Cytology
Cytologic examination of lesions of the external ear can be very useful to determine whether the process is inflammatory or neoplastic and, in many cases, can elucidate the etiology.
Pinna and periauricular area
Inflammatory lesions
Inflammatory lesions of the external ear may be infectious or sterile. As with any other location, the absence of detectable etiological agents on cytology does not rule out infection.
Infectious inflammation
A wide range of infectious agents may potentially be seen on smears from lesions of the pinna and periauricular area. Malassezia dermatitis is a common contributing factor to the clinical signs of pinnal pruritus in dogs, less commonly in cats, suffering from atopic otitis or other concurrent dermatoses. Canine leproid granuloma and leishmaniasis are two other infectious diseases with a predilection for the pinna. Other organisms that may be seen rarely on cytology of pinnal lesions from cats or dogs include yeasts such as Blastomyces dermatitidis, Cryptococcus spp., Histoplasma capsulatum, Sporothrix schenckii, other opportunistic fungi (Figure 18.7), protozoa including Neospora caninum, Toxoplasma gondii, Trypanosoma cruzi, the mites Demodex, Sarcoptes, and Notoedres cati (N. cati is seen exclusively in cats), and dermatophyte infections, which are often present elsewhere in the skin as well. The cytologic appearance of selected lesions is described below. Otodectes cynotis ear mites are discussed in the ‘Ear Canal’ section.
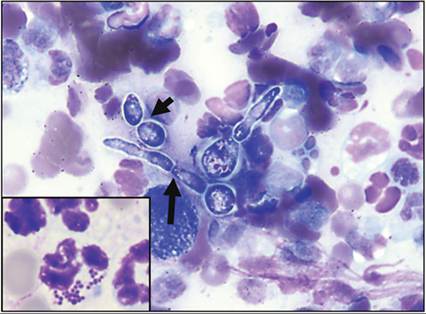
Figure 18.7 Intact papule on the pinna of a dog on immunosuppressive therapy; opportunistic fungal infection. Fungal elements including round yeasts chained together in pseudohyphae (short arrow) and true septated hyphae (long arrow) are present on a background of macrophages and degenerate neutrophils.
Inset: cytology of a ruptured and draining papule revealed only degenerate neutrophils and a secondary bacterial infection. If possible, always sample intact (nonruptured/ulcerated) lesions (Wright–Giemsa, 1,000? magnification; inset: modified Wright–Giemsa, 1,000? magnification).
Malassezia dermatitis
Malassezia spp., most commonly Malassezia pachydermatis, are yeast organisms that can cause significant pinnal pruritus with or without ear canal involvement. The concave surface of the affected pinna is commonly erythematous, greasy or waxy (ceruminous), scaly (yellow or slate gray), crusty, and malodorous. Mild to moderate lichenification and thickening of the affected pinna may be noted, depending on chronicity (Figure 18.8). The lesions may be localized to one or both pinna, or may be generalized, affecting other parts of the animal, including the ear canals, lips, ventral neck, axillae, groin, interdigital skin, perianal area, and intertriginous areas that are warm and moist. The development of clinical signs is more common in the highly humid months, corresponding with the peak of the allergy season, but may persist into the winter. Malassezia dermatitis is a hypersensitivity reaction; therefore the clinical response is not related to the number of yeast organisms present but, rather, to the patient’s reaction to them (Chen & Hill, 2005).

Figure 18.8 Canine inner surface of the ear pinna; gross appearance of Malassezia dermatitis. The pinna is erythematous with prominent scaling, thickening, and lichenification.
Tape strip sample collection is usually the most useful technique, causing the least irritation to the inflamed pinna. However, if the affected skin on the pinna is markedly exudative with thick ceruminous debris present, a dulled scalpel blade or spatula may be used to collect the debris and smear it onto a glass slide.
