Cases
CASE 1
Signalment/history
A 3.5-year-old, spayed female Jack Russell Terrier with a history of recurrent ear infections. She was adopted by her owners when she was 12 weeks of age and has suffered with ear problems her entire life.
She was noted to have an ear infection the day she was adopted. There is no seasonal improvement or worsening of the clinical signs. The owners also report that the dog’s stools are soft, making it difficult to pick them up, and she will vomit intermittently (approximately once weekly) with no other signs of illness.Physical examination
All abnormal findings are limited to the ears. The concave surface of each pinna is erythematous and swollen, with mild to moderate lichenification and hyperpigmentation, and a malodorous ceruminous scaling and crusting are present (Figure 18.51). The pinnae are sensitive to touch. Otoscopic examination reveals mild hyperplasia of the lining of each ear canal with a moderate amount of light brown ceruminous, malodorous debris clinging to the lining of each ear canal. Each tympanic membrane is intact and normal.

Figure 18.51 Ear pinna from a dog with a history of ear infections and allergies. The pinna is erythematous and swollen with mild to moderate lichenification, hyperpigmentation, ceruminous scaling, and crusting.
Cytology
Cytology samples were collected from the pinna using the tape strip technique and from the ear canals using a cotton tipped applicator (Figure 18.52). Cytology results showed 4+ Malassezia spp. yeast from the left pinna, 1+ Malassezia spp. yeast from the right pinna, 2+ Malassezia spp. yeast from the left ear canal, and 3+ Malassezia spp. yeast from the right ear canal.
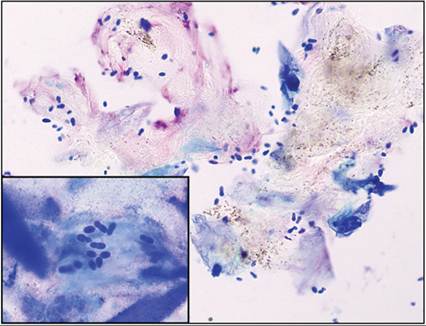
Figure 18.52 Canine ear pinna and canal cytology preparations; Malassezia spp.
dermatitis. Clumps of keratinized epithelial cells with adhered Malassezia spp. yeast are present. Note the small, brown round to rice-shaped melanin granules in the keratinocytes; these should not be mistaken for bacteria. Inset: tape preparation from the same patient showing basophilic keratinocytes with adhered yeast and keratin bars (modified Wright–Giemsa: main, 500? magnification; inset: 1,000? magnification).
Management/outcome
The dog was placed on a strict diet trial using a limited antigen kangaroo and oatmeal diet (Iams Veterinary Formula Skin & Coat Plus Response KO diet) to rule in/out food allergies as a primary or contributing factor in her allergic ear disease. The ear canal infections were treated with topical Posatex Otic Suspension (Merck Animal Health; 1.0% orbifloxacin, 0.1% mometasone furoate monohydrate, and 0.1% posaconazole, otic suspension) in each ear canal (0.2 ml q24h for 21 days). The Malassezia spp. dermatitis of the pinnae was treated by cleaning the pinnae daily with Epi-Otic (Virbac Animal Health; 2.7% lactic acid and 0.1% salicylic acid) ear cleanser on a cotton ball, allowing 2 minutes contact time. The pinnae were then wiped clean and dry using dry cotton balls and then 1–2 drops of Posatex were applied daily for 7 days and then twice weekly for 7 days. Once the infections were cleared, the food trial was continued for another 21 days with weekly ear cleaning of the ear canals as the only treatment.
The ear infections completely resolved with the treatment plan above and did not recur 3 weeks after medications were ceased. On food rechallenge with her previous diet, her pinnae and ear canals became erythematous within 2–3 days, which resolved when the rechallenge was discontinued. The dog has been maintained on the KO diet without further flaring of the clinical signs. Interestingly, the gastrointestinal issues also completely resolved while on the food trial, and flared on food rechallenge.
Discussion
This case illustrates how factors influencing the microenvironment of the ear can predispose individuals to developing Malassezia spp.
yeast overgrowth/infection. In this case, food allergies resulting in inflammation and altered sebum production of the pinnae and ear canal allowed overgrowth of yeasts, which, themselves, are capable of eliciting a hypersensitivity reaction. Eliminating both the yeast infection and the predisposing factor (food allergy in this case) is necessary for clinical resolution (Murphy, 2001).CASE 2
Signalment/history
A 15-month-old, female spayed Maine Coon cat with a 3-month history of a unilateral left ear problem. The cat was adopted from a Maine Coon breeder as a young kitten. She appeared to be healthy at that time. Three months ago the owner noted that the cat appeared to be sensitive when her left ear was touched, and purulent debris was found on otoscopic examination.
