Transtracheal wash and bronchoalveolar lavage
Collection techniques and sample preparation and preservation
Transtracheal wash (TTW) and bronchoalveolar lavage (BAL), with or without bronchial brushing, are generally used to evaluate the larger airways and smaller airways, including the alveoli, respectively.
The cytologic results between the two techniques can differ significantly, and should therefore be interpreted accordingly (Hawkins & DeNicola, 1989). Material is collected in a sterile manner from the tracheal lumen with tracheal washes, allowing cytological investigation for the presence of inflammation, infection, allergy, parasitic infestation, or neoplasia. Samples from a TTW can be collected either directly by entering through the cricothyroid ligament between two tracheal rings, or via an endotracheal (ET) tube. As muscle coverage increases towards the thoracic inlet, insertion of the needle between tracheal rings is easier in more anterior locations. For direct penetration of the tracheal wall, sedation is optional because it will impair the cough reflex, which is necessary for fluid retrieval. Depending on the size of the patient a 16- to 19-gauge jugular catheter is used. After numbing the area with local anesthetic, the catheter should be inserted with the bevel of the needle facing down, in a downward direction, to avoid laceration of the larynx and avoid contamination by the oropharynx. The catheter is then passed over the needle up to the level of the corina (4th intercostal space) and the needle removed. Approximately 0.1–0.2 ml/kg (maximum 10 ml) of warm, sterile, nonbacteriostatic saline is used, of which only half is initially injected using a 12 ml or larger syringe. A different syringe is used for aspiration of the fluid. Injected fluid remaining in the tracheobronchial tree will be absorbed and is not cause for concern. Although uncommon, complications may include subcutaneous emphysema, tracheal laceration, hemorrhage, cellulitis, hemoptysis, pneumomediastinum, and pneumothorax (Johnson & Vernau, 2011). A mild neutrophilic influx into the airways and transient bronchoconstriction may also occur (Kaneko et al., 1996). The method using an ET tube requires general anesthesia and should be reserved for small dogs and cats. Care should be taken not to contaminate the ET tube tip in the oropharynx. Once the tube is in place, the cuff should be inflated and the patient placed in lateral recumbency. A jugular catheter or sterile polypropylene urinary catheter is then inserted into the ET tube up to the point of the carina, after which saline is instilled and collected as previously described (Creevy, 2009; Creighton, 1974; McCullough & Brinson, 1999b).Bronchoalveolar lavage is indicated in patients with chronic coughing, bronchial or interstitial patterns on thoracic radiographs, and lung masses. Bronchoscopy is the ideal technique to obtain samples through BAL. Since BAL is used to sample the smaller airways and the alveoli, bronchoscopy will allow the operator to select specific lobes of the lung based on localization or severity of the lesion, as well as visualize masses that can be biopsied. The patient should be maintained under general anesthesia and the bronchoscope passed through an ET tube to allow visualization of the airways. Aliquots of warmed, sterile, nonbacteriostatic saline are injected through the biopsy channel. This is immediately reaspirated with a syringe or pump (Woods et al., 2014a). Multiple lung lobes should be lavaged to increase the possibility of identifying an etiologic agent (Hawkins et al., 1990, 1995; McCullough & Brinson, 1999b). In cats with lower respiratory disease, total and differential cell counts in BAL samples often differ significantly between lung segments and, therefore, clinicians should be cautious when using a single BAL cytology to define the inflammatory process present (Ybarra et al., 2012). If a bronchoscope is unavailable or the patient is too small for a scope, the ET tube technique may be used. As with TTW, the patient should be maintained under general anesthesia, the ET tube passed, and the patient placed in lateral recumbency with the most severely affected side down.
A sterile tube, long enough to reach up to the level of the 11th rib, should be inserted through the ET tube. The recommended total volume of warm, sterile saline for infusion, as previously described, is 1–3 ml/kg or 5–20 ml per site in dogs and 3–10 ml aliquots per site in cats (Hawkins et al., 1990; Finke, 2013; Johnson & Drazenovich, 2007; Dehard et al., 2008; Rajamäki et al., 2001a). The suction pump aspiration technique has been shown to improve BAL fluid retrieval compared with manual aspiration; however, the increased fluid retrieval did not significantly improve the rate of diagnostic success in dogs with pulmonary disease (Woods et al., 2014b). Preferably >50% of the infused volume should be recovered and it should have a foamy appearance which indicates the presence of surfactant and therefore adequate lavage of the lower airways (Woods et al., 2014a; Finke, 2013; Andreasen, 2003; Hawkins et al., 1990). The main complications associated with BAL are transient hypoxia, bronchoconstriction, and exacerbation of respiratory insufficiency (Johnson & Vernau, 2011; Johnson & Drazenovich, 2007; Allerton et al., 2013). Therefore, patients should be supplied with supplemental oxygen before, during, and up to 20 minutes after the procedure.Tracheobronchial brush samples allow cytological evaluation of visible endobronchial lesions (Rebar et al., 1980; Hawkins et al., 2006; Zhu et al., 2015). Samples are obtained using an endoscopic brush passed through the biopsy channel of the endoscope or, alternatively, a protected sterile cytology brush or culture swab can be introduced directly through the oral cavity and larynx into the tracheal for sample collection. It is a useful adjunct but not a replacement for BAL and useful when a potentially hypocellular BAL sample is collected. The agreement of tracheobronchial brush cytology with BAL cytology is good for detecting inflammation, with the type of inflammation identified dependent on the technique used (Zhu et al., 2015).
