Inflammation of the nasal cavity
Infectious
Neutrophils predominate in nasal exudates associated with bacterial, viral, and some fungal infections. Other inflammatory cells, such as macrophages, lymphocytes, and plasma cells, may also be present (Figure 13.8).
The normal bacterial flora in the nasal and oral cavities is generally pleomorphic; therefore a monomorphic bacterial population suggests either infection or bacterial overgrowth (Figure 13.9; French, 1987; Michiels et al., 2003). Neutrophils containing phagocytized bacteria consisting of a monomorphic population strongly suggest infection (Figure 13.7). Primary bacterial infections are rare and usually secondary to mucosal injury, viral, parasitic, or fungal infections, dental disease, oronasal fistulas, idiopathic lymphoplasmacytic rhinitis, and neoplasia. These conditions should be suspected in a patient with sinusitis that is unresponsive to antimicrobial therapy. Cytologic findings with viral rhinitis are nonspecific and often only secondary bacterial infection, with the presence of various types of inflammatory cells, can be seen (Windsor & Johnson, 2006; Windsor et al., 2006). With mycotic rhinitis, fungal hyphae may be difficult to identify between cells and debris because they may not stain well with Romanowsky stain and appear as clear filamentous structures. The most common fungal agents responsible for mycotic rhinitis in dogs are Aspergillus spp. and Penicillium spp. (Figure 13.10), whereas Cryptococcus spp. occur more frequently in cats (Figure 13.11). Aspergillus spp. and Penicillium spp. are morphologically similar and present as septate, branching hyphae (2–4.5 μm wide), associated with serosanguineous to mucopurulent nasal exudates, nasal mucosal necrosis, and turbinate destruction (Peeters & Clercx, 2007; Day, 2011). Although fungal rhinosinusitis, caused by Aspergillus spp., occurs less frequently in cats, two forms have been described, namely sinonasal aspergillosis and sinoorbital aspergillosis (most common). Both infections start in the nasal cavity and brachycephalic breeds of cats, especially Persian and Himalayan, are predisposed. Feline sinonasal aspergillosis is usually noninvasive with a favorable prognosis, whereas feline sinoorbital aspergillosis carries a guarded to poor prognosis (Barrs & Talbot, 2020; Barachetti et al., 2009). Cryptococcus neoformans is a saprophytic yeast that is round to oval (3.5–7.0 μm in diameter), stains basophilic, and is surrounded by a thick polysaccharide capsule (1–30 μm) that stains poorly with Wright–Giemsa or Diff-Quik® stains. Narrow-based budding is a feature of the organism (Figure 13.12). The organism is often diagnosed by examining only touch imprints of nasal lesions or exudates (Lester et al., 2011; Sykes & Malik, 2012). An increase in the prevalence of subclinical cryptococcosis and asymptomatic dog and cat carriers of Cryptococcus gattii has been reported, which may contribute to outbreaks of clinical cryptococcosis in humans and animals (Duncan et al., 2005). 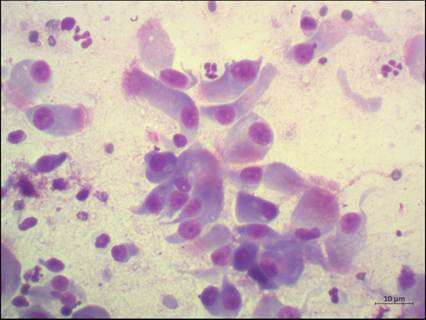
Figure 13.8 Neutrophilic inflammation. Several neutrophils and a few lymphocytes are seen amongst clusters of ciliated and nonciliated respiratory epithelial cells (Wright–Giemsa, 500? magnification).
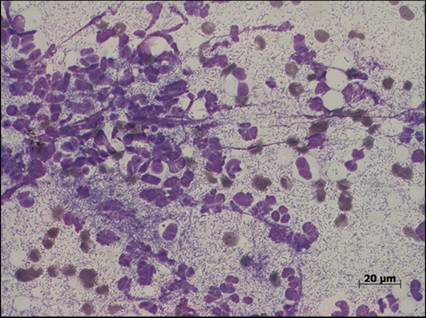
Figure 13.9 Bacterial overgrowth. An overgrowth of a monomorphic population of bacteria. The high number of neutrophils most likely indicates a bacterial infection despite the fact that all of the bacteria appear to be extracellular (Diff-Quik, 500? magnification).
