Cases
CASE 1
Signalment/history
A 9-year-old spayed female domestic shorthair cat presents for a 1-week history of lethargy and progressive anorexia. The cat is dehydrated and has small ulcerations below her tongue.
Blood work reveals azotemia with marked increases in both urea nitrogen and creatinine. An abdominal ultrasound shows bilaterally enlarged kidneys. FNAs are obtained from both kidneys (Figures 10.69a, b, representative of both aspirates). 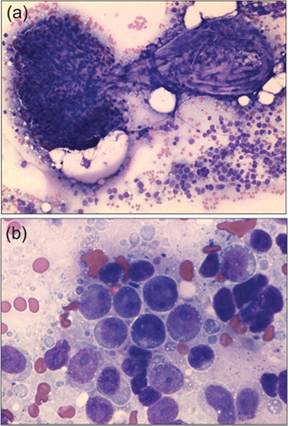
Figures 10.69a,b (a) 200? magnification view of the renal aspirate. (b) 600? magnification view of a highly cellular region (Diff-Quik®).
Cytology
A single glomerulus is present, confirming the aspirate is renal in origin. No other renal tissue is observed. Instead, the high cellularity is attributed to a proliferation of large lymphocytes with deeply basophilic cytoplasm, finely stippled chromatin, and multiple nucleoli.
Diagnosis
Bilateral renal lymphoma causing acute kidney injury.
Cases 2 and 3 (compare and contrast)
Signalment/history
· CASE 2. A 12-year-old neutered male Miniature Pinscher presents for occasional straining to urinate. An abdominal ultrasound reveals a large mass originating in the trigone region of the bladder (Figure 10.70a). A traumatic catheterization of the mass is performed (Figure 10.70b).
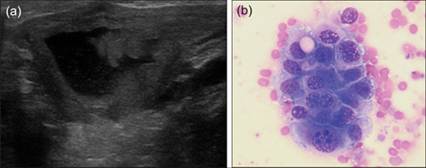
Figures 10.70a,b (a) Ultrasound of the bladder mass (trigone region). (b) A representative cluster of urothelial cells recovered via traumatic catheterization (modified Wright’s, 600? magnification).
· CASE 3. A 10-year-old neutered male Yorkshire Terrier presents for sporadically urinating blood. An abdominal ultrasound reveals a papillary mass in the cranioventral region of the bladder (Figure 10.71a).
Several small bladder stones are also seen on ultrasound. A traumatic catheterization of the mass is performed (Figure 10.71b). 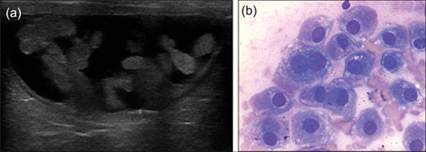
Figures 10.71a,b (a) Ultrasound of the bladder mass (cranioventral region) (b) A representative cluster of urothelial cells recovered via traumatic catheterization (modified Wright’s, 600? magnification).
Cytology
· The cells from Case 2 display pleomorphism suggestive of urothelial carcinoma: moderate anisocytosis, moderate anisokaryosis, increased and variable N:C ratios, frequent binucleation, and multiple nucleoli.
· The cells from Case 3 display mild anisocytosis and occasional binucleation with monomorphic nuclei, changes suggestive of hyperplastic urothelial cells, with uroliths the presumed predisposing factor. Both cases have very suggestive ultrasonographic and cytologic findings, but histopathology and/or BRAF testing is recommended because cytology results are not definitive.
Diagnosis
· CASE 2. Urothelial carcinoma (confirmed by cytoscopic biopsy).
· Case 3. Polypoid cystitis (confirmed by cystotomy, urolith removal, and excisional biopsy).
CASE 4
Signalment/history
An 8-month-old female Yorkshire Terrier is referred for surgical correction of a portosystemic shunt. The shunt was diagnosed 2 months earlier based on clinical signs and blood work abnormalities (decreased albumin and urea nitrogen, increased bile acids). At this visit, the owner reports a new problem of inappropriate urination. A urine sample is collected by cystocentesis (Figure 10.72).
