Cases
CASE 1
Signalment/history
A 4-year-old, tortoiseshell domestic shorthair cat. Fully vaccinated; chronic sinusitis unresponsive to antimicrobial therapy; decreased appetite.
Physical examination
Swollen left maxillary sinus; unilateral, mucohemorrhagic discharge from the left nasal passage; inspiratory stridor; FeLV/FIV negative; urinalysis showed concentrated urine.
Computed tomography with contrast of the nasal passages
A CT scan showed a 24 ? 22 mm heterogeneously contrast enhancing mass, extending from the left nares caudally to the cribriform plate, eroding the ipsilateral orbital lamina, and invading the orbit ventrally and axially. There was diffuse homogeneous soft tissue opacification of the ipsilateral frontal and sphenoid sinuses as well as the entire nasopharynx (Figure 13.93). The opacification seen within the sinuses did not appear to be a direct extension from the mass itself.
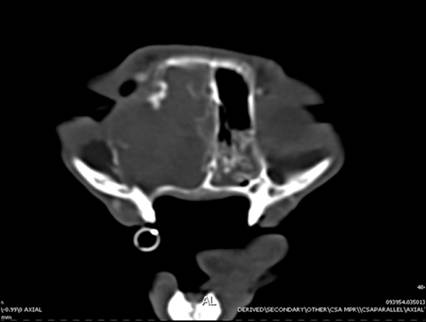
Figure 13.93 Nasal tumor. CT scan showing a mass in the left caudal nasal cavity, eroding the ipsilateral orbital lamina, and invading the orbit ventrally and axially. There was diffuse homogeneous soft tissue opacification of the entire nasopharynx.
Interpretation: suspected nasal adenocarcinoma with secondary obstructive sinusitis.
Cytology of the nasal mass
A sample of the nasal mass was obtained under general anesthesia through FNA biopsy. The smears were of good diagnostic quality with a high cellularity. There was a moderate blood admixture and many areas with a blue stippled background, consistent with necrosis. High numbers of epithelial cells arranged in papillary or occasionally acinar formations were seen. These cells had a medium to dark blue cytoplasm, often with poorly defined borders (Figure 13.94).
Nuclei were round to oval to slightly angular, with a coarse to clumped chromatin pattern and one to multiple prominent and often angular and giant nucleoli. A pronounced anisocytosis, variation in the N:C ratio, anisokaryosis, macronucleosis, nuclear molding, and occasional binucleation were present (Figure 13.95). Very high numbers of degenerate neutrophils and lesser numbers of activated macrophages, small and medium-sized lymphocytes, eosinophils, and plasma cells were seen. High numbers of bacteria were present in the background and phagocytized in the neutrophils. 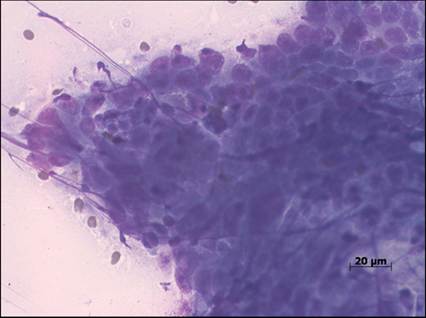
Figure 13.94 Nasal tumor. High numbers of epithelial cells arranged in sheets were seen. The cells had a medium to dark blue cytoplasm, often with poorly defined borders (Diff-Quik, 500? magnification).
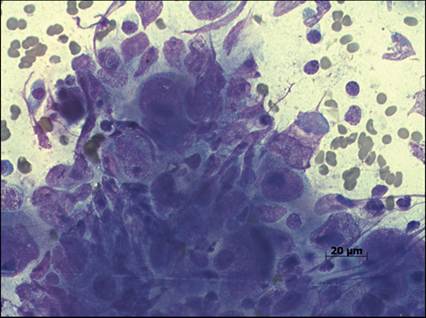
Figure 13.95 Nasal tumor. The nuclei of the neoplastic epithelial cells were round to oval to slightly angular, with a coarse to clumped chromatin pattern and one to multiple prominent and often angular and giant nucleoli. Marked anisocytosis, anisokaryosis, macronucleosis, nuclear molding, and occasional binucleation were present (Diff-Quik, 500? magnification).
