Nasal cavity
The most common reported causes for chronic nasal disease in dogs and cats include neoplasia, followed by lymphocytic-plasmacytic rhinitis or chronic rhinitis, and fungal infection.
Primary bacterial rhinitis is rare in dogs and cats and is usually secondary to foreign bodies or disorders where there is disruption of normal mucociliary mucosal integrity (Lobetti, 2009; Meler et al., 2008; Cohn, 2020; Henderson et al., 2004).Collection techniques and sample preparation
A thorough visual inspection of the nasal cavity through endoscopy (rhinoscopy), as well as localization of the lesion(s), using imaging modalities such as radiography or computed tomography (CT), should be performed prior to obtaining samples for cytologic examination. It is advisable to perform a complete blood count (CBC) and hemostatic profile prior to sample collection since most sampling techniques result in significant hemorrhage due to the rich vascular supply of the nasal mucosa. Hemorrhage may obscure proper visualization of the cavity and hamper radiographic interpretation; therefore, radiography should be performed prior to rhinoscopy and sample collection. Rhinoscopic evaluation of the nasal cavity is unable to predict the presence or absence of inflammation and, therefore, it is important to obtain samples for microscopic evaluation either through nasal swabs, nasal flushing, nasal brushing, fine needle aspiration (FNA) biopsy, or pinch biopsy techniques. General anesthesia, together with a properly inflated endotracheal tube and packing of the oropharynx with gauze, is recommended during sample collection. Tilting the patient’s nose downward will further prevent any aspiration during the procedure (Tasker et al., 1999; Elie & Sabo, 2006; Miller, 2007).
Superficial and deep nasal swabs are easily obtained and nontraumatic but are limited to identifying superficial inflammation, secondary bacterial infection, hemorrhage, or necrosis and do not provide much information on disease processes involving the deeper lying nasal mucosa.
However, some infectious diseases, such as cryptococcosis in cats, are easily diagnosed by cytologic examination of the nasal discharge. Samples obtained through nasal flushing can also be very unrewarding; therefore more invasive techniques are needed to yield diagnostic material. A traumatic nasal flush can be accomplished by nicking the catheter, creating a rough surface that will assist with dislodging material. Care must be taken not to penetrate the cribriform plate. The distance from the external nares to the medial canthus of the eye should be measured beforehand, and the catheter should be marked or cut to the appropriate length. Small amounts (5–10 ml) of nonbacteriostatic, sterile saline are flushed into the cavity via a 20–35 ml syringe with alternating positive and negative pressure. The catheter should be moved back and forth against the mucosa as the fluid enters the cavity, in an attempt to acquire deeper lying tissue cells. An alternative method involves directing the catheter into the nasopharynx via the oral cavity and retroflexing it around the soft palate. Once the bulb of the catheter is inflated, saline can be lavaged through the nasal cavity and collected at the external nares. This technique is especially useful in patients with very small nasal passages, such as cats and small dogs (Tasker et al., 1999; Kuehn, 2006). Any fluid retrieved through either method should be collected in an EDTA-anticoagulated tube for microscopic examination. EDTA is considered to be bacteriostatic; therefore samples for microbiology should be collected using a sterile swab or into a sterile tube. If the fluid is very turbid, direct smears can be made of the particulate matter using the ‘squash’ preparation technique. Briefly, a drop of fluid is placed on a clean slide with a second slide placed on top, perpendicularly. Once the fluid has spread, the two slides are pulled apart in a horizontal fashion with minimal vertical pressure applied. If the fluid is clear, the sample can be centrifuged and smears prepared of the sediment. If available, cytocentrifugation can be used for further concentration of the sample. One study described a minimally invasive hydropulsion method of forceful nasal flushing, which was able to obtain a large sample for biopsy of nasal tumors in dogs and cats. The study reported a success rate for definitive diagnosis of 90.2%, higher than previous reports of nasal flushing and endoscopic pinch biopsy techniques. This technique was successful in obtaining tissue from a variety of tumors, and the gross rhinoscopic appearance of the mass did not influence the success of the hydropulsion (Ashbaugh et al., 2011).A cytobrush or endoscopic brush can be used to collect tissue to roll on a clean glass slide for cytologic examination; however, brush cytology often misses the deeper inflammatory cells and may not correlate with histologic findings. One study reported very poor agreement between cytologic and histologic samples in cats, with only 25% of samples having the same predominant cell type (Michiels et al., 2003). Brush cytology has been shown to correctly identify neoplasia of epithelial origin in 86–88% of cases, but diagnoses of mesenchymal tumors are less likely (Clercx et al., 1996; Caniatti et al., 2012). Brush cytology samples with high cellularity are reported to have lower sensitivity for the diagnosis of neoplasia compared with samples having low or moderate cellularity (Caniatti et al., 2012). Fine needle aspiration biopsy or biopsy, using a large gauge polypropylene urinary catheter with the end cut at a 45° angle, attached to a syringe, has been shown to yield the most diagnostic material when a mass lesion is present. It is important, however, to accurately identify the location of the mass using various imaging techniques. Care should again be taken not to penetrate the cribriform plate. Alligator biopsy forceps can be used to obtain a pinch biopsy for impression cytology and histopathology (Withrow et al., 1985; Tasker et al., 1999).