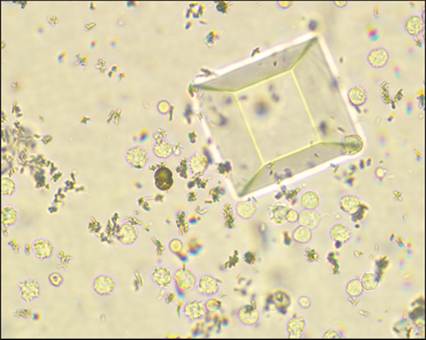
Figure 10.72 Wet-mount preparation of the urine sediment (unstained, 400? magnification).
Microscopy
A single intact ammonium biurate crystal is present, consistent with this patient’s portosystemic shunt.
In addition, there are large numbers of leukocytes and rare erythrocytes. There are many small, variably shaped structures that are difficult to identify. They may be bacteria, but they could also be fragments of crystals. A single large struvite crystal is also present.Additional test results
Gram staining reveals low numbers of bacterial cocci, and urine culture identifies a Staphylococcus sp. The urine pH is high (8.0). The majority of the small, variably shaped structures from the wet mount do not stain with Wright’s or Gram stain, consistent with crystal fragments.
Diagnosis
(1) Urinary tract infection with urease-producing Staphylococcus sp. and secondary struvite crystal formation. (2) Ammonium biurate crystals, consistent with portosystemic shunt.
CASE 5
Signalment/history
An 8-year-old female spayed domestic shorthair cat presents with a history of recurrent urinary tract infections, presumed the result of lifelong urinary and fecal incontinence secondary to neurologic injury. The patient has been treated with multiple courses of various antibiotics in the past. Her most recent urine culture, performed one month prior to this visit, revealed large numbers of multi-drug resistant Enterococcus faecium. A cytocentesis urine sample is collected as follow-up to that infection (Figure 10.73).
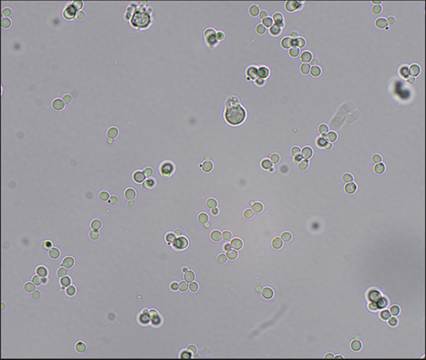
Figure 10.73 Wet-mount preparation of the urine sediment (unstained, 500? magnification).
Microscopy
Numerous round to oval refractile structures are noted, along with rare leukocytes. Differentials for the structures include erythrocytes, fat droplets, and yeast organisms. Small narrow-based buds are occasionally noted, most consistent with yeast.
Additional test results
A line preparation of urine sediment is prepared, dried, and stained with Wright’s stain (Figure 10.74). The structures stain deeply basophilic, inconsistent with erythrocytes (which would stain lightly eosinophilic) or fat droplets (which would not stain).
Instead, this staining is consistent with a yeast organism, confirming the initial sediment exam suspicion. Culture reveals a pure population of Candida glabrata. 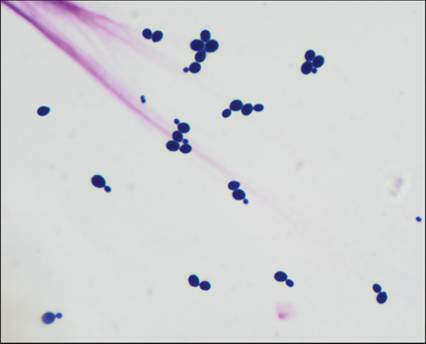
Figure 10.74 Line preparation of urine sediment. Deeply basophilic round to oval yeast organisms display occasional narrow-based budding (modified Wright’s, 1,000? magnification).
Diagnosis
Candida infection. Very low numbers of Candida organisms may represent mucocutaneous contamination in voided samples, but large numbers are a pathologic finding. The yeast infection in this patient has likely arisen secondary to the chronic antibiotic usage, although the neurologic injury and incontinence may also have predisposed to this infection. The inflammatory reaction is minimal, which could indicate underlying immunosuppression.