In the authors’ experience, the latter may cause significant irritation to the pinna, resulting in considerable self-trauma to the sampled pinna. The tape strip sample (stained in jar 3 of Romanowsky rapid stain only) or the smeared stained glass slide will reveal basophilic stained yeast ranging in size from 2.0 ? 4.0 μm up to 6.0 ? 7.0 μm. Malassezia yeast exhibit unipolar budding resulting in ‘snowman’, ‘peanut’, or ‘footprint’ type shapes. Inflammatory cells, most commonly neutrophils, may or may not be present, but are not a common feature of Malassezia dermatitis.Leishmaniasis
Leishmania (Leishmania) infantum and Leishmania (Leishmania) donovani are protozoal parasites that can cause severe disease in dogs. L. infantum is also an important zoonotic disease. Canine leishmaniasis is endemic in Europe, Africa, South America, and Asia, and cases have been specifically reported in foxhounds in North America, as well as in imported dogs in nonendemic areas (Duprey et al., 2006; Cleare et al., 2014). Infection with Leishmania spp. can result in a spectrum of diseases, the manifestations of which depend on the interplay of parasite and host factors. The intermediate hosts of Leishmania are several genera of sandflies. Dogs with clinical leishmaniasis commonly have cutaneous lesions, with a predilection for more sparsely haired areas such as the muzzle and the pinna (Figure 18.9). This predilection is thought to be attributable to the biting preferences of the sandfly. Pinnal lesions range from a silvery scale with alopecia, to ulcers and, much less commonly, nodules. Lesions may be on one or both ears (Cleare et al., 2014). Leishmania (Leishmania) mexicana can cause cutaneous disease in dogs and cats, including reported cases of pinnal lesions in cats in Texas where it is endemic (Trainor et al., 2010). Leishmania (Viannia) braziliensis is another species which causes cutaneous lesions in dogs and cats (Brilhante et al., 2019; Rivas et al., 2018). Other Leishmania species may also sporadically cause cutaneous lesions including of the pinna in dogs and cats.

Figure 18.9 Gross appearance of leishmaniasis. Left: ear pinna of a dog; concave surface, with alopecia, erosion, ulceration, depigmentation, and hyperpigmentation. Right: ear pinna from a cat; convex surface, showing alopecia and crusting. (Courtesy Dr. Guadalupe Miro.)
Impression smears of the exudate overlying ulcerated lesions or aspirates of the nodules typically reveal a mixed inflammatory cell population with a variable amount of hemodilution. There are macrophages with variable numbers of lymphocytes, plasma cells, and nondegenerate neutrophils. A superficial and opportunistic bacterial infection may also be seen, with predominantly cocci; some degenerate neutrophils may accompany the infection and may be seen containing phagocytized bacteria. Variable, but typically low, numbers of protozoal amastigotes are seen phagocytized by macrophages and free in the background. They are ovoid to tapered organisms, approximately 3–6 ? 1.5–3.0 μm in size, with a central dark nucleus, rod-shaped kinetoplast, and pale basophilic cytoplasm (Figure 18.10).
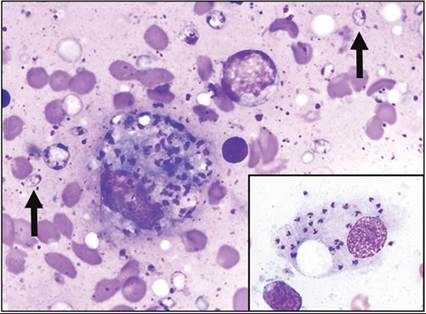
Figure 18.10 Touch imprint of an ulcerated mass on the right pinna of a cat; leishmaniasis. A large macrophage filled with amastigote forms of Leishmania is present on a background of protein, RBCs, and cellular debris. The organisms have a larger oval nucleus and a perpendicular, smaller, rod-shaped kinetoplast giving the image of a person hanging from a parachute. Free organisms are also noted in the background (arrows). In this case, the infection was confirmed as L. mexicana via RNA gene sequencing (modified Wright–Giemsa, 1,000? magnification). Inset: tissue from a foxhound, infected with L. infantum. A large macrophage containing amastigotes is present (Wright–Giemsa, 1,000? magnification).
(American Society of Veterinary Clinical Pathology: Mystery Slide Conference, 2014, Case 8, submitted by Dr. Holly Minard.)