Normal cytology of the nasal cavity
In healthy animals, samples collected from the nasal cavity contain few cells and a small amount of mucus.
Large, nonkeratinized squamous epithelial cells, often associated with low numbers of mixed population extracellular bacteria (normal bacterial flora) colonizing their surface, are obtained from the oropharynx and external nares (Figure 13.1). The presence of Conchiformibius spp. (previously known as Simonsiella spp.) in the sample confirms oropharyngeal contamination. Conchiformibius spp. are large, rod-shaped bacteria that align in a row after division, giving them a distinctive ‘bar code’ appearance (Figure 13.2) (Nyby et al., 1977a). 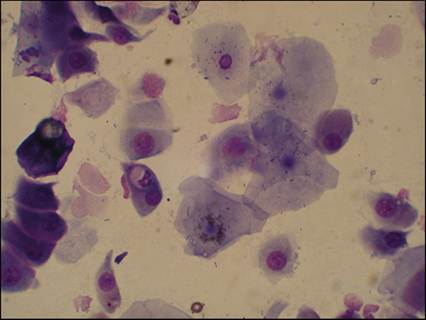
Figure 13.1 Oropharyngeal contamination. Large, keratinized and nonkeratinized squamous epithelial cells with low numbers of mixed population extracellular bacteria (normal bacterial flora) obtained from the oropharynx and external nares (Diff-Quik, 500? magnification).
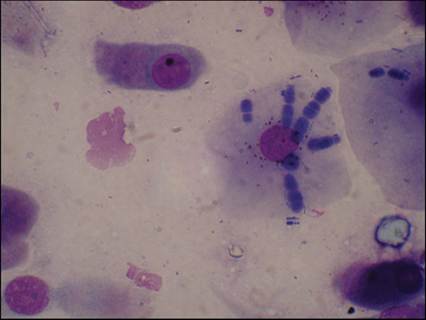
Figure 13.2 Oropharyngeal contamination. A superficial squamous epithelial cell with several Conchiformibius organisms (previously Simonsiella spp.). Conchiformibius spp. are large, rod-shaped bacteria that align in a row after division and indicate that there was oropharyngeal contamination of the sample (Diff-Quik, 1,000? magnification).
Neutrophils are usually absent with oropharyngeal contamination; however, in patients with oral inflammation or dental disease, inflammatory cells may be seen (Figure 13.3). The predominant cell type from the nasal turbinate is typically ciliated columnar respiratory epithelial cells, which appear elongated or cone shaped with eosinophilic staining cilia on their flattened apical ends and a round nucleus present in the basal end of the cell (Figure 13.4). These respiratory epithelial cells can be seen as single cells or in clusters (Figure 13.5). Occasionally, basal epithelial cells may be seen, depending on the collection method used.
