CASES
CASE 1
Signalment/history
Seven-year-old, spayed female domestic shorthair barn cat. The patient presented 2 weeks ago for significant weight loss (>50% reduction over 1 year).
The owners reported normal appetite and no vomiting.Diagnostics
A CBC revealed a moderate to marked normocytic normochromic anemia (Hct = 15% [0.15 l/l]; reference interval [RI] = 25–45 [0.25–0.45]), thrombocytopenia (platelets = 31 ? 106/μl [RI = 200–500]), and normal white blood cell counts with minimal toxicity noted. A biochemistry profile showed hyperproteinemia (8.3 g/dl [83 g/l]; RI = 6.0–8.0 [60–80]), hyperglobulinemia (6.3 g/dl [63 g/l]; RI = 2.8–4.8 [28–48]), and hypoalbuminemia (2.0 g/dl [20 g/l]; RI = 2.3–2.5 [23–25]). The patient was FIV/FeLV negative and an fPLI SNAP® test was normal.
Treatment
No significant changes were reported after a 1-week course of doxycycline; however, the patient was noted to be dehydrated and had lost more weight, so was hospitalized for supportive care and additional diagnostics. Repeat blood work showed an unchanged anemia (Hct = 15% [0.15 l/l]) and mild icterus (serum bilirubin = 0.6 mg/dl [10.26 μmol/l] [RI = 0–0.3, 0–5.13]). Reticulocyte count failed to show evidence of regeneration. Mycoplasma PCR was negative. Abdominal radiographs were obtained and revealed decreased serosal detail; therefore an abdominal ultrasound was performed. The liver was diffusely enlarged and slightly hyperechoic, and a minimal amount of sludge was noted in the common bile duct. There was also mild splenomegaly, the duodenal and jejunal walls were slightly thickened with altered echogenicity, and a scant amount of free peritoneal fluid was noted. Aspirates of the liver, spleen, and abdominal fluid were submitted to a reference laboratory; images from the liver aspirate are shown (Figures 9.59a, b).
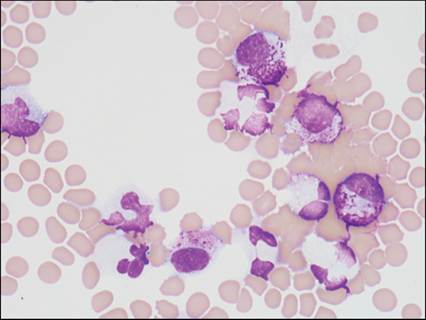
Figures 9.59 Feline hepatic aspirate (Wright–Giemsa, 1,000? magnification).
Cytologic description
Clusters of cohesive hepatocytes are present. These polygonal cells have an abundant amount of basophilic to pink granular cytoplasm, a single round nucleus with finely stippled chromatin, and a single prominent nucleolus. Macrophages, neutrophils, and lymphocytes are present. A macrophage contains phagocytized yeast, which are round to oval, 2–4 μm in diameter, with a thin clear capsule, narrow-based budding, and a purple crescent-shape along one end representing nuclear material. A small orange crystal is noted at the bottom center of Figure 9.59b and is consistent with hematoidin.
Cytologic interpretation
Pyogranulomatous hepatitis with Histoplasma capsulatum.
Outcome
The spleen had similar findings. The fluid sample was of low cellularity. The patient was started on itraconazole (10 mg/ml) and over the next week showed appropriate clinical and biochemical improvement (Hct increased to 20% [0.2 l/l], biochemical icterus resolved). The patient was discharged with instructions to follow a 4–6-month course of itraconazole and was lost to follow-up.
CASE 2
Signalment/history
Nine-year-old, spayed female Golden Retriever. The patient had a 7 cm diameter, grade II peripheral nerve sheath tumor removed from the dorsal intrascapular area 9 months ago. Adequate margins could not be confirmed and the patient was started on metronomic chemotherapy consisting of cyclophosphamide and piroxicam. The patient also suffered from arthritis, for which she was receiving carprofen. She had a history of mildly increased liver enzyme activity. She re-presented to her primary care veterinarian for vomiting and lethargy. In-house blood work revealed marked elevation of ALT, a mild anemia, and neutrophilia (Table 9.2, day 0). The chemotherapy was discontinued and antibiotic and hepatoprotectant therapies (amoxicillin/clavulanic acid and Denamarin) were started.