Histologically, the pattern of the inflammation within the dermis varies, but a perivascular pattern is seen most frequently. The inflammation is pyogranulomatous to granulomatous, with macrophages and variable numbers of nondegenerate neutrophils, lymphocytes, and plasma cells. Amastigotes may be difficult to see on routine hematoxylin and eosin (H&E) staining: Giemsa stains will highlight the organisms. Leishmania amastigotes are approximately 3 μm in diameter, with a dark central nucleus, rod-shaped kinetoplast, and pale eosinophilic cytoplasm. They may be seen free in the dermis admixed within the inflammatory infiltrates, or phagocytized within macrophages. Although the detection of amastigotes is specific for leishmaniasis, the sensitivity of detection on histopathology is quite low. Polymerase chain reaction (PCR) assay of tissues or aspirates of lymph node, spleen, or bone marrow, or immunohistochemistry of biopsies of skin lesions are the recommended diagnostics where cytology and histopathology are negative (Cornegliani et al., 2005; Giunchetti et al., 2006; Cleare et al., 2014; Koutinas Koutinas, 2014).
Mycobacteriosis
A dog-specific infection of the pinna is canine leproid granuloma. Canine leproid granuloma is a typically asymptomatic disease caused by multiple mycobacteria of the Mycobacterium simiae-related group (Hughes et al., 2000). They are not considered zoonotic. These mycobacteria are slow-growing organisms that cause the formation of one or more firm alopecic nodules on or around the pinnae, especially on the dorsal fold of the ear (Malik et al., 1998). The lesions may be ulcerated (Figure 18.11). Leproid granulomas are most frequently seen in Boxers and other short-coated breeds (Malik et al., 1998). Biting flies are thought to transmit the bacteria, hence the predilection for the pinna and the more frequent occurrence in short-coated dog breeds (Smith, 1973).
class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7426/image/image1007.jpg" alt=fig18.11.jpg>
Figure 18.11 Dorsal fold of the ear of a dog; gross appearance of leproid granulomas. A larger, partially alopecic nodule and a smaller ulcerated nodule are present. (Courtesy Dr. Frane Banovic.)
Aspiration of the nodules reveals a variably cellular, mixed inflammatory cell infiltrate of epithelioid macrophages, plasma cells, lymphocytes, neutrophils, and binucleate macrophages and multinucleate giant cells (Figure 18.12). Epithelioid macrophages are macrophages with abundant pale basophilic cytoplasm and a small eccentric nucleus with a small prominent nucleolus; as the name indicates, they possess similarities to epithelial cells. The cytoplasm of epithelioid macrophages and giant cells contains clear and refractile (negative staining) rod-shaped bacteria; free bacilli may also be seen within the background (Twomey et al., 2005). Mycobacteria are negative staining because their lipid cell wall resists Romanowsky-type stains (Malik et al., 1998). Organism numbers vary from few to many. Acid-fast stains may be applied to air-dried and unstained smears to highlight the mycobacteria. Alternatively, stained slides that are suspect but negative may be destained and then stained with acid-fast stain (Marcos et al., 2009).
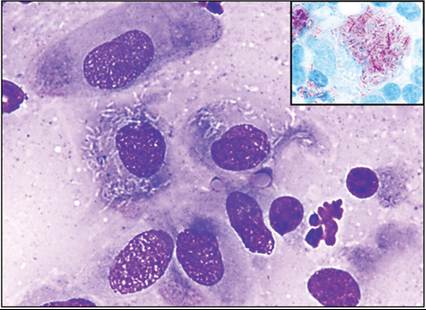
Figure 18.12 Aspirate of a lesion on the pinna of a dog; mycobacteriosis. Epithelioid macrophages contain nonstaining bacilli. A few free bacteria are also noted in the background (modified Wright–Giemsa, 1,000? magnification). Inset: note the characteristic acid-fast staining of the organisms. Acid-fast staining may be performed on unstained or destained cytology preparations (acid-fast stain, 1,000? magnification). (Courtesy Dr. Valarie Pallatto.)