Cytology/initial treatment
Ear cytology using a cotton tipped applicator revealed numerous inflammatory cells (4+) and cocci (2+) (Figure 18.53). Tresaderm (Merial; 40 mg thiabendazole, 1 mg dexamethasone, 3.2 mg neomycin/ml of solution) ear medication was prescribed (0.15 ml in the ear daily for 14 days) and the cat appeared to be more comfortable. Neither repeat cytology nor repeat otoscopic examination was performed. Within 2–3 weeks of discontinuing the Tresaderm, the ear infection was documented to have recurred. At the last recheck visit, the cat had been treated with the Tresaderm once again for 14 days, with clinical improvement noted; however, on otoscopic examination, the ear canal remained full of purulent debris. Otic cytology was repeated and numerous inflammatory cells were found with no evidence of infection (no cocci, rods, or yeast found). An inflammatory polyp was suspected and the cat was scheduled for a bulla CT scan, gentle cleaning of the ear canal, and possible traction extraction of the polyp.
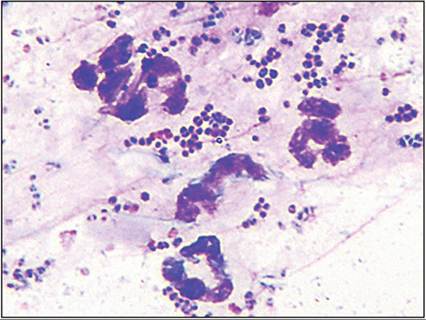
Figure 18.53 Ear cytology from a young adult cat with a history of unilateral ear sensitivity.
Many degenerate neutrophils and myriad cocci are present on a proteinaceous background (modified Wright–Giemsa, 1,500? magnification).
Imaging
On the CT scan, the left ear canal was reported to be full of a soft tissue attenuating structure (Figure 18.54). The structure extended through the tympanic membrane into the middle ear and came in contact with the outer osseous wall of the cochlea. The remainder of the tympanic bulla and the inner ear were normal.
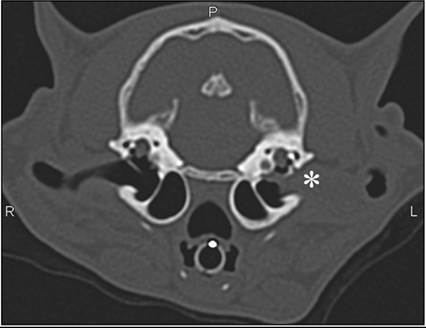
Figure 18.54 Image from a CT scan of a young adult cat with a history of unilateral ear sensitivity. The left ear canal is filled with a soft tissue attenuating structure (asterisk) that extends from the vertical canal into the middle ear. An inflammatory polyp is most likely.
Management/outcome
On otoscopic examination, following gentle removal of the purulent debris from the ear canal, a pink fleshy mass was noted and was removed from the canal using hemostats and traction avulsion. Subsequent histopathologic evaluation of the mass confirmed a nasopharyngeal polyp with lymphoplasmacytic inflammation (Figure 18.55).
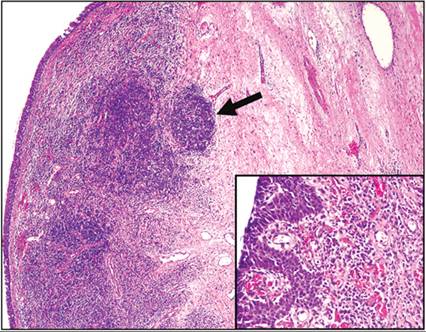
Figure 18.55 Section of a mass retracted from the ear canal of a cat; nasopharyngeal polyp. The mass is composed of fibrous connective tissue lined by pseudostratified to cuboidal epithelium. Multifocal aggregates of lymphocytes are present and occasionally form follicles (arrow). Inset: below the pseudostratified epithelium, a mixed inflammatory infiltrate is present. Lymphocytes predominate, but lesser numbers of plasma cells, macrophages, and neutrophils are also present as are many vascular structures (H&E: main, 40? magnification; inset: 200? magnification).
