Cytologic interpretation
Inflammation
Inflammation of the lung parenchyma appears very similar to that seen in other tissue, with neutrophils being the predominant cell type. Typical causes include bacterial infection, neoplasia, necrosis, presence of foreign material, and other noninfectious causes.
Necrotic debris is often aspirated and appears as amorphous, bluish-gray to pink material that may be scattered throughout the smear or concentrated in certain dense aggregates (Figures 13.70, 13.71). Foreign material may sometimes be observed surrounded by aggregates of inflammatory cells. Increased numbers of alveolar macrophages (Figure 13.72) may be seen with both acute and chronic inflammatory disorders such as necrosis, atelectasis, lung lobe torsion, hemorrhage, neoplasia, and pneumonia due to foreign material. An increased number of epithelioid macrophages, together with multinucleated giant cell macrophages, is termed granulomatous inflammation. Epithelioid macrophages are plump, round with well-defined cytoplasmic borders and blue–gray to pale pink cytoplasm. Granulomatous inflammation is most commonly associated with certain infectious agents, including fungi, protozoa, mycobacteria, other bacteria such as Nocardia spp., or foreign bodies (Grimes et al., 2014). 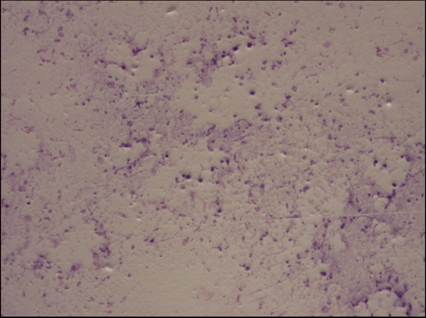
Figure 13.70 Necrosis. A sample taken from the necrotic center of a lung lesion can appear as amorphous, bluish-gray to pink material that may be scattered throughout the smear or concentrated in certain dense aggregates (Diff-Quik: 100? magnification).
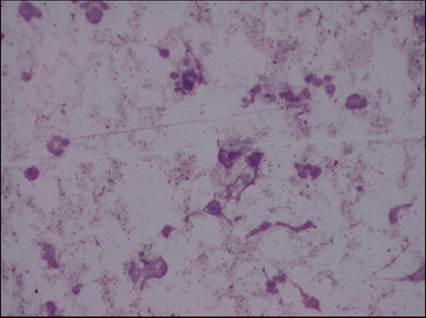
Figure 13.71 Necrosis. A sample taken from the necrotic center of a lung lesion can appear as amorphous, bluish-gray to pink material that may be scattered throughout the smear or concentrated in certain dense aggregates (Diff-Quik: 500? magnification).
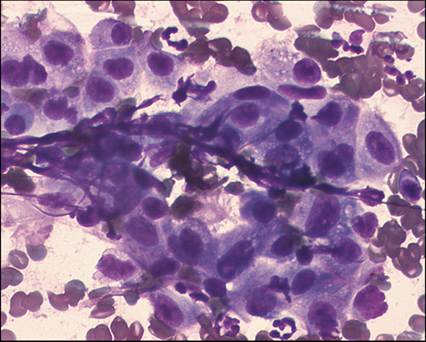
Figure 13.72 Alveolar macrophages. An increased number of alveolar macrophages may be seen with both acute and chronic inflammatory disorders. Similar to macrophages seen in bronchoalveolar washes, they have abundant blue–gray cytoplasm and an eccentrically positioned, round to bean-shaped nucleus (Diff-Quik, 500? magnification).
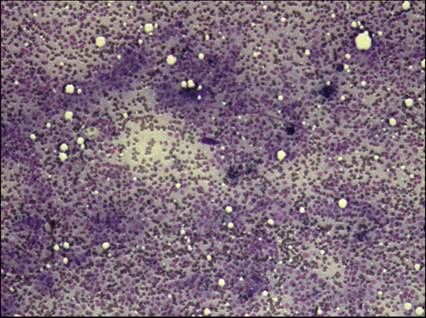
Figure 13.73 Neoplasia. The most common primary tumors of the lung in dogs and cats are epithelial tumors, such as adenocarcinoma, showing typical cell-to-cell adhesion (Diff-Quik, 100? magnification).
Hypersensitivity
A hypersensitivity response or eosinophilic inflammation is present when eosinophils are >10% of the nucleated cell count, especially in the absence of a peripheral eosinophilia. Variable numbers of other leukocytes such as macrophages, neutrophils, and mast cells may also be seen. Causes include allergic or hypersensitivity disorders, eosinophilic bronchopneumopathy, parasite infestation, and some fungal, bacterial, and neoplastic diseases (Clercx et al., 2000; Clercx & Peeters, 2007a; Grimes et al., 2014).