Histologically, the lesions are located in the dermis and/or subcutis and are composed of sheets of epithelioid macrophages, neutrophils, fewer lymphocytes and plasma cells, and variable numbers of multinucleate giant cells. The inflammatory cell population often forms poorly circumscribed granulomas or pyogranulomas (Figure 18.13). The cytoplasm of macrophages and giant cells contains bacilli that are negative staining and often difficult to identify on H&E stains, but are readily stained by modified acid-fast stains such as Fite stain or Ziehl–Neelsen stain (Malik et al., 1998; Foley et al., 2002).
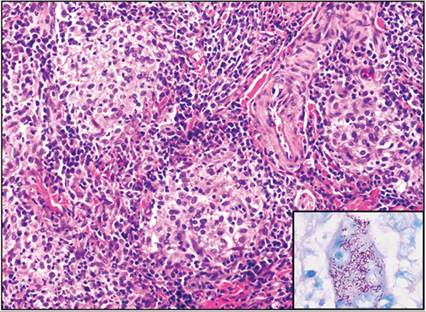
Figure 18.13 Haired skin from the pinna of a dog; leproid granuloma. Multiple small nodules composed of epithelioid macrophages are present and are surrounded by fewer neutrophils, lymphocytes, and plasma cells (H&E, 200? magnification). Inset: a multinucleate giant cell filled with phagocytized acid-fast bacilli (acid-fast stain, 1,000? magnification).
The lesions usually spontaneously regress within weeks to months, although some may require treatment with surgical excision and/or anti-mycobacterial antibiotics (Malik et al., 1998; Foley et al., 2002). Where leproid granuloma is suspected but organisms cannot be identified on cytology or histopathology, mycobacterial PCR can be performed on Romanowsky-stained aspirate smears (not acid-fast stains) or on formalin-fixed, paraffin-embedded tissues (Reppas et al., 2013).
Sterile inflammation
A variety of noninfectious conditions can cause inflammatory lesions on the pinna or periauricular region of cats and dogs. Due to the sparseness of hair, the pinnae are frequent targets of insect bites from flies (e.g. Stomoxys calcitrans) in dogs and mosquitoes in cats (Figure 18.14).
Nodular lesions may result. Cytologically, insect bites are characterized by a mixed inflammatory population, which is dominated by small and mature lymphocytes, with variable numbers of plasma cells in chronic lesions, and also eosinophils, which are usually predominant in mosquito bites (Nagata & Ishida, 1997). In mosquito bite hypersensitivity, free eosinophil granules may be present in the background (Power & Ihrke, 1995). Variable numbers of mast cells (especially with mosquito bites), neutrophils, and macrophages may be seen. Increased numbers of neutrophils are expected, particularly where there is ulceration and secondary infection.
Aural hematomas are frequently seen in dogs and, less commonly, in cats. They often form subsequent to head shaking due to otitis externa or the presence of a foreign body within the ear canal. Damage to auricular blood vessels results in hemorrhage between the cartilage layers or between the skin and cartilage, forming a pocket (Dye et al., 2002). Aspirates contain a dense pale eosinophilic proteinaceous background with large numbers of free erythrocytes, with macrophages containing phagocytized erythrocytes and, in subacute to chronic lesions, macrophages containing gold/brown granular pigment consistent with hemosiderin (Figure 18.15). Variable neutrophilic inflammation may accompany the erythrocytes, and an occasional plump spindle cell may be seen. Removal of the inciting cause and drainage and correction of the hematoma are indicated (Joyce Day, 1997).

Figure 18.14 Ear pinna from a cat; gross appearance of mosquito bite hypersensitivity. One large and two smaller regions of ulceration are present. Due to the thinness of the hair in this region, the ear pinnae are often affected by insect bites.
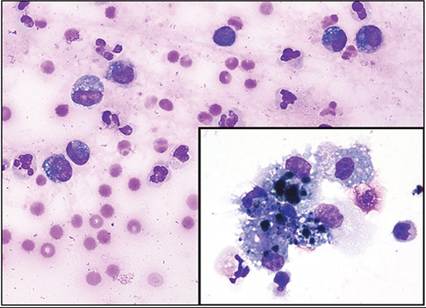
Figure 18.15 Fluid drained from the ear pinna of a dog; acute hemorrhage, aural hematoma. Many RBCs are present on a pale pink, hemolyzed background. Inflammatory cells consisting of a mix of nondegenerate neutrophils and vacuolated macrophages are also noted. In this particular case, erythrophagia is not appreciated. Grossly, the sample was hemorrhagic and failed to clot when drained. The fluctuant mass appeared 2 days previously and developed due to head shaking in response to otitis externa (Wright–Giemsa, concentrated direct preparation, 700? magnification). Inset: in this sample, coarsely clumped blue–black material within macrophages is consistent with hemosiderin and indicates an older lesion (Wright–Giemsa, 1,500? magnification). (Courtesy Dr. Ann Barger.)
