Cases
CASE 1
Signalment/history
A 10-year-old neutered male Labrador Retriever-mix dog was presented for forelimb lameness.
Physical examination
The patient was toe-touching lame on the right forelimb and a swelling was detected in the area of the distal radius.
Radiographic imaging revealed a lytic and proliferative lesion affecting the distal radius (Figure 12.23a). 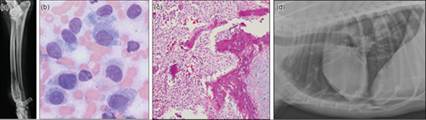
Figures 12.23a–d (a) Digital radiographic image of the lateral aspect of the right forelimb demonstrating a lytic and proliferative bone lesion affecting the distal radius. (Courtesy Laura Garrett.) (b) Cytology of the bone lesion revealed pleomorphic rounded to spindloid neoplastic cells, consistent with sarcoma (Wright–Giemsa: a and b, 1,000? magnification). (Courtesy Anne Barger.) (c) Histopathology of the bone lesion (H&E, 100? magnification). (d) Lateral thoracic radiograph with nodular pulmonary lesions, compatible with metastatic neoplasia. (Courtesy Laura Garrett.)
Cytology
An aspirate of the lesion was obtained using a 20-gauge needle and syringe, and smears of the sample were prepared. The slides were stained with Wright–Giemsa and examined cytologically.
A pleomorphic population of individualized cells was present. The cells varied from rounded to spindloid in shape, with a small to moderate amount of basophilic cytoplasm, a round or oval nucleus, moderate to high N:C ratio, finely to coarsely stippled chromatin, and prominent nucleoli (Figure 12.23b). The cells displayed moderate anisocytosis, anisokaryosis, and anisonucleoliosis, and occasional binucleation. Low numbers of cells contained a few fine, magenta granules within the cytoplasm.
Diagnosis
The cytologic interpretation was sarcoma, with osteosarcoma as the top differential.
Management/outcome
Because of financial limitations, the owners elected limb amputation without other therapeutic modalities. The histopathologic diagnosis was osteosarcoma (Figure 12.23c). Thoracic radiographs prior to surgery did not reveal appreciable metastatic lesions. Four months following limb amputation, the patient was presented for weight loss and lethargy. Thoracic radiographs were repeated, and several discrete nodular lesions, compatible with metastatic disease, were identified (Figure 12.23d). Due to the poor prognosis and declining patient quality of life, the owners elected humane euthanasia.
Discussion
Osteosarcoma is a proliferation of malignant neoplastic osteoblasts that can be identified in the axial and appendicular skeleton. Lesions often arise in the metaphyseal region of long bones. Lesions display variable radiographic changes, but many are both lytic and proliferative. Atypical, pleomorphic mesenchymal cells may be identified on cytologic examination of aspirates of bone lesions, although peripheral blood contamination is common and may limit the conclusiveness of cytology. Staining for ALP activity may be helpful in samples of appropriate cellularity, but neoplastic cells must be differentiated from reactive, non-neoplastic osteoblasts that may be present concurrently. Histopathology may be necessary to differentiate osteosarcoma from other sarcomas that may be found in bone lesions. Pulmonary metastasis is common, although other sites, including skin and organ metastasis, are also observed.
CASE 2
A young adult male neutered domestic shorthair cat was presented for evaluation due to lethargy and pain upon being picked up. The cat had an indoor/outdoor lifestyle and was up to date on vaccinations.
Physical examination
The patient demonstrated pain responses to palpation over all four limbs, and radiographs revealed multifocal lytic bone lesions, primarily affecting long bones.
Cytology
An aspirate of a lytic humeral lesion was obtained using a 20-gauge needle and syringe, and smears of the sample were prepared.
The slides were stained with Wright–Giemsa and examined cytologically. An inflammatory population was present and consisted of a mix of nondegenerate and mildly degenerate neutrophils, rounded and spindloid macrophages, and occasional multinucleated giant cells. Several macrophages contained rounded or oval fungal yeast, which ranged from approximately 2 to 4 microns wide (Figure 12.24). The yeast structures were surrounded by a thin area of clearing and contained a crescent-shaped or rounded basophilic nucleus. A few organisms were also observed free in the background blood. Low numbers of hematopoietic precursors were also noted, consistent with incidental sampling of bone marrow. 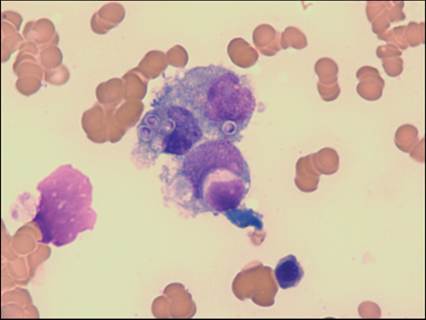
Figure 12.24 Cytology of the bone lesion revealed macrophages that contained fungal yeast (Wright–Giemsa, 1,000? magnification). (Courtesy Anne Barger.)
Diagnosis
The cytologic interpretation was pyogranulomatous inflammation with intralesional fungal yeast. The morphology was consistent with Histoplasma capsulatum.
Management/outcome
Due to a guarded prognosis, the owner declined further diagnostic testing (PCR) and treatment. The patient was humanely euthanized, and necropsy was not performed.
Discussion
A 2012 review of a group of 22 cats with histoplasmosis found that weakness (68%), weight loss (50%), and anorexia (45%) were the most common presenting complaints. Physical examination information was available for 20 of the cats, and only 4 had recorded lameness (Aulakh, 2012). Fielder et al. reviewed 25 cases of feline histoplasmosis with lameness or joint effusion and found bone lesions in 29 of 33 radiographs (88%) of carpi and tarsi. Diagnosis was made via cytology of one or more tissues in 22/25 cats (88%). Of cats for which serum ALP concentration was available (n = 18), no cat demonstrated an elevation in this value (Fielder et al., 2019). The Aulakh 2012 study assessed outcome and found that 12/22 cats (55%) survived to discharge; three died during the first week of treatment, and seven died or were euthanized without treatment.