The clinical signs quickly resolved. Over the next 3 weeks the leukocytosis, anemia, and ALT values continued to decrease while concordant mild increases in ALP were noted (Table 9.2, days 0–18).Table 9.2 Select values from serial evaluation of a 9-year-old, spayed female Golden Retriever dog. Results are reported as value (reference interval*). Values outside the reference interval are in bold
| Day 0 | Day 4 | Day 12 | Day 18 | Day 47 | Units | |
| ALP | 141 (0–140) | 164 (0–140) | 156 (0–140) | 133 (7–92) | 152 (7–92) | U/l |
| cALP | 71 (0–40) | 101 (0–140) | U/l | |||
| ALT | 2,332 (0–120) | 906 (0–120) | 637 (0–120) | 203 (8–65) | 137 (8–65) | U/l |
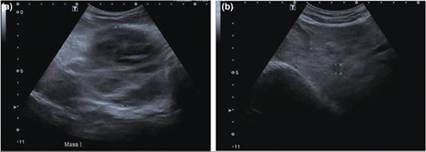
| GGT | a 7 cm hyperechoic mass in the mid-abdomen, likely associated with the liver (Figures 9.60a, b). Ultrasound-guided aspirates of the liver mass and normal liver were acquired. Representative images from the liver mass cytology are shown (Figures 9.61a–c). The biochemical data are listed in Table 9.2. Figures 9.60a,b Ultrasound images of abdominal masses present in a 9-year-old, spayed female Golden Retriever dog. (a) A 7.6 cm mass effect was noted in the cranial abdomen. It was challenging to determine if the mass effect was associated with the liver, spleen, or independent of these organs. (b) The liver was diffusely enlarged, and multiple small masses, some measuring up to 3.6 cm, were observed. (Courtesy Dr. Elizabeth Peters.)
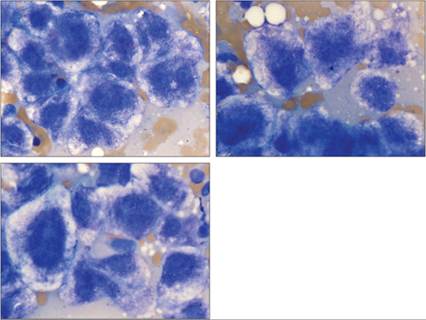
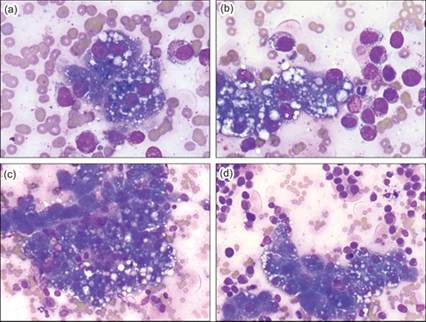
Figures 9.61 Canine liver sample (Wright–Giemsa, 1,000? magnification).
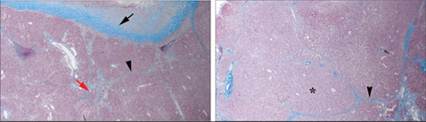
Cytologic description There are large cohesive clusters of hepatocytes present, which have an abundant amount of basophilic to pink granular cytoplasm, a centrally located round nucleus with finely stippled chromatin, and a single prominent nucleolus. These cells have a marked degree of anisocytosis, anisokaryosis, variable N:C ratio, frequent trinucleation, nuclear molding, and multiple nucleoli. These cells frequently have moderate to abundant amounts of clear foamy cytoplasmic rarefaction, consistent with glycogen or hydropic degeneration. The background consists of minimal cellular debris in a moderately proteinaceous fluid.Cytologic interpretation Likely regenerative nodule; rule out hepatocellular carcinoma. Outcome A follow-up on day 47 revealed that the biochemistry profile continued to improve but the mass was increasing in size on ultrasound. A surgical biopsy was elected. Histology (Figure 9.62) revealed multifocal, 3 cm nodules composed of smaller nodules. The smaller nodules demonstrated a fibrous connective tissue capsule and bridging between portal triads (bridging fibrosis), atrophied hepatocytes, and serpiginous biliary ducts (biliary hyperplasia). Enlarged hepatic lobules lacked a central vein and had disorganized hepatic cords present, which were compressing adjacent parenchyma (hyperplastic nodule). Concurrently, these findings indicate hepatic cirrhosis (fibrosis and regeneration) and suggest massive hepatic necrosis. The FNA sample demonstrates the marked dysplasia that can occur with a strong regenerative effort. Figure 9.62 Liver mass, histologic sections. Black arrow indicates thickened capsule. Black arrowhead indicates bridging fibrosis. Red arrow indicates lobular compression and atrophy. Asterisk indicates regenerative nodule (Mason-trichrome, 50? magnification). (Courtesy Dr. Arnon Gal.)