Other less common sterile lesions of the pinna and periauricular region include:
· Eosinophilic plaques or granulomas, especially in cats. Lesions are composed of mainly eosinophils with accompanying nondegenerate neutrophils, macrophages, lymphocytes, plasma cells, and occasional mast cells (Bloom, 2006).
· Para-auricular abscesses can form secondary to any cause of ear canal stenosis (Rogers, 1988). Cytologically, they are composed of variably degenerate neutrophils, occasional macrophages, and anucleate squamous epithelial cells. Bacteria may be present if there is a secondary infection.
· Sterile granulomas and pyogranulomas in dogs or cats, which contain macrophages and accompanying rare to frequent neutrophils with fewer small lymphocytes and plasma cells (Santoro et al., 2008). A thorough search for mycobacteria, Leishmania, and fungal organisms, including dermatophytes, is always indicated in such lesions, and special stains, cultures, and PCR may also be indicated.
· Feline relapsing polychondritis is a rare disease of cats that results in swollen, curled, and painful pinnae. It is thought to be an autoimmune reaction to the auricular cartilage resulting in necrosis and inflammation. Cartilage in other locations may also be affected (Delmage & Kelly, 2001; Gerber et al., 2002; Baba et al., 2009). Cytologic findings have not been reported but a mixed inflammatory cell infiltrate is expected.
· Frostbite, cold agglutinin disease, and vasculitis may also manifest on the tips of the pinnae.
· Systemic dermatitides such as immune-mediated, hormonal, or allergic skin diseases may also have pinnal or periauricular foliaceus. Immune-mediated diseases such as pemphigus foliaceous, pemphigus vulgaris, erythema multiforme, lupus erythematosus, dermatomyositis, bullous pemphigoid, sebaceous adenitis, and vasculitis can be seen in this region as well as elsewhere in the skin. They may present as alopecic, papular, vesicular, or ulcerated lesions. Multiple biopsies and histopathology are required for diagnosis. Hypothyroidism and hyperadrenocorticism may cause pinnal alopecia. Allergic skin disease such as atopic dermatitis, food allergy, or, rarely, contact allergy can cause alopecia, erythema, scale, or crusting lesions. In the absence of a secondary infection, cytology of suspected allergic skin disease is generally not very rewarding, typically yielding only keratinocytes and, occasionally, melanin laden cells (due to the associated hyperpigmentation). Eosinophils are only very rarely seen (KMM, personal experience).
Neoplasia and non-neoplastic mass lesions
Neoplasms of the pinnae and periauricular regions appear similar to those seen elsewhere in the skin. Metastasis to the ear appears to be very uncommon (Sula, 2012). The most common tumors seen in this region are (Bostock & Dye, 1979; Roth, 1990; Sula, 2012):
· Round cell: histiocytoma, mast cell tumor, plasmacytoma, lymphoma, melanoma, melanocytoma.
· Epithelial: SCC, cutaneous basilar neoplasm, sebaceous adenoma, sebaceous epithelioma, sebaceous carcinoma, papilloma.
· Mesenchymal: hemangioma, hemangiosarcoma, fibrosarcoma, feline sarcoids.
· Non-neoplastic mass-like lesions of the pinnae include ceruminous and sebaceous hyperplasia (see ‘Ear Canal’) and feline ceruminous cystomatosis. Feline ceruminous cystomatosis is a benign cystic proliferation of the ceruminous glands of the inner pinna and external ear canal. The cystic component contains brown inspissated material, which may fill the ear canal. They are grossly seen as proliferative blue/brown masses. Cytologically, the fluid is proteinaceous and basophilic (Figure 18.16), and cholesterol crystals, anucleate squamous epithelial cells, and vacuolated macrophages may be seen (Corriveau, 2012). For a description of ceruminous gland neoplasms, see ‘Ear Canal’ and ‘Neoplasia and Non-Neoplastic Mass Lesions’.