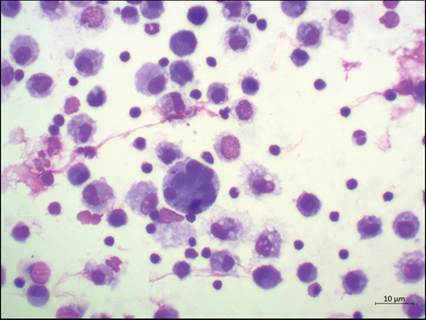
Inflammation in dogs with chronic cough is more readily identified on bronchial brushing cytology compared to BAL cytology (Hawkins et al., 2006). Bronchial brushings are also useful for detecting Bordetella organisms that are adherent to epithelial cells (Canonne et al., 2016).The processing of fluid samples should be standardized. Samples obtained through TTW or BAL should be divided into two portions: one portion should be placed into an EDTA tube to preserve cellular morphology and the other portion into a sterile container for possible microbial culture. Samples should ideally be placed on ice and processed within 30–60 minutes, since cell morphology is not well preserved in TTW/BAL samples (Andreasen, 2003; McCullough & Brinson, 1999b; Rebar et al., 1980). If this is not possible, the sample should be placed on ice or stored at 4°C and processed within 4 hours. The laboratory should be contacted before sample collection; however, if the sample cannot reach the laboratory within 60 minutes, direct smears should be made of turbid samples or mucoid material present in the sample, in an attempt to avoid cellular changes due to the low-protein environment as well as enzyme release by the cells. Macrophages and neutrophils may phagocytize RBCs, bacteria, and other debris if the sample is not processed within the prescribed period of time (McCullough & Brinson, 1999b; Rakich & Latimer, 1989a). The protein concentration in BAL samples is not routinely measured as it is very low. The determination of cell counts on BAL samples is questionable due to increased mucus and lack of standardization of techniques and therefore an inconsistent degree of dilution (Creevy, 2009; Woods et al., 2013). Cell counts can, however, be helpful in determining whether the BAL sample was adequate. A sample with a cell count be an incidental finding, while multinucleated are associated with cell activation and increased phagocytosis. Leukocytes such as neutrophils and eosinophils are frequently seen in washes and look like those seen in the blood (Figure 13.27).
Normal differential cell counts for BALs have been established for dogs and cats and are generally considered more important than absolute counts (Table 13.1) (Woods et al., 2014a; Rajamäki et al., 2001a; Rebar et al., 1980). Neutrophils usually represent the washes of normal dogs and cats, as well as in inflammatory conditions. This picture shows several neutrophils along with a single plasma cell, which resemble those seen in lymphoid tissue (Diff-Quik, 500? magnification).
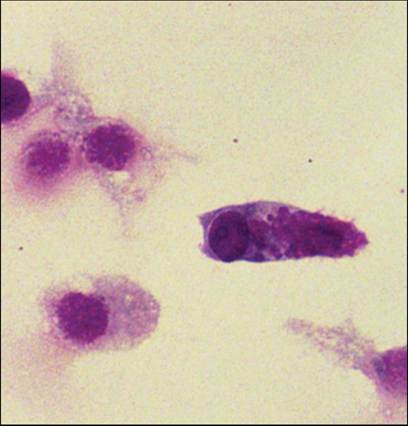
Figure 13.30 Goblet cells. Goblet cells are mucus-producing bronchial cells that are occasionally seen in normal transtracheal and bronchoalveolar washings. They are elongated cells and contain round granules of mucin that stain from red to blue to clear (Diff-Quik, 1,000? magnification).
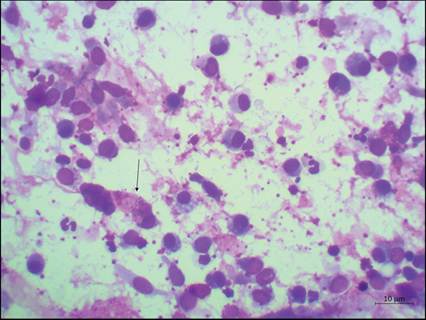
Figure 13.31 Goblet cells. Goblet cells are mucus-producing bronchial cells that are occasionally seen in normal transtracheal and bronchoalveolar washings. They are elongated cells and contain round granules of mucin that stain from red to blue to clear (Wright–Giemsa, 500? magnification).
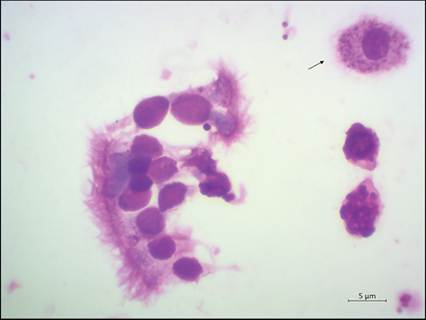
Figure 13.32 Goblet cells from a bronchoalveolar lavage. Two goblet cells with a rounded appearance, a small cluster of ciliated respiratory epithelial cells and a macrophage containing mucinous material (arrow) (Wright–Giemsa, 1,000? magnification).