Immediately following the procedure, the cat was placed on oral prednisolone at a tapering dose for 8 weeks: 2 mg/kg daily for 14 days, 1 mg/kg daily for 14 days, 0.5 mg/kg daily for 14 days, and 0.5 mg/kg on alternate days for 14 days.
She was rechecked at 1 week, 6 weeks, 3 months, and 1 year post-removal of the mass and has recovered without incident. She is playful, interacts with the family, and shows no evidence of recurrence of the polyp.Discussion
In this case, the species, age (young), and recurrent, unilateral nature of the clinical signs should all lead to suspicion of an underlying lesion, most likely an inflammatory polyp. While inflammatory polyps can often be visualized by otoscopic or oropharyngeal examination, advanced imaging can also be helpful for evaluation of middle ear involvement and therapeutic planning (traction avulsion versus ventral bulla osteotomy). Although recurrence may be more likely with traction avulsion, many clinicians prefer this simpler approach and reserve ventral bulla osteotomy for cases in which there is middle ear involvement or with recurrence following traction avulsion. Use of corticosteroids may decrease the risk of recurrence (Fan & de Lorimier, 2004).
CASE 3
Signalment/history
An 11.5-year-old, neutered male American Cocker Spaniel with a long history of ear and skin problems related to atopic otitis/dermatitis. His skin allergy signs are well controlled with oral cyclosporine (5 mg/kg) daily and a limited antigen venison and potato diet (Hill’s Prescription Diet d/d Canine Skin Support Potato & Venison Formula); however, his ears still flare from time to time, usually after he is boarded. Approximately 6 weeks ago, the owner noted a small mass on the left pinna. At first the dog was not bothered by the mass, but the owner is concerned because the mass is increasing in size and is more red and irritated than previously noted. Now it does seem to bother the dog, and he will scratch at the left pinna and occasionally bleeding from the growth is noted.
Physical examination
On physical examination, other than the mass on the pinna, there is no evidence of inflammation or infection involving the ears. A 3.5 ? 2 cm mass is located on the concave surface of the left pinna, just before the entrance to the external ear canal (Figure 18.56).
The mass is multilobulated, malodorous, eroded, and exudative with necrotic tissue and a cream colored substance/exudate. 
Figure 18.56 Concave surface from the ear pinna of a dog; carcinoma. A large, fleshy, erythematous and multilobulated mass is present near the entrance to the external ear canal. Erosions and surface exudation are present on the mass and erythema in the surrounding tissues is also noted.
Cytology
Cytologic findings based on FNA of the mass reported carcinoma with ceruminous adenocarcinoma being a strong consideration given the location, although no secretory material was observed (Figure 18.57).
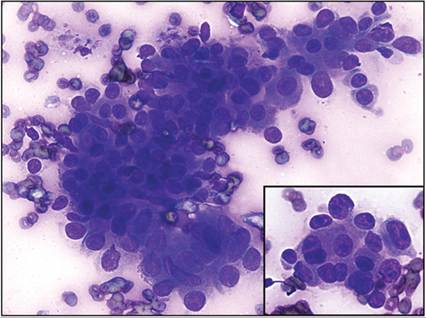
Figure 18.57 Cytology of a mass from the ear pinna of a dog; carcinoma. Clusters of deeply basophilic and jumbled epithelial cells are present. Cells exhibit mild to moderate anisocytosis and anisokaryosis, have a high and variable N:C ratio, and moderately basophilic cytoplasm. Nuclear molding is noted. Inset: cells have large, oval, deeply basophilic nucleoli. Although no material suggestive of glandular secretions is present, given the location, a ceruminous adenocarcinoma would be the top consideration (Wright–Giemsa, 500? magnification).
Management/outcome
The mass was surgically removed. Histopathologic evaluation reported a poorly differentiated carcinoma with nine mitotic figures/10 hpf and 6 mm lateral by 1.5 mm deep margins. The owners declined further staging or treatment concerning the neoplasm. At 6-month follow-up, the dog continued to do well, with no recurrence of the mass noted, and his allergies remained well controlled.
Discussion
This case illustrates the critical role cytology plays in the clinical evaluation of mass lesions. Although evaluation of the cytology preparation did not allow for specific identification of the neoplasm type, the mass could be identified as a carcinoma, which is helpful in planning for the removal of the mass and additional diagnostics (staging, declined in this case). In this particular case, histopathology was also unable to specifically identify the type of carcinoma, but still provided valuable information regarding surgical margins and mitotic index, a measure of tumor proliferation.