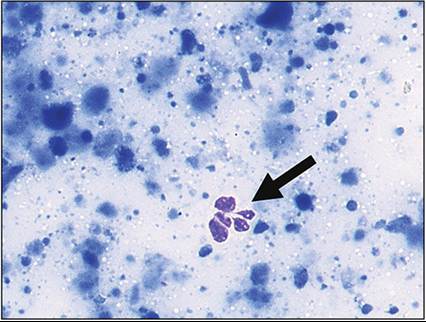
Figure 18.16 Cytologic appearance of feline ceruminous cystomatosis. The lesion is characterized by basophilic, proteinaceous fluid, which may form dense aggregates. Note the single ruptured neutrophil (arrow) (modified Wright–Giemsa, 800? magnification). (Courtesy Dr. Rebekah Gunn-Christie.)
Dentigerous cysts and dermoid cysts are lesions that may rarely be seen in the periauricular region (Sula, 2012). Dentigerous cysts contain fluid, which may be variably basophilic on smears, and there may be low numbers of vacuolated macrophages and anucleate or nucleated squamous epithelial cells (Poulet et al., 1992). Dermoid cysts are congenital epidermal inclusion cysts, so cytology comprises large numbers of anucleate squamous epithelial cells and associated squamous debris (Tolbert et al., 2009).
Round cell neoplasms
Histiocytoma
Histiocytomas are benign tumors of Langerhans cells, a subtype of histiocytes located in the skin. Histiocytomas typically present as a single circular, dome-shaped, and variably alopecic mass. They have a predilection for the pinna, with most arising on the head or extremities. Young dogs less than 3 years of age are typically affected, although they may be seen in dogs of any age. This neoplasm has not been reported in cats. Cytologically, aspirates are usually moderately to highly cellular and contain large numbers of monotypic medium-sized round cells with an eccentric round to ovoid nucleus, fine chromatin, usually no distinct nucleoli, and a pale gray/blue cytoplasm with often a clearing at the periphery of the cell (Figure 18.17). Binucleate and multinucleate cells and mitotic figures are typically rare. Variable numbers of small and mature lymphocytes may also be seen admixed. Lymphocytic infiltration (T cells) is often a harbinger of imminent regression of the neoplasm. Histologically, the lesion is a nodule composed of sheets of medium-sized round cells, which are most dense superficially (‘top heavy’), and often extend to the dermoepidermal junction. Mitotic figures are relatively frequent and variable numbers of small lymphocytes, occasional plasma cells, and neutrophils are interspersed (Taylor et al., 1969).
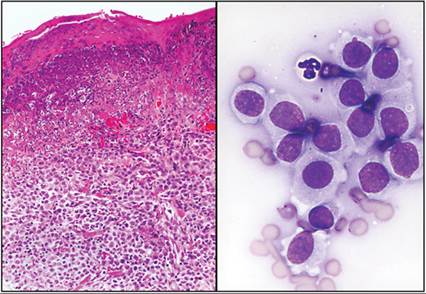
Figure 18.17 Tissue from the pinna of a dog; histiocytoma. Left: the dermis contains an expansile mass composed of sheets of medium-sized round cells. The round cells are uniform in size and have round to ovoid to reniform nuclei with pale eosinophilic cytoplasm (histiocytes). There are also very occasional small lymphocytes and neutrophils admixed. The overlying epidermis is ulcerated with an accompanying neutrophilic inflammatory response and an adherent serocellular crust (H&E, 200? magnification). Right: the classic cytologic appearance of a histiocytoma; note the pale cytoplasm, which tends to stain paler toward the outer edge of the cell, and the ruffled cytoplasmic border (modified Wright–Giemsa, 1,000? magnification).