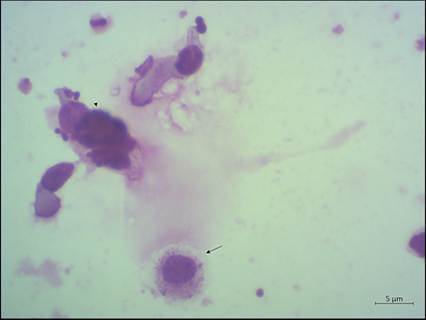
Figure 13.33 Goblet cell. Single elongated goblet cell with a cytoplasm distended by granules (arrowhead). A single macrophage (arrow) (Wright–Giemsa, 1,000? magnification).
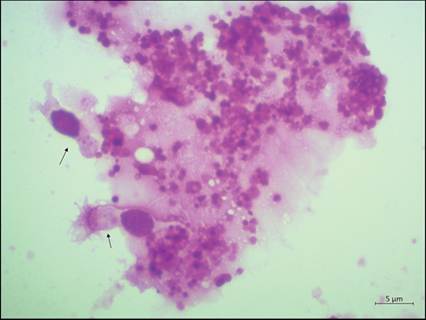
Figure 13.34 Free granules from ruptured goblet cells in bronchoalveolar lavage fluid.
A goblet cell and ciliated respiratory epithelial cells indicated by arrows (Wright–Giemsa, 1,000? magnification).
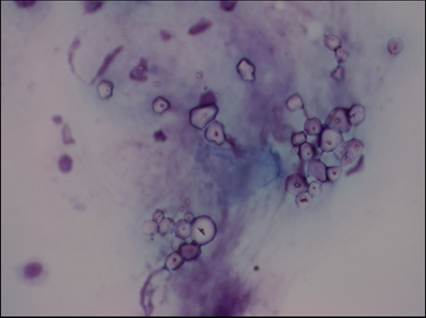
Figures 13.35 Corn starch. A transtracheal or bronchoalveolar wash from a dog containing corn starch (glove powder), which is occasionally seen in samples and is considered an incidental finding. Cytologically, corn starch appears as large, round to hexagonal structures that stain clear or blue and have a central fissure (Diff-Quick, 500? magnification).
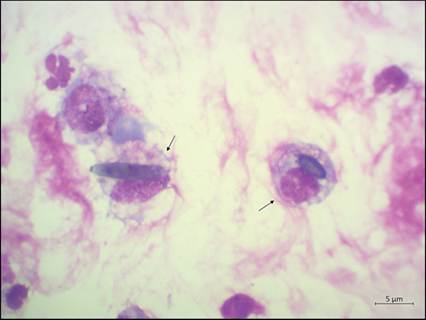
Figure 13.36 Pollen and plant material. Phagocytized pollen and plant material (arrows) in tracheal wash fluid (Wright–Giemsa, 1,000? magnification).
Cytologic interpretation
Samples of TTWs and BALs are usually interpreted according to the type, quantity, and proportion of cells recovered; however, information gathered from history taking, physical examination, and radiography should be considered. The cell proportions often differ between TTW and BAL samples. In general, cellular patterns can be categorized as: (a) insufficient sample, (b) oropharyngeal contamination, (c) eosinophilic infiltrate, (d) neutrophilic infiltrate, (e) macrophage infiltrate, and (f) the presence of atypical cells.
Insufficient sample
The absence of cells on a direct or concentrated preparation may indicate that the sample is not representative of the cytology of the respiratory tract. Similarly, when a predominance of only columnar respiratory epithelial cells, in the absence of alveolar macrophages, is seen in a BAL specimen, it indicates that only the airways and not the alveolar space has been effectively sampled.
Oropharyngeal contamination
Contamination is much more likely when TTWs or BALs are performed through an ET tube. Superficial squamous cells and a mixed population of bacteria (specifically Conchiformibius spp.) are the hallmarks for oropharyngeal contamination (Figures 13.37, 13.38) (Nyby et al., 1977b). Many bacteria may be seen adhered to the surface of squamous epithelial cells and generally without the presence of neutrophils. However, neutrophils may be present in a contaminated sample if the patient has a purulent or ulcerative oropharyngeal lesion or suffers from dental disease (Figure 13.39). Oropharyngeal contamination may therefore have a significant effect on the interpretation of the cytologic evaluation and culture results.
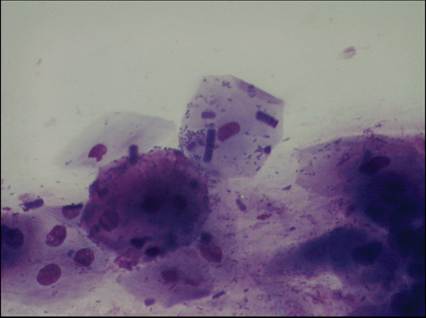
Figure 13.37 Oropharyngeal contamination. The presence of several large, superficial squamous cells associated with Conchiformibius spp. bacteria is a hallmark of oropharyngeal contamination (Diff-Quik, 500? magnification).