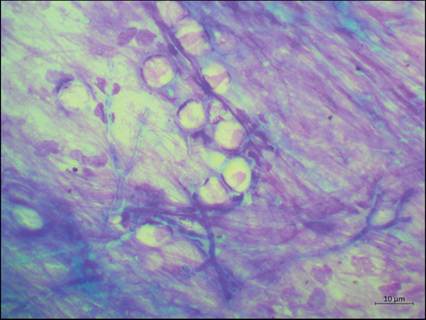
Figure 13.10 Fungal infection. Fungal hyphae – branching, septate with straight, parallel walls and globose terminal ends – arranged in mats and individually.
The hyphae resembled that of Aspergillus or Penicillium spp. (Wright–Giemsa, 500? magnification).
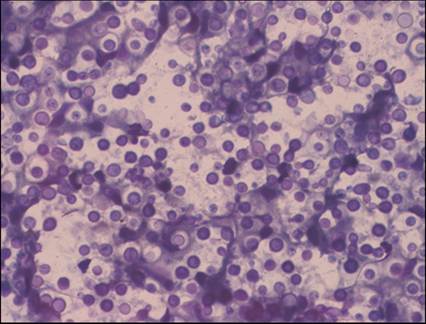
Figure 13.11 Nasal cryptococcosis. Numerous round to oval, basophilic staining yeasts surrounded by a thick nonstaining polysaccharide capsule. This is the typical presentation for Cryptococcus neoformans. Narrow-based budding is also often seen cytologically (Diff-Quik, 500? and 1,000? magnification, respectively).
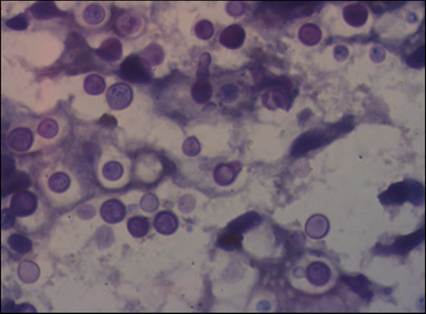
Figure 13.12 Nasal cryptococcosis. Numerous round to oval, basophilic staining yeasts surrounded by a thick nonstaining polysaccharide capsule. This is the typical presentation for Cryptococcus neoformans. Narrow-based budding is also often seen cytologically (Diff-Quik, 500? and 1,000? magnification, respectively).
Noninfectious
Foreign bodies such as plant awns or twigs are fairly common in dogs and are either directly inhaled or enter the nasal cavity traumatically through the external nares, the nasal planum, or through the palate via the oral cavity. Typically, a marked, suppurative to pyogranulomatous, inflammatory reaction is present and close attention should be paid to identifying any foreign material. Eosinophils may predominate in nasal exudates resulting from allergic rhinitis, but may also be present in response to parasites, fungi, bacteria, and neoplasia (Burkhard & Millward, 2010; Arndt, 2014).
Neoplasia of the nasal cavity
Neoplasia of the nasal cavity is uncommon in dogs and cats, but carries a poor prognosis when present because the majority of nasal tumors are malignant (80–90%). Malignant tumors, such as carcinomas, are more often seen in older animals, involve the caudal two-thirds of the nasal cavity, and result in destruction of the nasal turbinates and septum. Metastasis, however, is uncommon and may only be present in the late stages of the disease.
