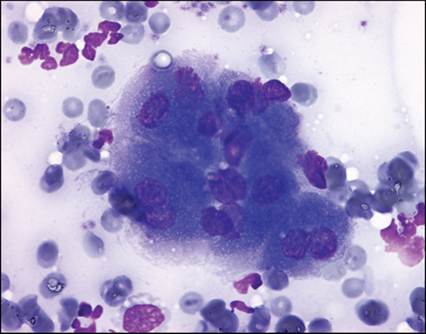
Figure 8.20 Aspirate of acute pancreatitis from a dog. Nondegenerate neutrophils surround two acini of exocrine pancreatic epithelial cells showing moderate anisokaryosis and prominent basophilic nucleoli. May–Grünwald–Giemsa (?1,000).
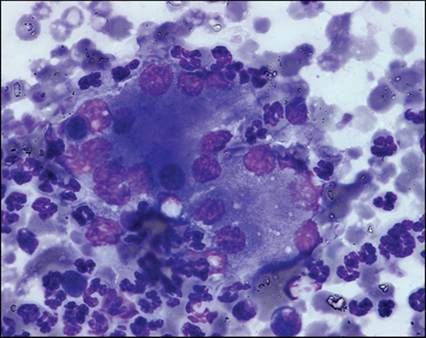
Figure 8.21 Aspirate of acute pancreatitis from a dog. The exocrine pancreatic epithelial cells show a highly basophilic cytoplasm and some binucleations. The neutrophils are mostly nondegenerate. May–Grünwald–Giemsa (?1,000).
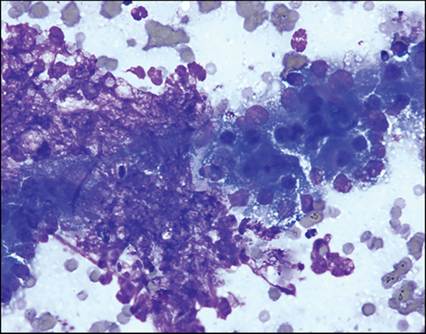
Figure 8.22 Aspirate of acute pancreatitis from a cat. The specimen is characterized by a hemorrhagic background and necrotic debris. Many degenerate neutrophils surround exocrine pancreatic epithelial cells showing marked anisocytosis and anisokaryosis. The cytoplasm of the epithelial cells shows decreased granularity and many small clear vacuoles consistent with cellular degeneration. May–Grünwald–Giemsa (?400).
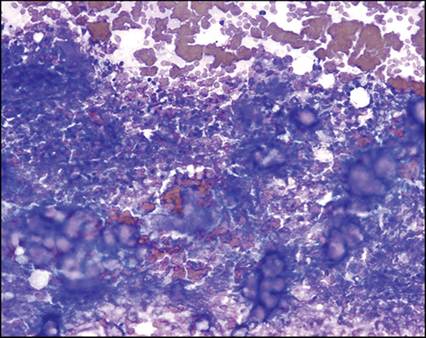
Figure 8.23 Aspirate of acute pancreatitis from a cat. The background is highly hemorrhagic and necrotic, containing many degenerate neutrophils.
Calcific debris appear as tridimensional amorphous refractile material. May–Grünwald–Giemsa (?200).
Chronic pancreatitis
Definition
Chronic pancreatitis is the result of progressive destruction of the pancreas by repeated mild episodes of acute pancreatic necrosis and inflammation (Bostrom et al., 2013; Zachary & McGavin, 2013). Owing to modest regenerative capacity, the destruction of pancreatic parenchyma causes progressive loss of glandular tissue and its replacement by fibrosis. The hallmarks of chronic inflammation in the pancreas are fibrosis and exocrine parenchymal atrophy, which are considered permanent changes (Washabau & Day, 2012; Zachary & McGavin, 2013).
Prevalence and gross anatomy
As for acute pancreatitis, the published prevalence of chronic pancreatitis differs according to different authors but remains high. In a study based on 151 unselected canine post-mortem examinations without pancreatic autolysis, chronic pancreatitis was identified in 34% of dogs (Watson et al., 2007). In another study on 101 dogs randomly selected at necropsy (Newman et al., 2006), lymphocytic infiltration was identified in 53 dogs (52%). In cats, an overall prevalence of 67% was identified in a group of 115 unselected feline post-mortem examinations and a prevalence as high as 45% of apparently healthy animals (De Cock et al., 2007).
Chronic pancreatitis is macroscopically characterized by distortion and shrinkage of a part or the whole organ, with often exaggerated lobulation, a gray to whitish color, firm consistency, and fibrous adhesions to adjacent tissues (Charles, 2007; Zachary & McGavin, 2013).
Histopathology
The microscopic appearance of chronic pancreatitis is characterized by disruption of the normal pancreatic architecture due to variable amounts of fibrosis (Figure 8.24) in association with lymphocyte and plasma cell infiltrates, parenchymal atrophy (Figure 8.25), and occasional ductal cystic dilation in cats (Charles, 2007; De Cock et al., 2007; Watson et al., 2007; Zachary & McGavin, 2013).