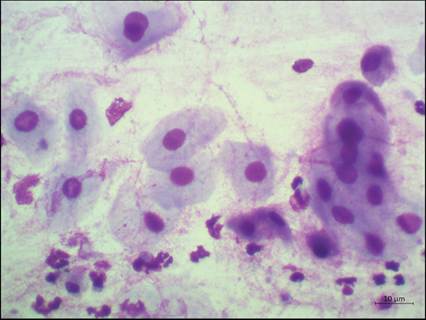
Figure 13.38 Oropharyngeal contamination. Sheet of squamous epithelial cells and some neutrophils in slightly mucinous background (Diff-Quik, 500? magnification).
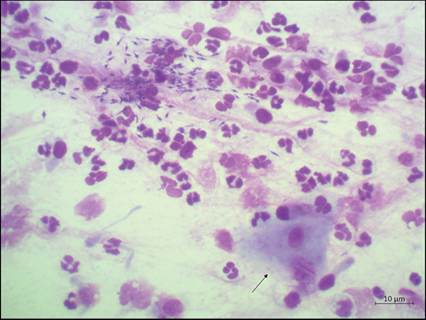
Figure 13.39 Oropharyngeal contamination. Neutrophils may be present in samples contaminated by the oropharynx, specifically when the patient suffers from oral or dental disease. Many neutrophils, a squamous epithelial cell (arrow), and extracellular bacteria are present in this bronchoalveolar lavage (Wright–Giemsa, 500? magnification).
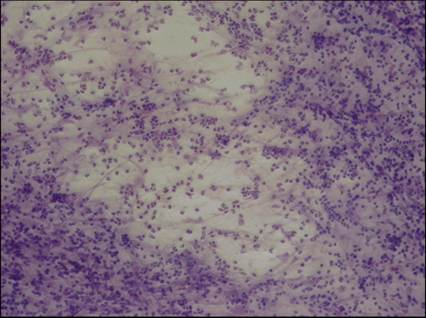
Figure 13.40 Inflammation. A bronchoalveolar lavage from a dog with inflammation of the lower respiratory tract. High numbers of neutrophils and some mucus strands are shown. When neutrophils are the predominant cell type, the sample should be closely examined for the presence of an infectious agent, such as bacteria (arrow) (Diff-Quik, 100? magnification).
Inflammation
Normally, neutrophils are present in very low numbers (inhalation of a toxic substance, as well as neoplasia (Andreasen, 2003; McCullough & Brinson, 1999b). Neutrophilic inflammation can also be induced with the aspiration of water that contains diatom algae (Benson et al., 2013). The presence of neutrophils with phagocytosed nuclear material, morphologically consistent with presumed lupus erythematosus cells, has been reported in the BAL fluid from a dog with a clinical diagnosis of systemic lupus erythematosus (Black et al., 2017). An increased amount of mucus can be seen with inflammation, irritation, or upper airway damage (chronic respiratory disease) due to increased numbers of goblet cells (Figure 13.47). Mucus usually stains more eosinophilic with inflammatory conditions due to the incorporation of inflammatory proteins and material from lysed cells (Figure 13.48) (Creighton, 1974). Curschmann’s spirals are mucus casts of small bronchioles that appear as spiral, twisted masses of mucus that may have perpendicular radiations (bottle-brush-like appearance; Figures 13.49, 13.50, 13.51). They are seen with disorders that result in chronic, excessive mucus production and are usually an indication of bronchiolar obstruction (Andreasen, 2003; Johnston, 1986). Increased numbers of alveolar macrophages are frequently seen with subacute and chronic pulmonary disorders, such as chronic persistent inflammation (Figure 13.52). Activated alveolar macrophages can also become bi- and multinucleated, known as giant cell macrophages (Figures 13.53, 13.54), with pulmonary disorders associated with chronic or pyogranulomatous inflammation (Andreasen, 2003). Epithelioid macrophages, characterized by granular eosinophilic cytoplasm, tend to cluster at sites of granuloma formation. Anthracotic pigment (dark or black granules) may be present within macrophages from clinically normal animals living in large cities or areas with polluted air (Roza & Viegas, 2007). Hyperplastic epithelium, together with goblet cell hyperplasia and increased mucus, is an additional change that can be seen with chronic inflammation. Cytologically, hyperplastic epithelium presents as variably sized, deeply basophilic epithelial cells (Figure 13.55).
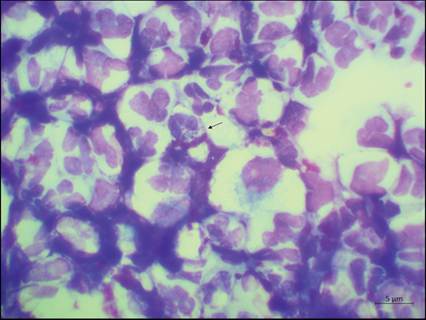
Figure 13.41 Inflammation. A bronchoalveolar lavage from a dog with inflammation of the lower respiratory tract. High numbers of neutrophils and some mucus strands are shown. When neutrophils are the predominant cell type, the sample should be closely examined for the presence of an infectious agent, such as bacteria (arrow) (Wright–Giemsa, 1,000? magnification).