Malignant epithelial tumors are seen more frequently and include adenocarcinoma, squamous cell carcinoma, transitional carcinoma, and undifferentiated carcinoma (Norris, 1979; Legendre, 1983).Adenocarcinomas are cytologically characterized by the presence of small aggregates to large sheets of neoplastic epithelial cells (Figures 13.13, 13.14). Malignant cells show various anaplastic changes such as macrocytosis, mild to moderate anisocytosis and anisokaryosis, basophilic cytoplasm that may contain numerous discrete vacuoles, an increased nuclear to cytoplasm (N:C) ratio, and increased number of visible nucleoli per nucleus, some with shape variations (Figure 13.15). Adenocarcinomas may be associated with the production of mucus, which appears as extracellular, amorphous to fibrillar, eosinophilic material. Anaplastic cells may individualize and appear as discrete round cells. These neoplastic changes may be difficult to differentiate from other ‘normal’, adaptive changes that may be seen with chronic inflammation or irritation. Hyperplasia and/or dysplasia are mechanisms for tissue cells to undergo adaptive changes in order to survive amid a pathologic stimulus such as chronic inflammation. Hyperplasia (increased number of cells) is often accompanied by dysplasia (loss of architectural organization) and may present as sheets of epithelial cells with an increased N:C ratio, mild to moderate anisocytosis, basophilic cytoplasm, and the presence of mitotic figures (Figure 13.16). Chronic ongoing inflammation may result in squamous metaplasia (Figure 13.17), where the normal cell type is transformed into one that is better able to endure the environmental stress while losing specialized function (squamous cells). Both hyperplasia and metaplasia may result in neoplasia. Squamous cell carcinomas present cytologically as large cells with angular borders, abundant cytoplasm, and centrally placed nuclei (Figure 13.18). The neoplastic epithelial cells can present in various stages of maturation: from immature, small, cuboidal, nucleated cells with deeply basophilic cytoplasm to large, mature, angular cells with abundant, pale cytoplasm and large nuclei.
Cytologic preparations are often associated with marked anisokaryosis accompanied by a moderate to marked neutrophilic inflammatory response. The presence of perinuclear vacuoles strongly suggests squamous cell origin (Burkhard Millward, 2010; Arndt, 2014). Mesenchymal tumors of the nasal cavity are uncommon and normally these tumors exfoliate poorly, which complicates cytologic diagnosis. Cytologic samples typically present as low cellular samples with the occasional individual or aggregate of plump, fusiform, or spindle-shaped cells. Mesenchymal tumors most often seen include osteosarcoma (Figure 13.19), fibrosarcoma, and chondrosarcoma. Round cell (discrete cell) tumors, such as lymphoma, mast cell tumors (Khoo et al., 2017), and transmissible venereal tumors, have been reported to occur in the nasal cavity of dogs and cats. Cytologic characteristics include highly cellular samples consisting of a homogeneous population of individualized, neoplastic round cells with distinct cytoplasmic borders, and morphologic characteristics resembling those seen in other sites (Arndt, 2014; Burkhard Millward, 2010). 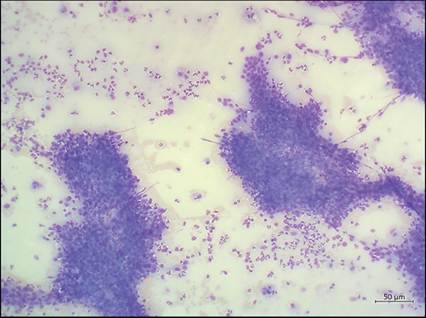
Figure 13.13 Nasal adenocarcinoma. Several cohesive sheets of epithelial cells from a nasal mass (Wright–Giemsa, 100? magnification).
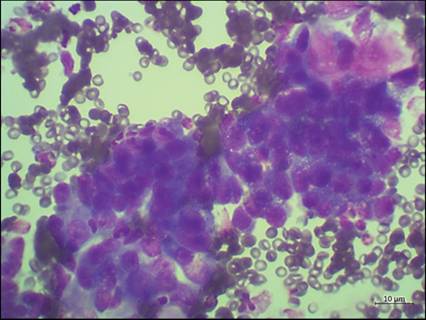
Figure 13.14 Nasal adenocarcinoma. A sheet of pleomorphic epithelial cells showing anisocytosis, anisokaryosis, and prominent nucleoli (Wright–Giemsa, 500? magnification).
