Lung parenchyma
Collection techniques and sample preparation
Intrathoracic FNA biopsy of the lung parenchyma may result in the cytologic diagnosis of inflammatory conditions, neoplasia, and infectious agents.
Limitations of FNA biopsy cytopathology include poor cellular yield, especially for certain cell types (e.g. mesenchymal cells), necrosis, failure to obtain a representative sample, and its inability to provide information regarding architectural changes (DeBerry et al., 2002a). Although complications may occur, it is generally considered a safe procedure. The procedure is performed using a 22-gauge needle (20–25 gauge) of variable length (depending on the depth and size of the lesion). A 5–12 ml syringe should be attached to the needle, either directly or via an extension tube. The use of an imaging modality such as thoracic radiographs, fluoroscopy, ultrasonography, or CT is strongly advised in order to obtain a representative sample of the lesion. Blind aspiration may, however, be attempted with diffuse, infiltrative pulmonary disease. The right caudal lung lobe is usually sampled with diffuse disease and the standard sampling site is the 7th to 9th intercostal space, one-third of the distance from the spinal column to the costochondral junction. If the chest is entered too far caudally, the liver can be accidentally aspirated. Hemostatic screening should preferably be performed before the procedure and should include a platelet count and other routine hemostatic assays. The procedure can either be performed with sedation only or under general anesthesia, depending on the clinical status of the patient. The hair over the sampling site should be clipped and the area prepared aseptically. Samples can be obtained using aspiration or nonaspiration techniques. Once the sample is in the bore of the needle it should be transferred efficiently to the surface of a clean slide. To create a monolayer of cells the ‘squash’ preparation technique can be used (described above under ‘Nasal Cavity’). If the material is very bloody, a normal blood smear preparation technique should be used. Possible complications for the procedure include pneumothorax and hemorrhage, both mild and self-limiting, and needle tract implantation, which is rare (Rakich & Latimer, 1989b; Teske et al., 1991; Wood et al., 1998b; Warren-Smith et al., 2011). Contraindications for the procedure include bleeding disorders, bullous emphysema, uncooperative patient, severe uncontrolled coughing, and pulmonary hypertension (Rakich & Latimer, 1989b; Wood et al., 1998b). Agreement of 82–89% between percutaneous FNA biopsy cytopathology and histopathology has been reported for dogs and cats (DeBerry et al., 2002a; Bonfanti et al., 2004).Normal cytologic features
Samples from normal lung parenchyma usually have a marked blood admixture and may contain a small amount of mucus. Typically, the nucleated cell count is low and consists mainly of respiratory epithelial cells. The epithelial cells are cuboidal to columnar, often ciliated, with a round, eccentric nucleus and lightly basophilic cytoplasm (Figure 13.67). Low numbers of alveolar macrophages are also commonly seen (Figure 13.68). Due to the blood admixture leukocytes will be present; however, their number should not exceed that which is expected in the blood. Other contaminants include ultrasound gel, corn starch (glove powder), and squamous cells from the skin. Samples may also contain mesothelial cells (Figure 13.69) and elements from an effusion (if present) due to the transthoracic technique used. If the sample is taken too far caudally, well-differentiated hepatocytes and skeletal muscle may be observed due to inadvertent aspiration of the liver or diaphragm (McCullough & Brinson, 1999a; Grimes et al., 2014).
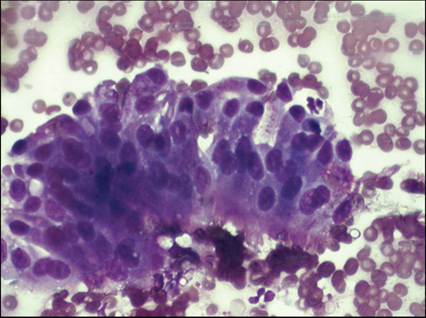
Figure 13.67 Respiratory epithelial cells. Respiratory epithelial cells may be seen with aspiration cytology of the lung. The epithelial cells can be cuboidal to columnar, are often ciliated, with a round, eccentric nucleus and lightly basophilic cytoplasm (Diff-Quik, 500? magnification).
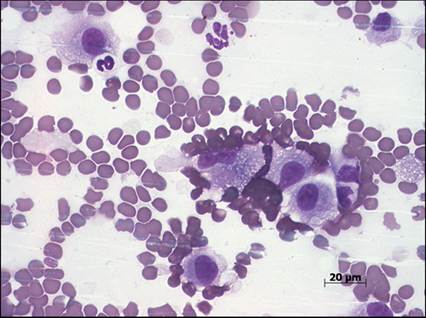
Figure 13.68 Alveolar macrophages. Low numbers of alveolar macrophages can be seen in samples obtained through aspiration of a lung lesion (Diff-Quik, 500? magnification).
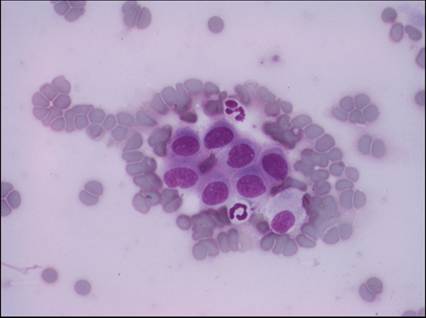
Figure 13.69 Contaminants in FNAs of lung tissue. A plaque of normal mesothelial cells can be seen due to contamination from the pleural lining during sample collection (Diff-Quik, 500? magnification).