Neoplasia
One of the more important reasons for performing a lung FNA biopsy is to diagnose primary and metastatic pulmonary neoplasia, since neoplastic cells are rarely seen in samples from TTW/BAL unless the tumor has eroded through the bronchial tree. Ultrasound-guided FNA biopsy of focal parenchymal lesions of the lung has been shown to be a very effective tool, with a sensitivity of up to 88% and minimal false-positive diagnoses of neoplasia (McMillan et al., 1988; Wood et al., 1998b). The most common primary tumors of the lung in dogs and cats are epithelial tumors (Ogilvie et al., 1989). Adenocarcinomas of bronchogenic or bronchiolar–alveolar origin are the most common neoplasms of the lung; however, cytologic differentiation is usually not possible (Figures 13.73, 13.74).
In addition, differentiating a primary from a metastatic epithelial tumor in the lung is also difficult. Common tumors to metastasize to the lungs include oral and nail bed melanoma, thyroid carcinoma, osteosarcoma, mammary carcinoma, and high-grade soft tissue sarcoma (Ogilvie et al., 1989). Aspirates of lung carcinomas typically yield highly cellular smears that consist of epithelial cells arranged as cohesive clusters (Figure 13.75, 13.76) or 3-dimensional balls (Figures 13.77, 13.78), with lesser numbers of individualized cells. Care should be taken not to confuse these individualized cells with discrete cell tumors. Acinar formation indicates glandular origin, suggesting an adenocarcinoma (Figure 13.79). Moderate to marked pleomorphism between cells within the same cluster (Figures 13.80, 13.81), as well as between clumps of cells, is common in pulmonary carcinoma. The neoplastic epithelial cells appear as round to polygonal, basophilic cells displaying various cellular criteria of malignancy including eccentrically placed nuclei with coarsely clumped chromatin and prominent, single to multiple nucleoli; anisokaryosis; and deeply basophilic cytoplasm (Figures 13.82–13.84). Cytoplasmic vacuolation, particularly around the perinuclear region, is frequently prominent (Figure 13.85). Other criteria of malignancy may be seen and include nuclear molding, signet ring cell formation (Figures 13.86, 13.87), nuclear gigantism, and bi- or multinucleated cells (Figure 13.88, 13.89). Necrotic material, with or without inflammation, is also commonly associated with neoplasia. Dysplastic or metaplastic changes to the pulmonary epithelial cells secondary to inflammation can complicate the diagnosis, and histopathologic examination is required to differentiate. Hemolymphatic neoplasia, such as lymphoma and malignant histiocytosis, has been reported to disseminate throughout the lung parenchyma, resulting in diffuse infiltrative disease (Geyer et al., 2010). Canine histiocytic malignancies are aggressive tumors that occur with high frequency in Bernese Mountain dogs and flat-coated Retrievers and have been described in the lung parenchyma. Cytologic findings included numerous pleomorphic, large, discrete mononuclear cells with abundant, lightly basophilic, vacuolated, cytoplasm. Nuclei are round to oval to reniform with marked anisokaryosis, and nucleoli are prominent. Multinucleated giant cells are frequently observed (Figures 13.90–13.92) (Brown et al., 1994). A diagnosis of presumptive primary pulmonary mast cell tumor has been described in two dogs, neither of which had a previous history of cutaneous mast cell tumor. Both dogs were presented with a massive solitary pulmonary mast cell tumor (Campbell et al., 2017). 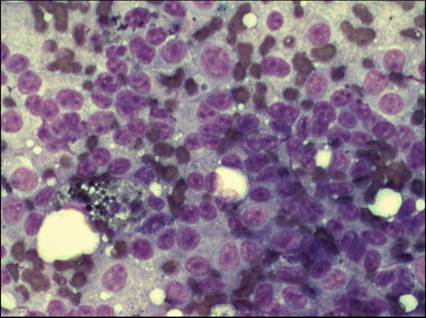
Figure 13.74 Neoplasia. The most common primary tumors of the lung in dogs and cats are epithelial tumors, such as adenocarcinoma, showing typical cell-to-cell adhesion (Diff-Quik, 500? magnification).