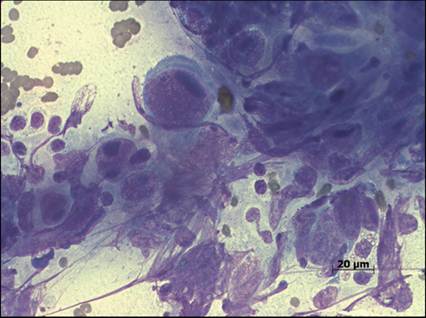
Figure 13.15 Nasal adenocarcinoma. Neoplastic epithelial cells display various cytologic signs of malignancy such as macrocytosis, marked anisocytosis and anisokaryosis, basophilic cytoplasm, an increased nuclear to cytoplasm ratio, and increased number of visible nucleoli per nucleus, some with shape variations (Diff-Quik, 500? magnification).
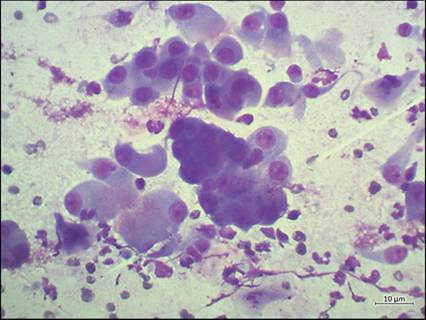
Figure 13.16 Epithelial hyperplasia and/or dysplasia. Nasal epithelium undergoes hyperplastic changes in order to survive amid a pathologic stimulus such as chronic inflammation. Hyperplasia is often accompanied by dysplasia and may present as sheets of epithelial cells with an increased nuclear to cytoplasm ratio, mild to moderate anisocytosis, and basophilic cytoplasm (Wright–Giemsa, 500? magnification).
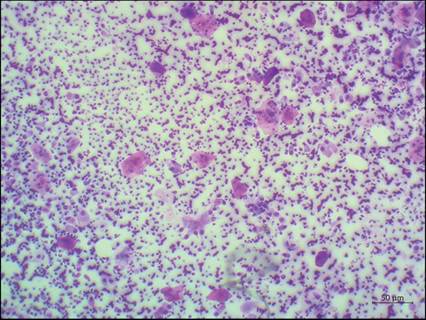
Figure 13.17 Squamous metaplasia. Chronic ongoing inflammation may result in the normal cell type changing into one that is better able to endure the environmental stress while losing specialized function (squamous cells) (Wright–Giemsa, 100? magnification).
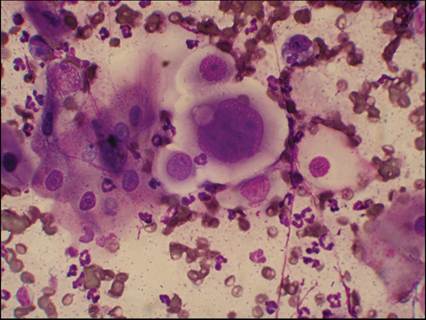
Figure 13.18 Squamous cell carcinoma. Squamous cell carcinomas present cytologically as large cells with angular borders, abundant cytoplasm, and centrally placed nuclei. The neoplastic epithelial cells can vary from immature, small, cuboidal, nucleated cells with deeply basophilic cytoplasm to large, mature, angular cells with abundant, pale cytoplasm and large nuclei. Cytologic criteria include marked anisokaryosis accompanied by a moderate to marked neutrophilic inflammatory response (Diff-Quik, 500? magnification).
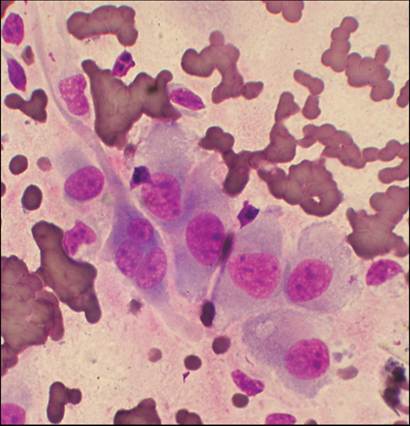
Figure 13.19 Osteosarcoma. The presence of individual or aggregates of plump, fusiform, or spindle-shaped cells, with cytoplasm streaming away from the nuclei may indicate a mesenchymal tumor of the nasal cavity (Diff-Quik, 500? magnification).