Interpretation: adenocarcinoma with secondary septic neutrophilic inflammation.
Histopathology of the nasal mass
The sections examined revealed an intact nasal mucosal epithelium. The lamina propria contained extensive areas of tubule-like structures consisting of neoplastic epithelial cells. The neoplastic cells displayed inconspicuous cytoplasmic margins with a small to moderate amount of homogeneous, eosinophilic cytoplasm. The polygonal, pleomorphic neoplastic cells typically had round to oval nuclei, but there were occasional multinucleated, syncytial-like neoplastic cells. Nucleoli were frequently prominent and multiple, a few of which were macronucleoli and irregularly shaped (Figure 13.96).
The surrounding areas consisted of many lymphocytes and plasma cells with fewer macrophages, eosinophils, and neutrophils, with multifocal areas of hemorrhage and necrosis (Figure 13.97). The mitotic rate averaged 2–3 mitotic figures per high-power field. Interpretation: high-grade adenocarcinoma. 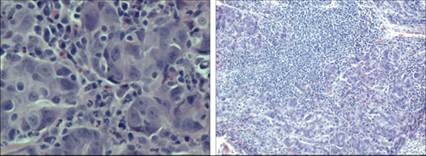
Figures 13.96,13.97 Nasal tumor. Histopathology of the mass revealed an intact nasal mucosal epithelium. The lamina propria contained extensive areas of tubule-like structures consisting of neoplastic epithelial cells. The cytoplasmic margins of the neoplastic cells were difficult to distinguish, and the cells had a small to moderate amount of homogeneous, eosinophilic cytoplasm. The polygonal, pleomorphic neoplastic cells typically had round to oval nuclei, with prominent and multiple nucleoli, a few of which were macronucleoli and irregularly shaped. The areas surrounding the neoplastic cells consisted of many lymphocytes and plasma cells with fewer macrophages, eosinophils, and neutrophils, with multifocal areas of hemorrhage and necrosis (H&E: 13.81, 500? magnification; 13.82, 50? magnification).
Follow up/outcome
The owners opted to perform radiation therapy; however, the patient developed severe complications due to the radiation therapy, and a decision was made to euthanize the cat.
Disease pathogenesis
Nasal adenocarcinoma is a malignant neoplasia of glandular cells of the nasal epithelium of dogs and cats. Adenocarcinomas are locally invasive neoplasms and rarely metastasize; occasionally, pulmonary metastasis can be found. Treatment of cats with adenocarcinoma consists of radiation therapy, which provides the most effective treatment at this time. Radiation therapy of the nasal structures can be complicated by cataracts of the eyes forming, blindness due to the radiation, and local skin reactions of the face, which include ulceration and inflammation.
CASE 2
Signalment/history
A 2-year-old, spayed female Dachshund. Chronic intermittent moist cough; referred for suspected cardiac disease.
Physical examination
No abnormalities detected. A mild sinus arrhythmia was present. No abnormal lung sounds were auscultated.
Thoracic radiographs
A standard right lateral thoracic view showed a mild diffuse broncho-interstitial pattern (Figure 13.98).
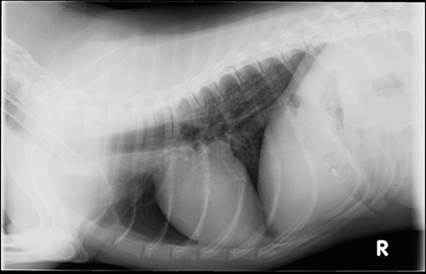
Figure 13.98 Eosinophilic inflammation. Right lateral view of the thoracic cavity showing a mild diffuse bronchointerstitial pattern.