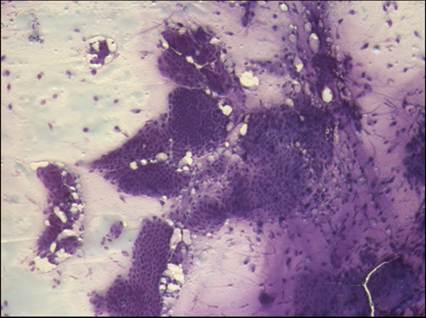
Figure 13.75 Neoplasia. Aspirates of lung carcinomas typically yield highly cellular smears that consist of epithelial cells arranged as cohesive clusters (Diff-Quik, 100? magnification) or three-dimensional balls, with lesser numbers of individualized cells.
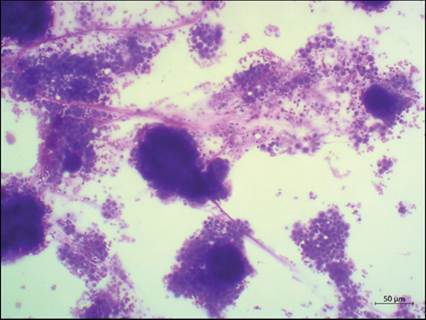
Figure 13.76 Neoplasia. Aspirates of lung carcinomas typically yield highly cellular smears that consist of epithelial cells arranged as cohesive clusters (Wright–Giemsa, 100? magnification) or three-dimensional balls, with lesser numbers of individualized cells.
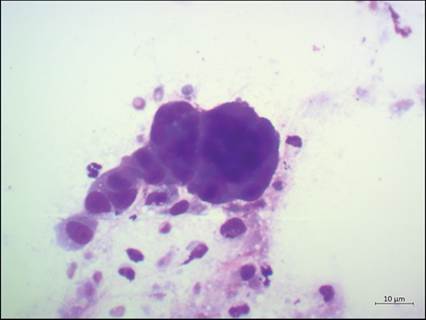
Figure 13.77 Neoplasia. Aspirates of lung carcinomas typically yield highly cellular smears that consist of epithelial cells arranged as cohesive clusters or three-dimensional balls (Wright–Giemsa, 500? magnification), with lesser numbers of individualized cells.
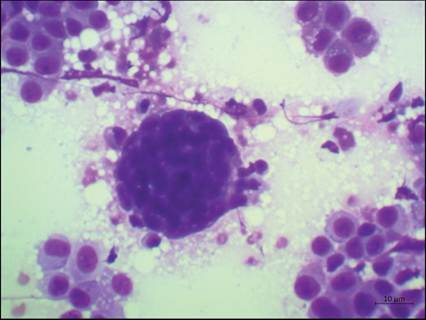
Figure 13.78 Neoplasia. Aspirates of lung carcinomas typically yield highly cellular smears that consist of epithelial cells arranged as cohesive clusters or three-dimensional balls (Wright–Giemsa, 500? magnification), with lesser numbers of individualized cells.
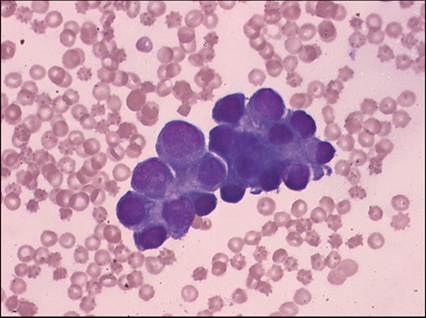
Figure 13.79 Neoplasia. Acinar formation, a cluster of cells that resembles a many-lobed berry, is an indication that the tumor is of glandular origin, suggesting an adenocarcinoma (Diff-Quik, 500? magnification).
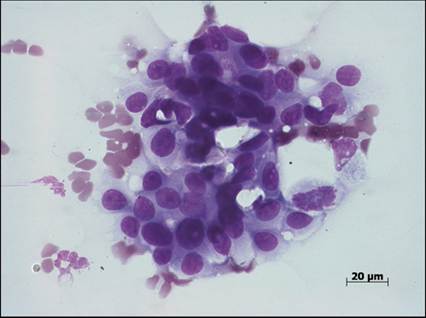
Figure 13.80 Neoplasia. Moderate to marked pleomorphism between cells can be seen within the same cluster of neoplastic epithelial cells sampled from a nodule in the lung (Diff-Quik, 500? magnification for both).