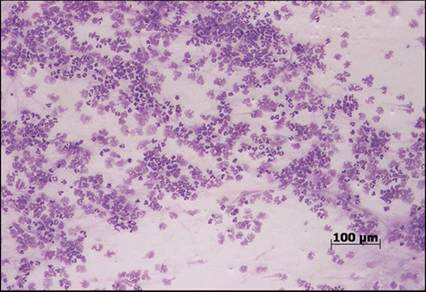
Figure 13.42 Inflammation. Neutrophils may show degenerative changes in the presence of bacterial toxins or may be smudged (ruptured) secondary to trauma from collection and preparation (Diff-Quik, 100? magnification).
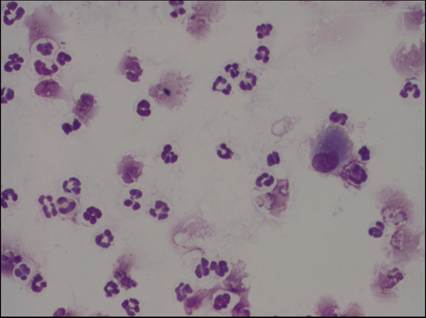
Figure 13.43 Inflammation. Bronchoalveolar lavage with several non-degenerate neutrophils. The nuclei of the non-degenerate neutrophils are slender with clear lobulation and stain darkly (Diff-Quik, 500? magnification).
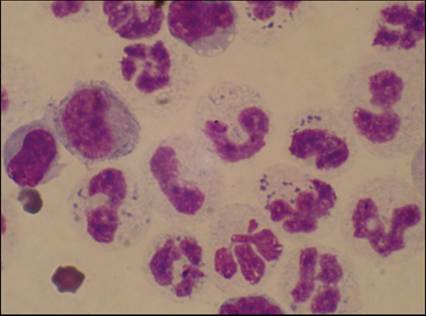
Figure 13.44 Inflammation. Cytologic appearance of degenerative neutrophils in samples includes a thicker nucleus that stains a lighter eosinophilic color and loses nuclear lobulation (karyolysis) (Diff-Quik, 1,000? magnification).
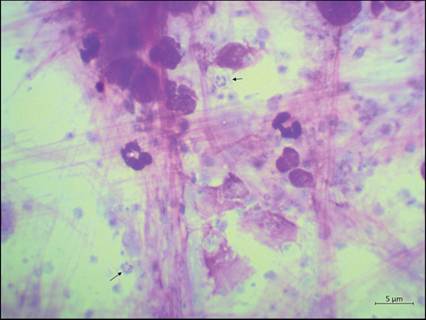
Figure 13.45 Inflammation in a tracheal wash of a dog. Numerous small (1–2 μm) oval organisms with a clear cytoplasm and peripheral nucleus, either occurring singly or arranged in a ring formation inside a cyst (arrows), in the background. These organisms are consistent with Pneumocystis spp. (Wright–Giemsa, 1,000? magnification).
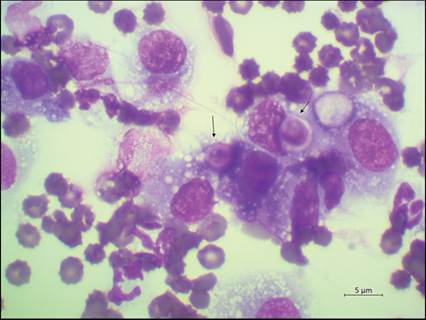
Figure 13.46 Inflammation in a bronchoalveolar lavage of a dog. Activated alveolar macrophages displaying phagocytosis of Cryptococcus neoformans yeast-like organisms (arrows) (Diff-Quik, 1,000? magnification).
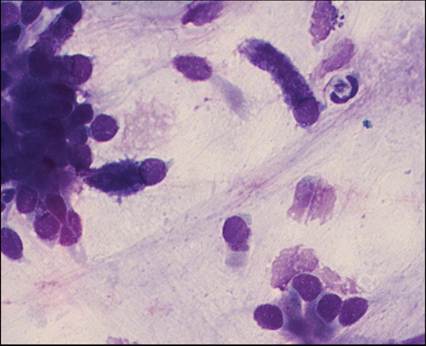
Figure 13.47 Goblet cells. An increased amount of mucus can be seen with inflammation, irritation, or upper airway damage (chronic respiratory disease) due to increased numbers of goblet cells. Goblet cells are distinguished from normal respiratory epithelial cells based on the presence of distinct large, intracytoplasmic, purple globules (Diff-Quik, 1,000? magnification).
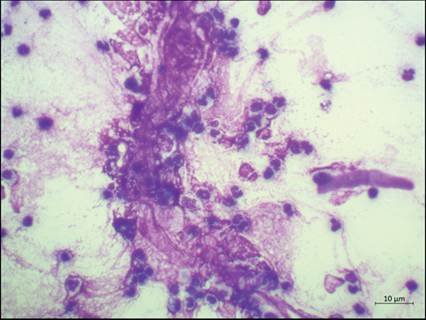
Figure 13.48 Mucus. Dark eosinophilic mucus is commonly seen with inflammatory conditions due to the incorporation of inflammatory proteins from lysed cells (Wright–Giemsa, 500? magnification).