Bronchoalveolar lavage cytology
The smears were of good diagnostic quality and high cellularity with good cell preservation. There was a moderate amount of blue, stringy mucus in the background. The majority of cells present were inflammatory cells, with the population consisting of 59% eosinophils; 27% neutrophils, nondegenerate; 8% small lymphocytes; 6% macrophages, occasionally reactive with cytoplasmic vacuolization (Figure 13.99). Ciliated epithelial cells were present in moderate numbers and squamous epithelial cells were very occasionally seen.
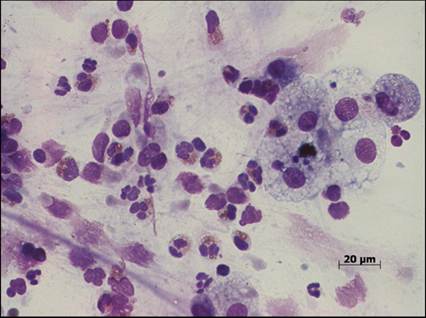
Figure 13.99 Eosinophilic inflammation. Smears from the bronchoalveolar lavage with high cellularity and a moderate amount of blue, stringy mucus in the background. The majority of nucleated cells present were inflammatory cells, predominated by eosinophils with fewer neutrophils and vacuolated macrophages (Diff-Quik, 500? magnification).

Figure 13.100 Metastatic lung tumor. Left lateral and dorsoventral radiographs of the thoracic cavity showing two well-marginated, round homogeneous soft tissue nodules. The stomach was moderately distended with gas with lobulated soft tissue opacities noted along the lesser curvature.
Interpretation: eosinophilic inflammation. Differential diagnoses: eosinophilic bronchopneumopathy secondary to a hypersensitivity reaction or parasites.
Follow up
The patient was started on an immunosuppressive dose of corticosteroids, tapered over several weeks. The coughing stopped soon after treatment was initiated.
Disease pathogenesis
Eosinophilic bronchopneumopathy (previously known as pulmonary infiltrates with eosinophils) is a condition that most commonly affects young adult dogs. Females are more frequently affected than males. The most common clinical sign is a harsh cough followed by gagging and retching. The cause of this condition is infiltration of eosinophils into the lungs. Causes of this infiltration of eosinophils can be parasites in the lungs or a hypersensitivity to inhaled allergens. Although peripheral eosinophilia is identified in 50–60% of cases, absence of eosinophilia (as was seen in this case) does not rule the condition out (Clercx et al., 2000; Clercx & Peeters, 2007a). The prognosis is good, and an excellent response is usually seen with corticosteroid treatment. Corticosteroid treatment can often be stopped completely without recurrence of coughing, but it is important to note that a relapse might occur, which will require another course of treatment. In some patients, chronic use of very low dose corticosteroid (e.g. every other day) might be needed.
CASE 3
Signalment/history
A 10-year-old, spayed female Bernese Mountain dog. Anorexia, depression, lethargy.
Physical examination
Mild pyrexia; muffled heart sounds; mild hypoglycemia.
Thoracic radiography
Standard right and left lateral, as well as dorsoventral radiographs were taken. Two well-marginated, round homogeneous soft tissue nodules were noted. The stomach was moderately distended with gas, with lobulated soft tissue opacities noted along the lesser curvature of the stomach (Figures 13.100, 13.101).
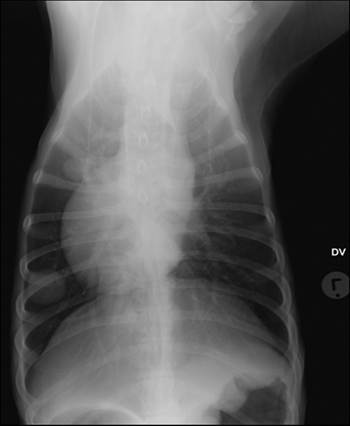
Figure 13.101 Metastatic lung tumor.
Left lateral and dorsoventral radiographs of the thoracic cavity showing two well-marginated, round homogeneous soft tissue nodules. The stomach was moderately distended with gas with lobulated soft tissue opacities noted along the lesser curvature.
Interpretation: suspected primary (with metastatic) or metastatic lung disease. Neoplasia should also be considered for the gastric lesion.