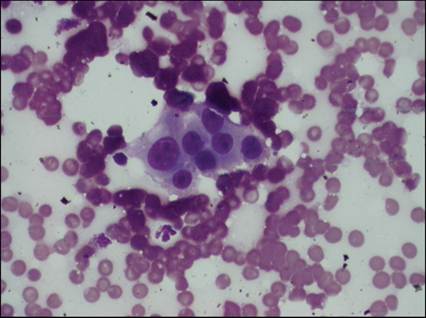
Figure 13.81 Neoplasia. Moderate to marked pleomorphism between cells can be seen within the same cluster of neoplastic epithelial cells sampled from a nodule in the lung (Diff-Quik, 500? magnification for both).
alt=fig13.82.jpg>
Figure 13.82 Neoplasia. Neoplastic pulmonary epithelial cells appear as round, basophilic cells displaying various malignant criteria such as eccentrically placed nuclei with coarsely clumped chromatin and prominent, single to multiple nucleoli, some with angular shapes; anisokaryosis; multinucleation, some with odd numbers of nuclei per cell, and deeply basophilic cytoplasm (Diff-Quik, 500? magnification).
During fluid accumulation in the pleural cavity, the pleural mesothelial cells undergo hypertrophy and hyperplasia, and individual cells exfoliate into the fluid. Cytologic differentiation between these reactive or dysplastic mesothelial cells and carcinoma cells can therefore be difficult.
Reactive mesothelial cells can have morphologic features resembling malignancy, especially when they are arranged in large clusters. If present, acinar formation may support a diagnosis of carcinoma or malignant mesothelioma (Hirschberger et al., 1999). 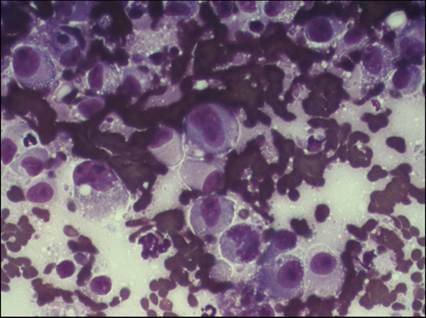
Figure 13.83 Neoplasia. Neoplastic pulmonary epithelial cells appear as round, basophilic cells displaying various malignant criteria such as eccentrically placed nuclei with coarsely clumped chromatin and prominent, single to multiple nucleoli, some with angular shapes; anisokaryosis; multinucleation, some with odd numbers of nuclei per cell, and deeply basophilic cytoplasm (Diff-Quik, 500? magnification).
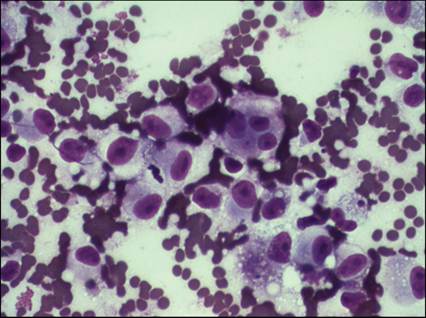
Figure 13.84 Neoplasia. Neoplastic pulmonary epithelial cells appear as round, basophilic cells displaying various malignant criteria such as eccentrically placed nuclei with coarsely clumped chromatin and prominent, single to multiple nucleoli, some with angular shapes; anisokaryosis; multinucleation, some with odd numbers of nuclei per cell, and deeply basophilic cytoplasm (Diff-Quik, 500? magnification).
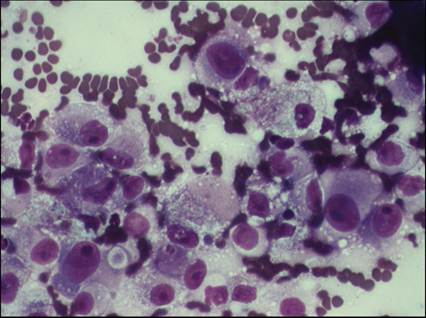
Figure 13.85 Neoplasia. Epithelial cells with cytoplasmic vacuolation, particularly around the perinuclear region, are frequently prominent in pulmonary neoplasia (Diff-Quik, 500? magnification).
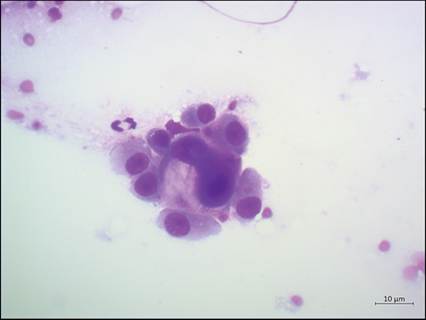
Figure 13.86 Neoplasia. Neoplastic pulmonary epithelial cells displaying malignant criteria such as nuclear molding, signet ring cell formation, nuclear gigantism, and multinucleation (Wright–Giemsa, 500? magnification).