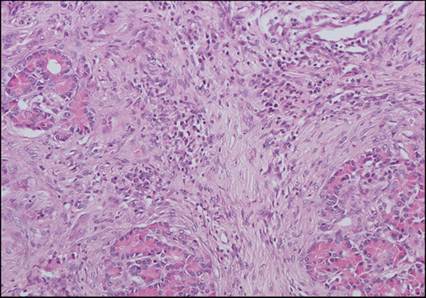
Figure 8.24 Chronic pancreatitis from a dog. Pancreatic microscopic structure is severely modified by interlobular fibrosis which extends into lobules, separating and replacing exocrine acini, associated with a sparse infiltrate of small lymphocytes. Residual exocrine pancreatic acini are well-differentiated with bright eosinophilic zymogen granules. Hematoxylin and eosin (?200).
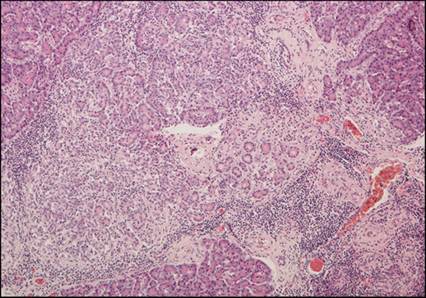
Figure 8.25 Chronic lymphocytic and atrophic pancreatitis from a cat. There is marked exocrine pancreatic lobular atrophy associated with perilobular and intralobular, dissecting, fibrosis, and lymphocytic infiltrate. Atrophic acini exhibit pale cytoplasm with severe depletion in zymogen granules. Some well-developed lobules are observed in the periphery of the atrophic one. Hematoxylin and eosin (?100).
Some authors have highlighted differences in histological appearance and distribution of fibrosis in different breeds of dogs and have described a periductular, interlobular pattern of fibrosis and inflammation in Cocker Spaniels compared to an acinar, dissecting intralobular pattern in other breeds (Watson et al., 2007).
Acute-on-chronic pancreatitis can be observed and is characterized by edema, necrosis, neutrophils (hallmarks of acute pancreatitis) admixed with lymphocytes and plasma cells, and underlying fibrosis (hallmarks of chronic pancreatitis). These observations corroborate the theory that irreversible damage to the pancreas may be caused by repeated incidents of acute pancreatitis (Watson et al., 2007; Bostrom et al., 2013).
Ultrasound
In case of chronic pancreatitis, the changes may be nonexistent or very subtle (Penninck et al., 2013); the pancreas usually remains a well-defined hypoechoic structure that contrasts with the slightly hyperechoic peripancreatic mesentery (Penninck and d'Anjou, 2013). Irregular margins, mild hyper/hypotrophy, heterogeneous parenchyma, calcification, and scarring can be encountered (Nyland et al., 2002). Some cases of chronic pancreatitis appear as a mass-lesion on ultrasound and must not be mistaken for pancreatic neoplasia (Watson et al., 2007). Ultrasonography has low sensitivity in case of chronic pancreatitis.
Cytology
Cytological specimens in cases of chronic pancreatitis are typically less cellular than in acute pancreatitis and often yield peripheral blood. Calcified debris and clusters of pancreatic acinar cells and ductal epithelial cells can be seen with hyperplastic changes sometimes mistaken for neoplasia (Bjorneby & Kari, 2002). Mixed inflammatory cells are found and include neutrophils, foamy or phagocytic macrophages, lymphocytes, and plasma cells (Figures 8.26 and 8.27) (Bjorneby & Kari, 2002; Cordner et al., 2015). In our experience, fibrosis is never seen in aspirates, and the distinction between acute and chronic pancreatitis is usually not possible with cytology alone.
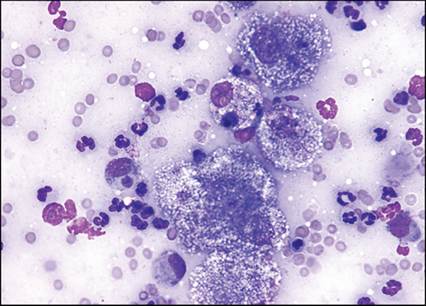
Figure 8.26 Aspirate of chronic pancreatitis from a cat. A small cluster of non-reactive exocrine pancreatic epithelial cells is surrounded by mixed inflammatory cells: many non-degenerate neutrophils and some large foamy macrophages. May–Grünwald–Giemsa (?400).
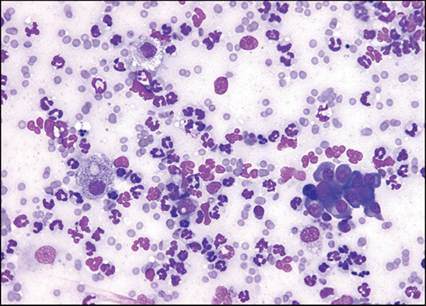
Figure 8.27 Aspirate of a chronic pancreatitis from a cat. Same case as Figure 8.26. Abundant inflammatory cells are present: mainly neutrophils but also some foamy macrophages and a small cluster of plasma cells. Some small lymphocytes are present but it is difficult to know their origin (inflammation or iatrogenic blood contamination). May-Grünwald Giemsa (x400).