Abdominal ultrasonography
The gastric fundus wall was focally markedly thickened by up to 2 cm with a diffuse hypoechoic appearance devoid of wall layering. The liver appeared to be normal size but was mild-to-moderately diffusely hypoechoic. The spleen was generous and mildly diffusely hyperechoic. All of the abdominal lymph nodes appeared to be mildly enlarged. There was also a small amount of anechoic free peritoneal fluid noted in the recesses.
Interpretation: suspected gastric adenocarcinoma.
Cytologic examination
Abdominal fluid
The smears were of moderate cellularity and cell preservation was good. There was a moderate blood admixture; moderate numbers of neutrophils and lesser numbers of macrophages and lymphocytes as well as occasional reactive mesothelial cells were present. Moderate numbers of medium to large cells with a medium blue cytoplasm, often with small clear vacuoles, were seen. These cells were present either singly or in small clusters or balls. Nuclei were round to oval with a coarse chromatin pattern and one to multiple small nucleoli. The cell population displayed an anisocytosis, anisokaryosis, increase in N:C variation, multinucleation, nuclear molding, and very occasional irregular mitoses (Figure 13.102).
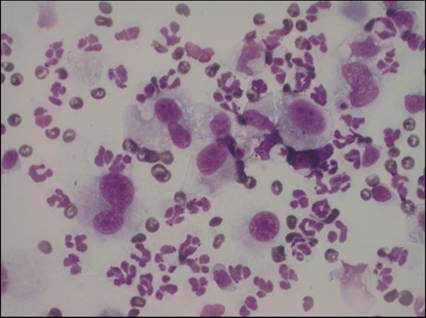
Figure 13.102 Metastatic lung tumor. Abdominal fluid containing moderate numbers of medium to large cells with a medium blue cytoplasm, often with small clear vacuoles. The cells were present either singly or in small clusters. This cell population displayed an anisocytosis, anisokaryosis, increase in nuclear:cytoplasm variation, multinucleation, nuclear molding, very occasional irregular mitoses, round to oval nuclei with a coarse chromatin pattern, and one to multiple small nucleoli (Diff-Quik, 500? magnification).
Interpretation: neoplastic effusion.
Gastric wall
One smear of low cellularity with poor cell preservation was examined. There was a marked blood admixture and many platelet clumps containing low numbers of neutrophils were present. Very low numbers of neutrophils and small lymphocytes were present in the bloody background. Very low numbers of discrete cells with a light blue, sometimes finely vacuolated cytoplasm and round to angular nucleus with a coarse chromatin pattern were seen (Figure 13.103). One cell with a small satellite nucleus was noted.
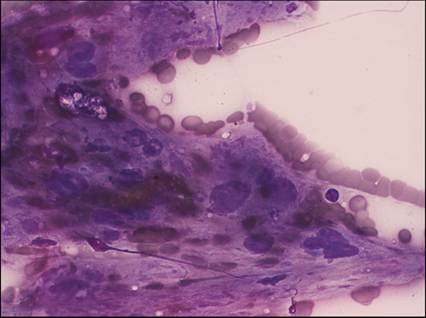
Figure 13.103 Metastatic lung tumor. The FNA sample of the lesion in the gastric mucosa had a marked blood admixture with low cellularity. Very low numbers of neutrophils and small lymphocytes were present in the bloody background, as well as low numbers of discrete cells with a light blue, sometimes finely vacuolated cytoplasm and round to angular nucleus with a coarse chromatin pattern (Diff-Quik, 500? magnification).
Interpretation: peripheral blood and low numbers of atypical cells. Further interpretation was limited due to the low cellularity and poor cell preservation. No normal gastric epithelial cells were seen.
Liver
The smears were of very low cellularity with a severe blood admixture. Occasional hepatocytes in small clusters with a stippled cytoplasm were seen. A few discrete cells with abundant basophilic, sometimes finely vacuolated cytoplasm and round to angular nucleus with a coarse chromatin pattern were seen (Figure 13.104). Low numbers of neutrophils, macrophages, and lymphocytes were also present, especially along the edges of the smears.