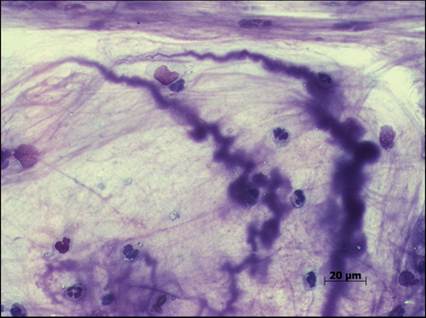
Figure 13.49 Curschmann’s spirals. Curschmann’s spirals are twisted mucus casts of small bronchioles that have a bottle-brush appearance due to perpendicular radiations. They are seen with disorders that result in chronic, excessive mucus production and are usually an indication of bronchiolar obstruction (Diff-Quik: both, 500? magnification).
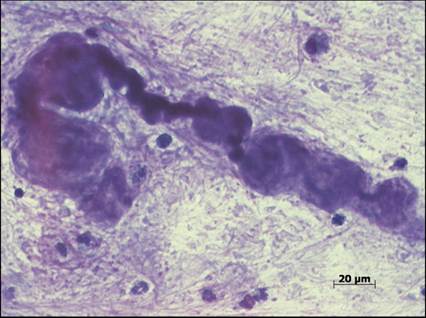
Figure 13.50 Curschmann’s spirals. Curschmann’s spirals are twisted mucus casts of small bronchioles that have a bottle-brush appearance due to perpendicular radiations. They are seen with disorders that result in chronic, excessive mucus production and are usually an indication of bronchiolar obstruction (Diff-Quik: both, 500? magnification).
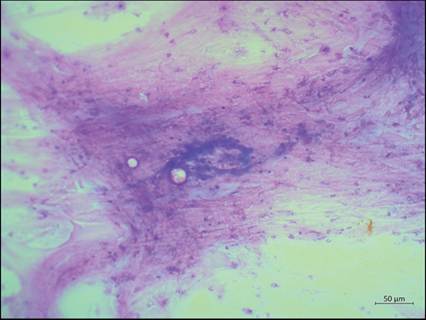
Figure 13.51 Curschmann’s spirals. Densely wound, deep basophilic mucus strands in a background of streaming eosinophilic mucus and cells (Wright–Giemsa, 100? magnification).
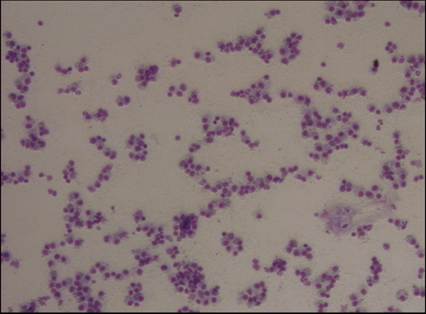
Figure 13.52 Alveolar macrophages. Increased numbers of alveolar macrophages are typically seen with subacute and chronic pulmonary disorders (Diff-Quik, 100? magnification).
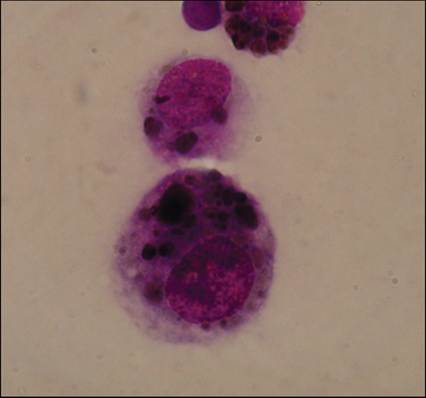
Figures 13.53 Giant cell macrophages. In chronic pulmonary inflammation, activated alveolar macrophages can become multinucleated and are then known as giant cell macrophages (Wright–Giemsa: both, 500? magnification).
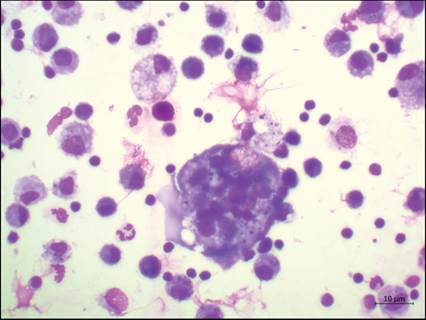
Figure 13.54 Giant cell macrophages. In chronic pulmonary inflammation, activated alveolar macrophages can become multinucleated and are then known as giant cell macrophages (Wright–Giemsa: both, 500? magnification).
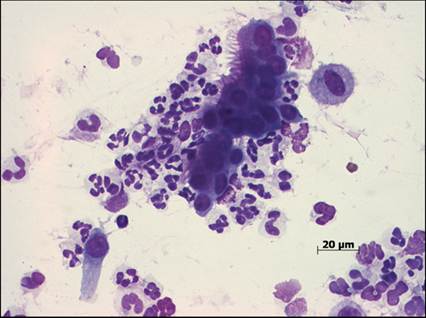
Figure 13.55 Hyperplastic respiratory epithelium. Hyperplastic respiratory epithelium is a change that can be seen with chronic inflammation. Cytologically, hyperplastic epithelium presents as variably sized, deeply basophilic epithelial cells (Diff-Quik, 500? magnification).