These cells are round to cuboidal with scant, deeply basophilic cytoplasm and a round nucleus that is centrally located (Figure 13.6). Mucus appears as eosinophilic amorphous extracellular material, often containing entrapped cells (Figure 13.7). Hemorrhage during sampling is a common occurrence and will result in the presence of red blood cells (RBCs), few white blood cells (WBCs), and sometimes platelet clumps. Iatrogenic contamination of a sample is suspected if the proportion of RBCs and WBCs is similar to that in peripheral blood (approximately 1 WBC per 500–1,000 RBCs) (Burkhard & Millward, 2010; Arndt, 2014). 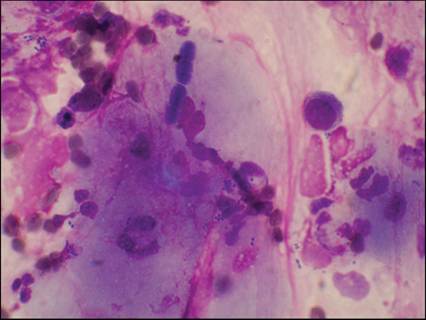
Figure 13.3 Oropharyngeal contamination with inflammation. Neutrophilic inflammation in the presence of oropharyngeal contamination can make it difficult to determine the origin of the inflammation. Inflammatory cells, specifically neutrophils, may be seen in patients with oral inflammation or dental disease (Diff-Quik, 1,000? magnification).
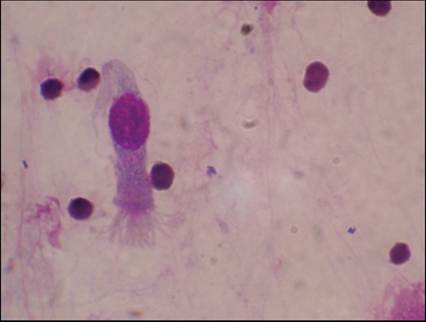
Figure 13.4 Respiratory epithelial cell. The predominant cell type from the nasal turbinates is typically ciliated columnar respiratory epithelial cells, of which one can be seen in this picture. They appear elongated or cone shaped with eosinophilic staining cilia on their flattened apical ends and a round nucleus present in the basal end of the cell (Diff-Quik, 1,000? magnification).
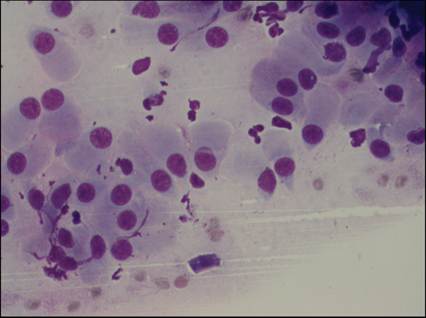
Figure 13.5 Nasal respiratory epithelial cells. Clusters of normal nonciliated respiratory epithelial cells from the nasal cavity (Diff-Quik, 500? magnification).
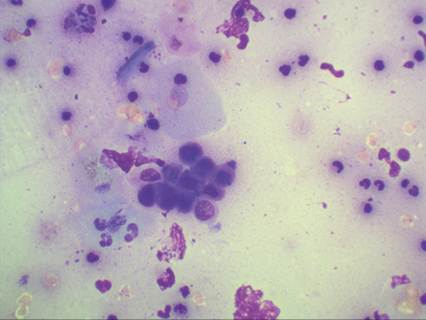
Figure 13.6 Basal epithelial cells. A group of basal epithelial cells, commonly seen as sheets of small cells with scant, round to cuboidal, deeply basophilic cytoplasm and a round nucleus that is centrally located (Diff-Quik, 500? magnification).
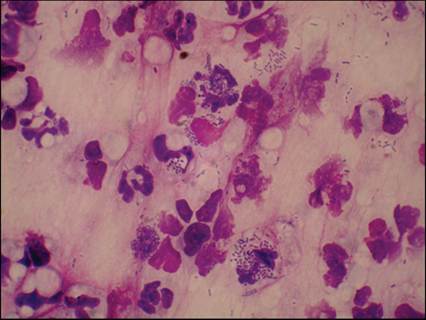
Figure 13.7 Nasal bacterial infection. Neutrophils with phagocytized bacteria indicating a bacterial nasal infection. Some mucus strands are present in the background appearing as eosinophilic amorphous extracellular material, containing entrapped cells (Diff-Quik, 1,000? magnification).