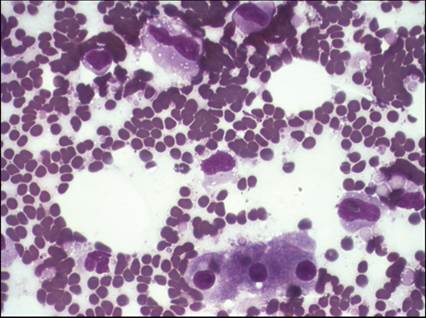
Figure 13.104 Metastatic lung tumor. The smears from the liver were of very low cellularity with a marked blood admixture. Hepatocytes were seen in small clusters. Few discrete cells with abundant basophilic, sometimes finely vacuolated cytoplasm and round to angular nucleus with a coarse chromatin pattern were seen (Diff-Quik, 500? magnification).
Interpretation: peripheral blood with very low numbers of hepatocytes and neoplastic metastasis.
Lung
The smears were of good diagnostic quality and high cellularity with good cell preservation. There was a moderate blood admixture. There were high numbers of epithelial cells arranged in acinar formations (Figure 13.105). These cells were oval to columnar to spindle-shaped with a medium blue cytoplasm, often with numerous small clear vacuoles (Figure 13.106). Nuclei were round to oval with a coarse chromatin pattern and one to two, small, occasionally angular nucleoli. A light pink material was often seen between the cells. Anisocytosis, anisokaryosis, multinucleation, and nuclear molding were present (Figure 13.107). Low numbers of neutrophils and macrophages were also seen.
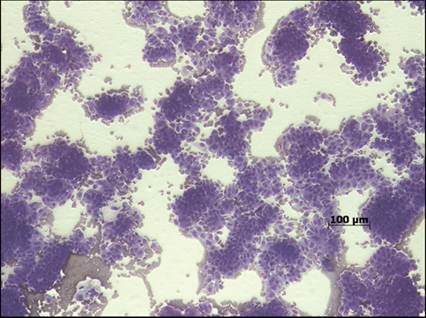
Figure 13.105 Metastatic lung tumor. The aspiration samples of the lung masses showed a moderate blood admixture with high numbers of epithelial cells arranged in acinar formations (Diff-Quik, 100? magnification).
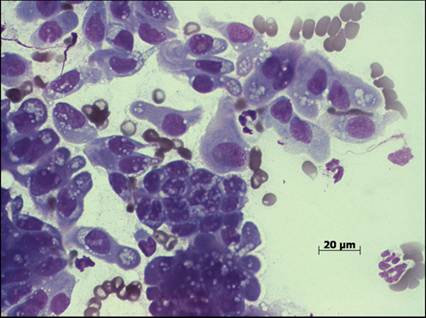
Figure 13.106 Metastatic lung tumor. The epithelial cells from the lung masses were oval to columnar to spindle-shaped with a medium blue cytoplasm, often with numerous small clear vacuoles (Diff-Quik, 500? magnification).
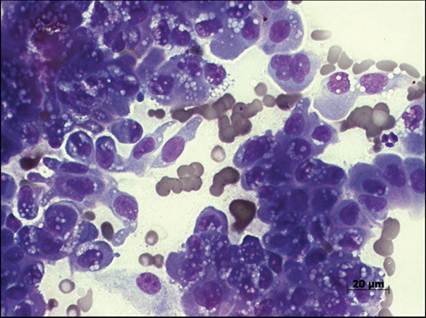
Figure 13.107 Metastatic lung tumor. The neoplastic epithelial cells from the lung mass had round to oval nuclei with a coarse chromatin pattern and one to two, small, occasionally angular nucleoli. Anisocytosis, anisokaryosis, multinucleation, and nuclear molding were present (Diff-Quik, 500? magnification).