Hypersensitivity
Healthy animals normally have a very low percentage (10% eosinophils are indicative of a significant hypersensitivity disease; however, clinically healthy/asymptomatic cats may have significantly higher numbers of eosinophils (up to 28%) (Wright–Giemsa, 500? magnification).
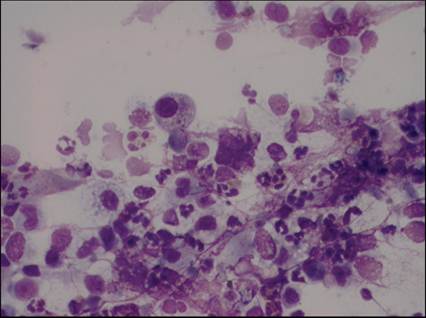
Figure 13.57 Eosinophils. When the sample contains a lot of mucus, eosinophils may become trapped and therefore predominate in certain areas of the slide. Their granules sometimes do not stain properly (Diff-Quik, 500? magnification).
Hemorrhage
Erythrocytes are not commonly present in BAL. Erythrophagocytosis (consistent with acute hemorrhage) (Figure 13.58) and/or macrophages containing pigmented hemoglobin breakdown products (hemosiderophages; associated with chronic hemorrhage) may be seen in conditions that cause pulmonary hemorrhage (Figures 13.59, 13.60). Hemoglobin breakdown products include hemosiderin (granular, bright blue to black pigment; Figures 13.61, 13.62) or hematoidin (small, bright yellow to orange crystals; Figure 13.63). These cytologic findings are essential for differentiating between iatrogenic hemorrhage and hemorrhage caused by pulmonary pathology such as congestive heart failure, feline asthma, neoplasia (primary and metastatic), infectious pneumonia, foreign body migration, heartworm emboli, coagulopathies, trauma, pulmonary embolism, neurological disease, tracheal collapse, and lung lobe torsion (DeHeer & McManus, 2005; McCullough & Brinson, 1999b; Perez-Arellano et al., 1992). Cats are 13 times more likely to have pulmonary hemosiderosis on BAL cytology compared with dogs (Hooi et al., 2019). Although no risk factors associated with pulmonary hemosiderosis have been identified in cats, increased respiratory rates, prolonged bronchoalveolar lavage times, concurrent transthoracic FNA biopsies, and cytologic diagnoses are associated with an increased risk in dogs (Hooi et al., 2019). Low to moderate numbers of hemosiderophages may be seen in tracheal wash fluid in cats with rhinitis and asthma (DeHeer & McManus, 2005).
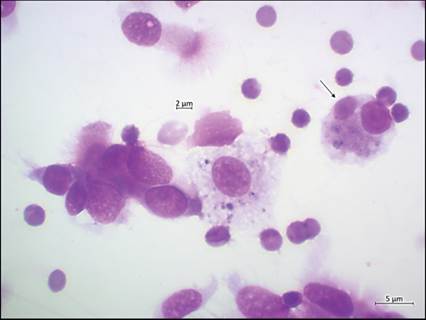
Figure 13.58 Hemorrhage. An alveolar macrophage showing erythrophagocytosis (arrow), indicating acute hemorrhage (Diff-Quik, 1,000? magnification).
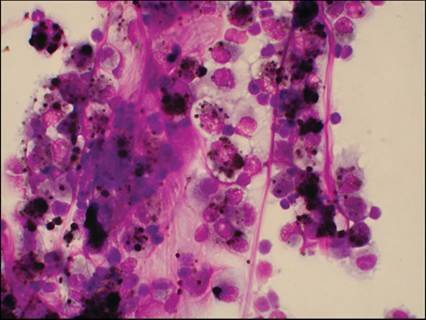
Figure 13.59 Hemorrhage. Alveolar macrophages containing pigmented hemoglobin breakdown (hemosiderophages) products are typically seen with conditions associated with chronic pulmonary hemorrhage (Diff-Quik: both, 500? magnification).
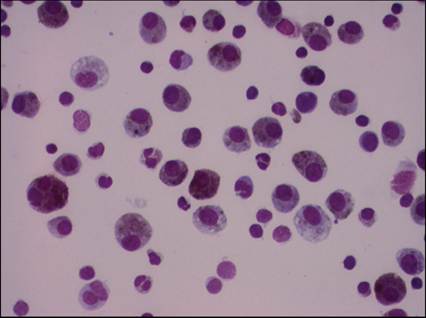
Figure 13.60 Hemorrhage. Alveolar macrophages containing pigmented hemoglobin breakdown (hemosiderophages) products are typically seen with conditions associated with chronic pulmonary hemorrhage (Diff-Quik: both, 500? magnification).
Figures 13.61 Hemorrhage. Hemosiderin, a breakdown product of hemoglobin, is often observed in macrophages of dogs and cats with chronic pulmonary hemorrhage and appears as a granular, bright blue to black pigment (Diff-Quik: both, 1,000? magnification).