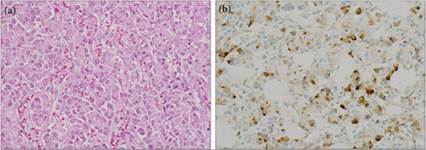
CASE 3 Signalment/history Eleven-year-old, neutered male mixed-breed dog. The patient presented with a 3-week history of sudden onset seizure activity, which was refractory to medical management. Physical examination At presentation the dog appeared sedated to mentally inappropriate. Examination revealed hyperthermia (102.9°F [39.4°C]), mild tachycardia (108–140 bpm), and hypertension (systolic, 140–180 mmHg). On a hand-held and bench-top glucometer, the patient was hypoglycemic, and continued to be hypoglycemic (diastase and PAS negative after diastase digestion of the glycogen.(Note: selected data from this case have been published previously [Moore et al., 2015].) Figures 9.65a,b Histologic sections of the liver mass. (a) Note the typical neuroendocrine appearance of round cells in nests and packets surrounded by a fine connective tissue stroma (H&E, 200? magnification). (b) The neoplastic cells stained positive for insulin (anti-insulin, diaminobenzidine, hematoxylin counterstain, 200? magnification). A histologically similar insulin-positive mass was present in the pancreas. (Courtesy Dr. Caroline Chu.)
CASE 4 CASE material provided by Dr. Caitlyn Connor. Signalment/history Five-year-old, spayed female French bulldog. The patient was presented for a 3-week history of persistent vomiting and diarrhea, refractory to symptomatic therapy (maropitant, ondansetron, antibiotics). Diagnostics A CBC revealed a moderate macrocytic, normochromic nonregenerative anemia (Hct = 28.3%; reference interval [RI] = 42–60), moderate thrombocytopenia (platelets = 95 ? 103/µL; RI = 226–424), and a moderate leukocytosis (WBC 37.3 ? 103/µL; RI = 4.2–12.9) characterized by a moderate neutrophilia (segmented neutrophils = 24.99 ? 103/µL; RI = 2.70–8.50) with a minimal regenerative left shift (band neutrophils = 0.373 ? 103/µL; RI = 0.00–0.300) with minimal signs of toxicity noted, a moderate monocytosis (monocytes = 3.357 ? 103/µL; RI = 0.100–1.00), minimal basophilia (basophils = 0.373 ? 103/µL; RI = 0–0), and 17% ‘other cells’ (Figure 9.66). Figure 9.66 Composite image of the nucleated cells found in the peripheral blood smear of a dog (modified Wright–Giemsa, 1,000? magnification).
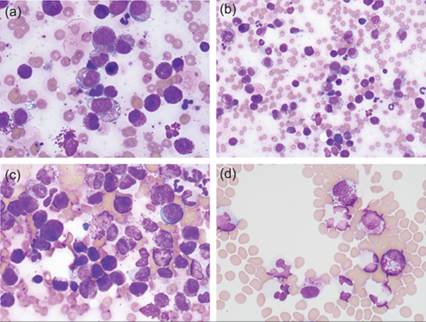
A serum biochemistry profile displayed increased liver enzyme activity (ALT = 672 U/l; RI = 12–106; ALP = 446 U/l; RI = 13–102) and cholestasis (total bilirubin = 1.20 mg/dl; RI = 0.00–0.20), a mild hypoproteinemia (5.2 g/dl; RI= 5.4–7.1) characterized by a mild hypoalbuminemia (2.8 g/dl;RI = 3.3–4.2), a mild disproportionate hypochloridemia (98 mmol/l; RI = 106–114; sodium within reference interval at 144 mmol/l; RI = 143–150), a mild to moderate hypokalemia (3.3 mmol/l; RI = 3.7–5.1), mild hypocalcemia (9.2 mg/dl; RI = 9.5–11.2), and a mild hyperphosphatemia (6.4 mg/dl; RI= 2.7–5.2). Thoracic radiographs did not show any significant findings. Abdominal radiographs exhibited hepatosplenomegaly, and abdominal ultrasound revealed hepatosplenomegaly with multiple splenic nodules, markedly enlarged jejunal lymph nodes, abdominal effusion, and a gastro-duodenal junction ulcer. Aspirates of the liver, spleen, jejunal lymph node, and abdominal fluid were submitted to a reference laboratory. Images from the liver aspirate are shown (Figure 9.67a–d). Figures 9.67a–d Canine hepatic aspirate (modified Wright–Giemsa, a and b 500? magnification, c and d 1,000? magnification).