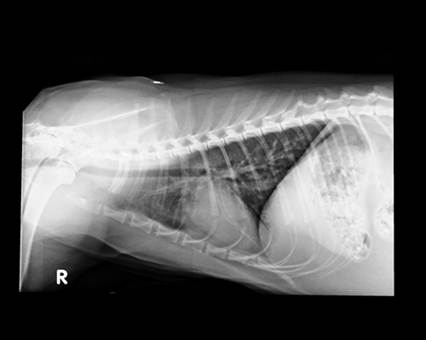
Figure 13.108 Feline asthma. Right lateral and dorsoventral radiographic views of the thoracic cavity showing a diffuse bronchointerstitial lung pattern.
Interpretation: metastatic adenocarcinoma.
Follow up/outcome
Due to the poor prognosis of the condition, the owners opted for euthanasia.
Disease pathogenesis
The pulmonary vascular bed receives a lot of blood coming from the right heart with each cardiac cycle. The lung serves as an ideal location for metastatic disease due to the numerous, well-oxygenated capillary beds through which the blood passes. Cancer cells detach from the primary tumor, enter the blood or lymphatics to be carried to distant sites, migrate from the vessel into the tissue, adhere, and then grow in the new site. Almost all neoplasms can metastasize to the lung but some are more likely to do so, such as oral and nail bed melanoma, thyroid carcinoma, osteosarcoma, and mammary carcinoma.
CASE 4
Signalment/history
A 1.5-year-old, sterilized female, Norwegian Forest cat. Fully vaccinated and presented with a history of chronic coughing and wheezing of two months’ duration.
Physical examination and minimum database
Bright and alert and normal temperature, heart rate, and respiratory rate. No abnormalities on thoracic auscultation. Mild stress leukogram noted on hematology, mild pre-renal azotemia, and mild hyperalbuminemia due to dehydration.
Thoracic radiography
Standard right and left lateral, as well as dorsoventral radiographs were taken. A broncho-interstitial lung pattern was evident (Figures 13.108, 13.109).

Figure 13.109 Feline asthma. Right lateral and dorsoventral radiographic views of the thoracic cavity showing a diffuse bronchointerstitial lung pattern.
Cytology of the BAL fluid
A large amount of mucoid material was noted on bronchoscopy and submitted for cytologic evailation. The material was very cellular (many clusters of cells, 40–50 cells/50? HPF). There was a mild blood admixture, and the background was highly mucinous (pink granular to fibrillar material with some light blue amorphous material) with some necrosis (degenerate unidentifiable cells). Leukocytes were seen in moderate to high numbers and included 13.5% neutrophils (mostly degenerate), 9% small mononuclear cells (mostly lymphocytes), 16.5% large mononuclear cells (mostly activated macrophages), and 61% eosinophils (Figure 13.110). High numbers of ciliated columnar epithelia cells were present and had medium blue cytoplasm that was sometimes vacuolated, basal oval nuclei with coarse chromatin, and multiple prominent nuclei (Figure 13.111). They showed mild to moderate anisokaryosis and binucleation. No microorganisms were seen.
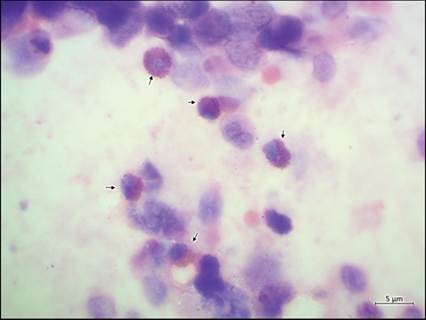
Figure 13.110 Feline asthma. Bronchoalveolar lavage smear. An increased proportion of eosinophils (arrows) were noted in a moderately mucinous background with a low proportion of ruptured and/or degenerate appearing respiratory epithelial cells (Wright–Giemsa, 1,000? magnification).
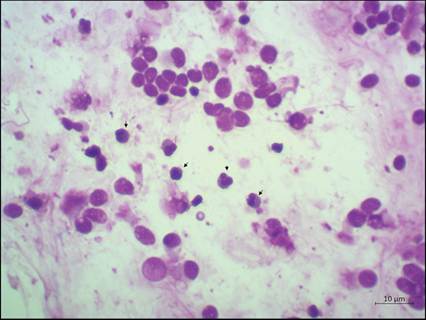
Figure 13.111 Feline asthma. Bronchoalveolar lavage smear. An increased proportion of eosinophils (arrows) were noted in a moderately mucinous background with a low proportion of ruptured and/or degenerate appearing respiratory epithelial cells (Wright–Giemsa, 500? magnification).