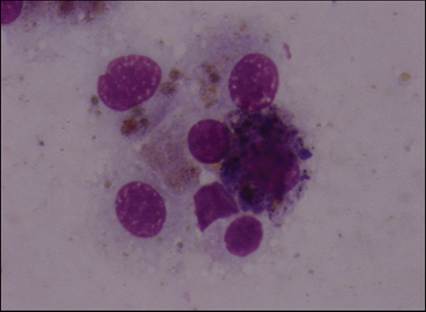
Figure 13.62 Hemorrhage. Hemosiderin, a breakdown product of hemoglobin, is often observed in macrophages of dogs and cats with chronic pulmonary hemorrhage and appears as a granular, bright blue to black pigment (Diff-Quik: both, 1,000? magnification).
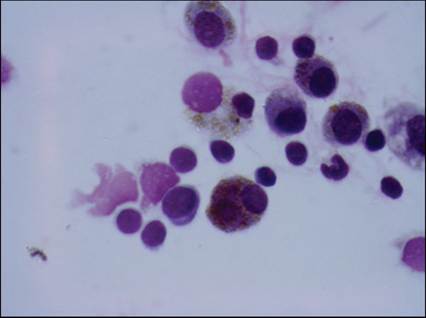
Figure 13.63 Hemorrhage. Hematoidin is also a breakdown product of hemoglobin and appears as small, bright yellow to orange crystals inside the macrophage (Diff-Quik, 1,000? magnification).
Necrosis
Samples containing necrotic material can be seen with inflammatory or neoplastic conditions. Cytologically, necrosis is characterized by the presence of basophilic granular to amorphous background material (Figures 13.64, 13.65). The material is often acellular, but inflammatory or even neoplastic cells may occasionally be imbedded in the material.
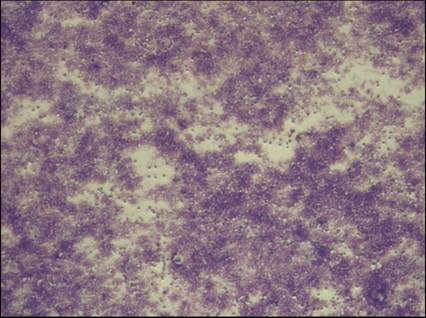
Figure 13.64 Necrosis. Necrosis can be seen with inflammatory or neoplastic conditions. Necrotic material appears cytologically as basophilic granular to amorphous background material (Diff-Quik, 100? magnification).
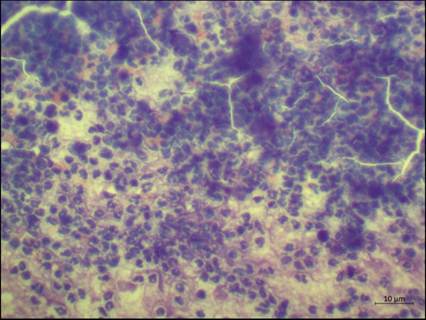
Figure 13.65 Necrosis. Necrosis can be seen with inflammatory or neoplastic conditions. Necrotic material appears cytologically as basophilic granular to amorphous background material (Wright–Giemsa, 500? magnification).
Neoplasia
Primary lung tumors or metastatic tumors are generally interstitial, and therefore neoplastic cells are rarely found in TTW/BAL samples unless the tumor has eroded into the airways or if it is a primary tumor involving the bronchial tree. Sometimes, the affected portion of the bronchial tree can be clogged with secretions and necrotic material, preventing cells from being collected via TTW/BAL. A definitive or supportive diagnosis yielded by BAL has been reported in 10 of 14 lung carcinomas (Hawkins et al., 1994). In contrast, a definitive diagnosis of canine primary pulmonary tumors, by tracheal wash, was only possible in 1 of 6 cases (McNiel et al., 1997). A very good agreement has been reported for the diagnosis of pulmonary carcinoma in dog and cat samples when comparing cytopathologic and histopathologic interpretation (Wood et al., 1998a; DeBerry et al., 2002b). Hyperplastic epithelial cells may appear as clusters with cells showing changes such as anisocytosis and, therefore, may be misinterpreted as neoplastic. Carcinomas (epithelial cell tumors) are most commonly seen (up to 80% of primary lung tumors). If clusters of cells are present, the cells should be examined for criteria of malignancy such as anisocytosis, anisokaryosis, multiple nuclei, prominent and multiple nucleoli, and nuclear molding. If there is cytologic evidence of acini formation or secretory product production (i.e., signet ring cell formation), it is classified as adenocarcinoma (Figure 13.66). In the case of lymphoma, pulmonary involvement may be determined through TTW/BAL samples (Andreasen, 2003; Hahn et al., 1996; Hawkins et al., 1993; McCullough & Brinson, 1999b).
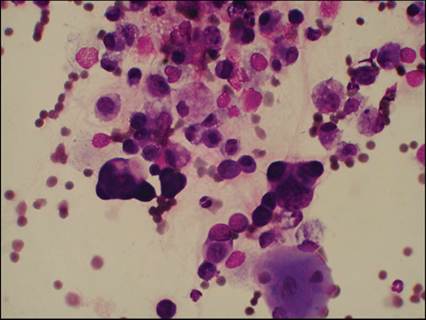
Figure 13.66 Primary lung neoplasia. Primary lung tumors or metastatic tumors are rarely found in bronchoalveolar samples. Carcinomas are most commonly seen and may show malignant criteria such as anisocytosis, anisokaryosis, very basophilic cytoplasm, multiple nuclei, and prominent and multiple nucleoli (Diff-Quik, 500? magnification).