Cutaneous plasmacytoma (plasma cell tumor)
Cutaneous plasmacytoma or plasma cell tumor is another round cell neoplasm that has a predilection for the pinnae in dogs. They are rare in cats. Plasmacytomas have a similar gross appearance to histiocytoma. Smears from FNAs are usually highly cellular with large numbers of round cells. The round cells typically possess a moderate nuclear to cytoplasmic (N:C) ratio and cells may exhibit moderate anisocytosis and anisokaryosis (Figure 18.18). The nucleus is round and eccentric with a variable chromatin pattern depending on the maturity of the cells: stippled, slightly open, or finely clumped. Nucleoli are usually not apparent. The cytoplasm is moderately to densely basophilic and cells may have a clear region next to the nucleus (perinuclear clearing or Golgi zone). In some tumors, the periphery of the cytoplasm may contain bright eosinophilic material, which may also be present in the background, and is thought to represent immunoglobulin. Binucleate and multinucleate cells and mitotic figures are usually frequent. Despite the pleomorphism and high mitotic rate, plasmacytomas are considered behaviorally benign and cured by complete excision. On histopathology sections, plasmacytoma is an expansile dermal tumor separated from the epidermis by a small area of normal dermal collagen (Grenz zone) composed of sheets of variably pleomorphic round cells, similar to the cytologic appearance described above (Figure 18.19).
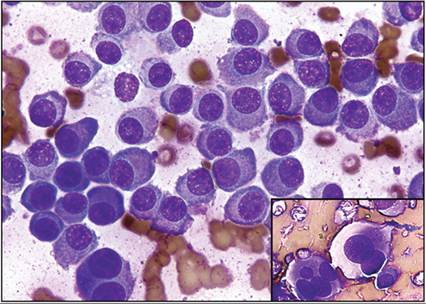
Figure 18.18 Aspirate of an ear mass in a dog; plasmacytoma. This example shows a well-differentiated plasmacytoma; cells have eccentric nuclei, coarse chromatin, basophilic cytoplasm, and variably well-developed Golgi zones. Occasional binucleated cells are present, a typical feature of this tumor type (Wright–Giemsa, 1,000? magnification). Inset: aspirate of a cutaneous mass on the pinna of a dog. As shown here, plasmacytomas can exhibit moderate to marked pleomorphism including marked anisocytosis and anisokaryosis, and multinucleation with varying sizes of nuclei. Despite the greater pleomorphism in this tumor, the expected behavior is benign (modified Wright–Giemsa, 500? magnification).
alt=fig18.19.jpg>
Figure 18.19 Ear mass from a dog; plasmacytoma. An expansile nodule present in the dermis is composed of sheets of plasma cells, separated from the epidermis by a thin strip of normal dermal collagen, known as a Grenz zone. Inset: the plasma cells exhibit mild anisocytosis and anisokaryosis with frequent binucleate and multinucleate cells. Despite these features, cutaneous plasmacytomas are typically behaviorally benign (H&E: main, 200? magnification; inset, 400? magnification).
Mast cell tumor
Mast cell tumors may be found on the pinnae of dogs and cats. Grossly, they can be nodular or plaque-like and variably alopecic. In the cat, solitary lesions are usually behaviorally benign and cured by complete excision (Molander-McCrary et al., 1998). Multiple lesions may suggest disseminated mastocytosis in the cat, an aggressive and malignant syndrome (Sabattini & Bettini, 2010). In dogs, pinnal mast cell tumors are considered more aggressive than cutaneous mast cell tumors elsewhere, with a relatively high metastatic rate (Higginbotham et al., 2000). Cytology of mast cell tumors is usually very cellular with large numbers of medium-sized round cells. The round cells have large numbers of dark purple round granules within the cytoplasm, which often obscure the cytoplasmic and nuclear detail. Where the nucleus can be seen, it is round with fine chromatin and typically no obvious nucleoli. Particularly in dogs, there are often variably low to high numbers of accompanying eosinophils. Free mast cell and eosinophil granules may be abundant in the background. There may also be collagen in the background, which stains palely to brightly eosinophilic (Figure 18.20). A proposed two-tier cytologic grading scheme for canine dermal mast cell tumors outlines criteria for a designation of cytologic high-grade with cytologic features of poor granulation (using Wright–Giemsa stain), or at least two of: mitotic figures, nuclear pleomorphism, bi- and multinucleation, and 50% variation in nuclear size (Camus et al., 2016) (Figure 18.21). Although not yet widely validated, use of this grading scheme is becoming more common as veterinarians may use it for treatment planning. The Oncology-Pathology Working Group suggests caution in classifying tumors as cytologic high grade if only two criteria are used and one of them is nuclear pleomorphism or anisokaryosis, since this may overclassify mast cell tumors as high grade compared to histopathologic grading (Berlato et al., 2021).