Interpretation: eosinophilic inflammation with moderate respiratory epithelial hyperplasia and mild necrosis. The epithelial hyperplasia and necrosis were likely due to chronic respiratory inflammation. The presence of copious numbers of respiratory epithelial cells indicates that the sample comes, at least in part, from the upper airways. Eosinophilic inflammation was most likely due to allergic bronchitis/feline asthma, especially given the age of the patient; however, eosinophilic granuloma and parasitic or bacterial infection couldn’t be ruled out on cytology.
For the aerobic culture and antimicrobial susceptibility testing of the bronchoalveolar lavage fluid, no growth was noted after 72 hours of incubation.
Follow up/outcome
The patient was diagnosed with feline allergic asthma. The treatment plan included a tapering dosage of oral glucocorticoids and concurrent, chronic inhalant glucocorticoid therapy. A bronchodilator inhaler, deworming, topical parasiticides, and a hypoallergenic diet were also included. The patient responded very well to medication, with no clinical symptoms noted by owners during subsequent follow-up visits.
Disease pathogenesis
Feline asthma is a common lower-airway inflammatory disease in cats affecting approximately 1–5% of the feline population and is thought to be allergic in origin. Generally, clinicopathologic abnormalities of cats with asthma are nonspecific. Common radiographic findings in asthmatic cats include a bronchial or bronchointerstitial lung pattern. Bronchoalveolar lavage fluid sample for cytologic examination can be collected using either bronchoscopy or a blind technique. Eosinophilic inflammation is noted on BAL fluid cytology of asthmatic cats. Adjunctive testing includes culture of the BAL fluid, allergy testing, pulmonary function testing, and biomarkers, for example endothelion-1. The condition is mostly treated with glucocorticoids and bronchodilators. These are effective treatments in many cats; however, some are unresponsive or minimally responsive. Therapies that might help reverse the underlying immunopathology of asthma or could be used as adjuncts in refractory asthma are being investigated in experimental feline asthma models and include allergy-specific immunotherapy, omega-3 fatty acids/nutraceuticals, inhaled lidocaine, tyrosine kinase inhibitors, and stem cells (Trzil, 2020).
CASE 5
Signalment/history
A 3-year-old, intact female, bull terrier. Progressive lethargy, weakness, anorexia, and weight loss were noted in the few weeks prior to presentation. Owners also noted difficulty in breathing, intermittent foaming at the mouth, and a dry cough.
Physical examination and minimum database
The patient was collapsed on presentation, with a poor body condition, and she displayed dyspnea and tachypnea that was characterized by abdominal breathing and abducted elbows. Referred and increased breath sounds were auscultated in all the lung quadrants with increased intensity in the right thoracic area. Hematology revealed a mild stress leukogram and pseudothrombocytopenia due to platelet aggregation and mild hypernatremia on serum biochemistry.
Thoracic radiography
Standard right and left lateral, as well as dorsoventral radiographs were taken. A severe, diffuse broncho-interstitial lung pattern involving all the lung lobes was evident (Figures 13.112–13.114).

Figure 13.112 Pulmonary neoplasia (carcinoma). Right and left lateral and dorsoventral radiographic views of the thoracic cavity showing a diffuse bronchointerstitial lung pattern.
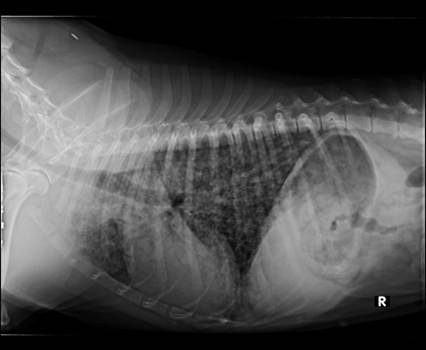
Figure 13.113 Pulmonary neoplasia (carcinoma). Right and left lateral and dorsoventral radiographic views of the thoracic cavity showing a diffuse bronchointerstitial lung pattern.