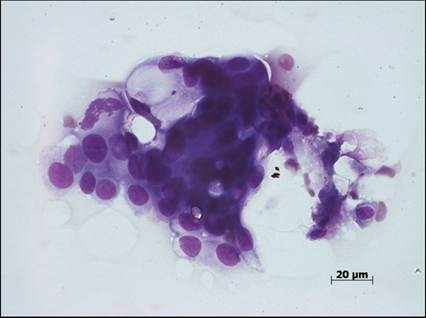
Figure 13.87 Neoplasia. Neoplastic pulmonary epithelial cells displaying malignant criteria such as nuclear molding, signet ring cell formation, nuclear gigantism, and multinucleation (Diff-Quik, 500? magnification).
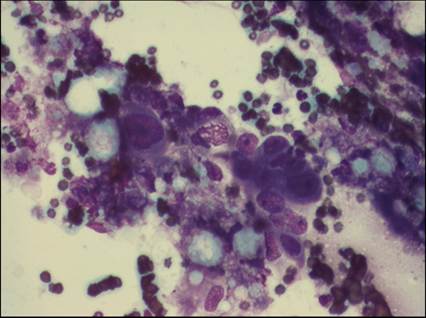
Figure 13.88 Neoplasia. Neoplastic pulmonary epithelial cells displaying malignant criteria such as nuclear molding, signet ring cell formation, nuclear gigantism, and multinucleation (Diff-Quik, 500? magnification).
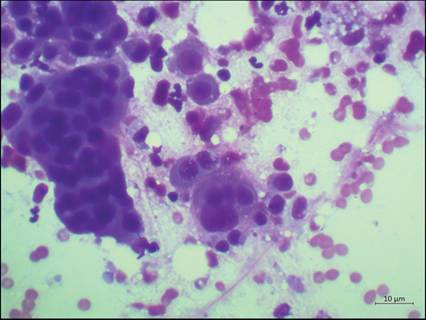
Figure 13.89 Neoplasia. Neoplastic pulmonary epithelial cells displaying malignant criteria such as nuclear molding, signet ring cell formation, nuclear gigantism, and multinucleation (Wright–Giemsa, 500? magnification).
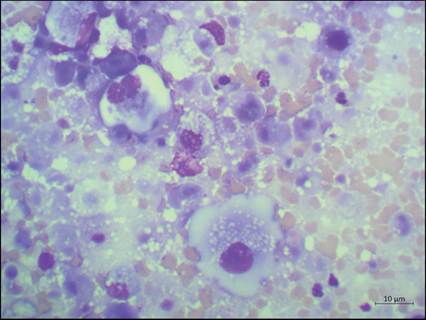
Figure 13.90 Neoplasia. Malignant histiocytic cells displaying marked pleomorphism, with abundant, lightly basophilic, vacuolated, cytoplasm. Nuclei are round to oval to reniform with marked anisokaryosis, and nucleoli are prominent. Multinucleated giant cells are frequently observed (Wright–Giemsa, 500? magnification).
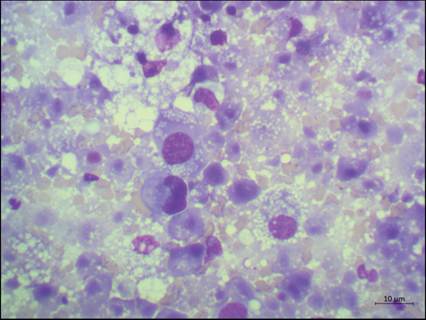
Figure 13.91 Neoplasia. Malignant histiocytic cells displaying marked pleomorphism, with abundant, lightly basophilic, vacuolated, cytoplasm. Nuclei are round to oval to reniform with marked anisokaryosis, and nucleoli are prominent. Multinucleated giant cells are frequently observed (Wright–Giemsa, 500? magnification).
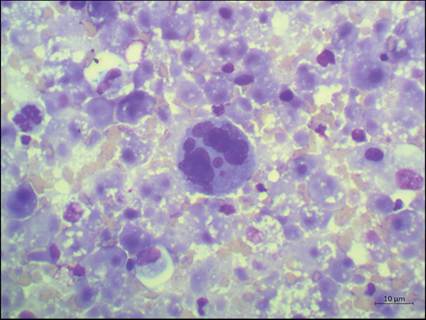
Figure 13.92 Neoplasia. Malignant histiocytic cells displaying marked pleomorphism, with abundant, lightly basophilic, vacuolated, cytoplasm. Nuclei are round to oval to reniform with marked anisokaryosis, and nucleoli are prominent. Multinucleated giant cells are frequently observed (Wright–Giemsa, 500? magnification).