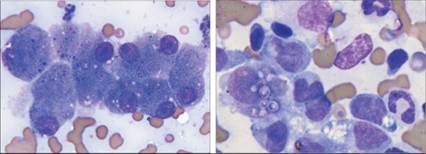
Cytologic description Liver: there are many hepatocyte clusters. Hepatocytes are round to polygonal with mild to moderate amounts of deeply basophilic cytoplasm and a variable nuclear to cytoplasmic ratio. They occasionally contain blue–black granular material consistent with lipofuscin or other pigment, and many hepatocytes contain moderate amounts of distinct clear cytoplasmic vacuolization consistent with lipid. Nuclei are round to ovoid with finely reticular chromatin and one to rarely two distinct nucleoli. Anisocytosis and anisokaryosis are mild to moderate, and there are moderate numbers of binucleate cells. Few trinucleated cells are seen. There are many large discrete round cells with moderately expanded amounts of lightly basophilic cytoplasm and a round nucleus with smooth to stippled chromatin. Most of the cells have at least minimal amounts of fine to slightly coarse metachromatic cytoplasmic granulation. In most cells, this granulation is evenly distributed across the cytoplasm. In some cells, the granulation forms a small packet adjacent to the nucleus. The cells display moderate anisocytosis and anisokaryosis, with binucleation apparent and some cells having more distinct nucleoli. There are pigment-laden macrophages and few neutrophils seen in the background with cellular debris and proteinaceous fluid. Blood smear: the leukocyte population appears moderately increased and is composed of mostly nondegenerate neutrophils with no appreciable toxic change. Monocytes appear morphologically normal and very few monocytes contain green pigment within the cytoplasm. Lymphocytes are predominantly small with a few intermediate-sized lymphocytes that are slightly smaller than the diameter of a neutrophil with deeply basophilic cytoplasm. Their nuclei are round with finely stippled chromatin and no discernible nucleoli. Eosinophils and basophils appear morphologically normal. The cells marked as ‘others’ are individualized mast cells. They contain moderate amounts of cytoplasm with variable numbers of fine to coarse deeply metachromatic granules distributed diffusely throughout the cytoplasm. Nuclei are centrally placed and ovoid to rarely irregular with fine stippled chromatin and no discernible nucleoli. No infectious etiologic agents are seen. Cytologic interpretation Liver: mast cell tumor; hepatocellular vacuolization consistent with lipid. Peripheral blood: circulating mast cells due to mast cell neoplasia; mild macrocytic, nonregenerative anemia, suspect anemia of chronic disease; mild thrombocytopenia with evidence of thrombopoiesis. Outcome All sampled tissue (liver, spleen, lymph node, abdominal fluid, and peripheral blood) contained the neoplastic mast cells, providing evidence of disseminated disease (Figures 9.68). A primary tumor was not evident by imaging. Because of worsening clinical condition and poor prognosis, the patient was euthanized. Necropsy was not performed. Figures 9.68a–d Spleen, jejunal lymph node, and abdominal fluid from a 5-year-old dog with mast cell neoplasia in the liver and peripheral blood. (a) The splenic aspirate had severe infiltration of neoplastic mast cells with variable amounts of metachromatic granules. Few small lymphocytes and neutrophils are present. (b) There were only scant lymphocytes present in the jejunal lymph node, but there were abundant neoplastic mast cells with variable amounts of metachromatic granules. (c) The neoplastic mast cells found in the other organs were present in the abdominal effusion and were more prominent than could be explained by peripheral blood contribution alone (modified Wright’s Giemsa, 1,000? magnification).
The primary tumor site was not identified in this patient. It is possible that the tumor originated in the liver or spleen or that these sites were metastasis from another location. Very low numbers of mast cells will be seen in healthy peripheral blood. The number and morphology of the circulating mast cells, and their morphologic similarity to the cells found in the liver, spleen, and jejunal lymph node, indicate circulating neoplastic mast cells. Circulating mast cells can be seen with hematogenous spread of visceral mast cell neoplasia and can also be seen with mast cell leukemia or mast cell neoplasia originating in the bone marrow; both of these conditions have a poor prognosis (Willman et al., 2021). The hepatocellular atypia, lipid vacuolization, and the mixed hepatopathy appreciated on biochemistry were sequelae to the mast cell neoplastic infiltration of this organ rather than indicative of hepatic lipidosis. The nonregenerative anemia and thrombocytopenia are likely indirect sequelae to this disease process. The intracellular green pigment in the monocytes is nonspecific; however, it has been described in dogs with IMHA, post-blood transfusion, or even severe liver disease, which may be present in this case ( Gorup et al., 2017; Soos et al., 2019). Acknowledgments The author would like to thank Dr. Walter Hoffman for his assistance with this work.
More medical literature on Medic.Studio
More on the topic CASES:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|