Figure 13.114 Pulmonary neoplasia (carcinoma). Right and left lateral and dorsoventral radiographic views of the thoracic cavity showing a diffuse bronchointerstitial lung pattern.
Cytology of the BAL
The material was turbid and flocculent and the automated total nucleated cell count was 2,260 cells/μl. The material was moderate cellularity (2 cells/50? HPF). Moderate amounts of mucus were noted in the background. The nucleated cell count consisted of 83% degenerate neutrophils, 5% lymphoid cells, and 12% macrophages. The macrophages were activated, with vacuolated cytoplasm. In addition, moderate numbers of epithelial cells arranged in tightly cohesive clusters were present (Figure 13.115). These cells were medium sized, round, and had round to oval centrally placed nuclei. The cells displayed intense cytoplasmic basophilia, high N:C ratio, moderate anisocytosis/anisokaryosis, and prominent nucleoli. Occasional multinucleation, with nuclear molding, was also seen (Figure 13.116).
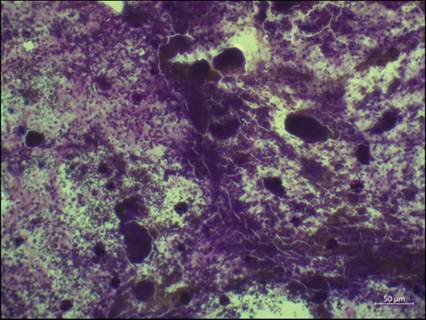
Figure 13.115 Bronchoalveolar lavage smear. Cellular and thick sample with a mild blood admixture and high numbers of tightly cohesive variably sized clusters of epithelial cells and moderate numbers of leukocytes in the background (Wright–Giemsa, 100? magnification).
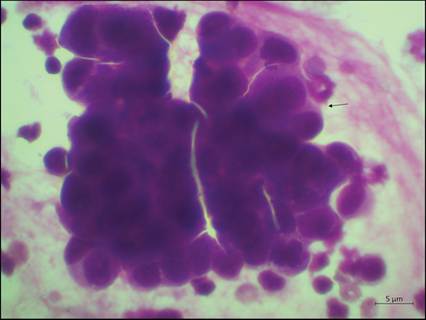
Figure 13.116 Bronchoalveolar lavage smear. A cluster of epithelial cells displaying increased cytoplasmic basophilia, moderate anisocytosis, anisokaryosis, coarse chromatin, multiple nucleoli, bi- and multinucleation with nuclear molding (arrow) (Wright–Giemsa, 1,000? magnification).
Interpretation: highly suggestive of a carcinoma, with secondary neutrophilic inflammation, and peripheral blood admixture. Histopathology was advised for definitive diagnosis.
Outcome
Due to the poor prognosis the owners opted for humane euthanasia. A diagnosis of severe, diffuse primary pulmonary bronchial carcinoma with metastasis to the regional lymph nodes was made on post-mortem examination.
Disease pathogenesis
Carcinomas comprise 80% or more of all primary lung tumors in dogs and cats (Hahn et al., 1996; Moulton et al., 1981). Pulmonary epithelial tumors are less common in dogs than in cats, affecting the cranial and caudal lung lobes more equally and often presenting as a single mass. These are often histologic classified as bronchioalveolar, adenocarcinoma, or anaplastic carcinoma; however cytologic differentiation isn’t possible (Barrett et al., 2014; Marolf et al., 2011; Burgess & Kerr, 2009). Furthermore, the cytologic preparations from primary and metastatic carcinomas are similar, and the two cannot be definitively differentiated by cytologic evaluation alone. Metastasis of pulmonary carcinomas is less common in dogs compared to cats and a better prognosis is associated with evidence of cell differentiation and the absence of clinical signs (McNiel et al., 1997).