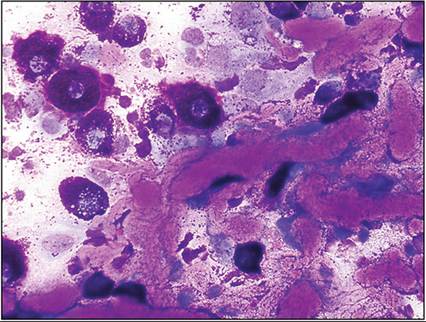
Figure 18.20 Canine skin mass; mast cell tumor with abundant collagen. Many thick, linear stands of palely to brightly eosinophilic and slightly fibrillar/granular collagen strands are admixed with well-differentiated mast cells and eosinophils. Collagen strands are occasionally seen in variable numbers in aspirates of mast cell tumor. This mast cell tumor would be consistent with a designation of cytologic low-grade (Camus et al., 2016) (Wright–Giemsa, 600? magnification).
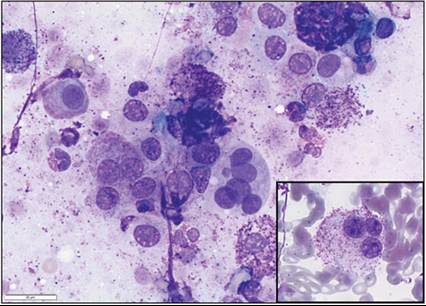
Figure 18.21 Dermal mass on the pinna of a dog; mast cell tumor with multiple criteria of malignancy (consistent with a designation of cytologic high-grade per Camus et al., 2016). Mast cells are variably granulated, exhibit marked anisocytosis and anisokaryosis, with binucleate and multinucleate cells. Grading of this mass on histopathology was grade 2 (Patnaik) high grade (Kiupel) (Patnaik et al., 1984; Kiupel et al., 2011) (modified Wright–Giemsa, 600? magnification).
In cats, cutaneous mast cell tumors may be classified as mastocytic (appearance typical as for mast cells) or atypical/histiocytic. The atypical/histiocytic subtypes are often reported in young Siamese cats and are poorly granular, appearing more similar to histiocytes than typical mast cells (Figure 18.22).
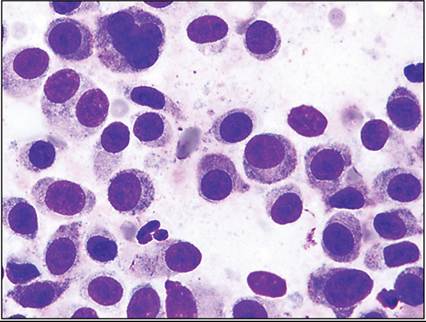
Figure 18.22 Mass on the lateral margin of the ear pinna of a 3-year-old Siamese cat; atypical mast cell tumor. These round cells are poorly granulated with only occasional cells showing a few well-delineated fine purple granules. Note the large multinucleated cell at the top of the image (Wright–Giemsa, 1,000? magnification). (Courtesy Dr. Robin Allison and Dr. Pi Jie Yang.)
Eosinophils and small mature lymphocytes often are admixed. This subtype may spontaneously regress (Sabattini & Bettini, 2010). The histopathologic appearance of mast cell tumors is somewhat variable, but generally consists of sheets of cells within the dermis (Figure 18.23). Unlike cytology specimens, the granules are fine and gray. Mast cell tumors can usually be confirmed (as long as they have granules) using toluidine blue or Giemsa staining, which stains the mast cell granules bright purple (metachromatic).
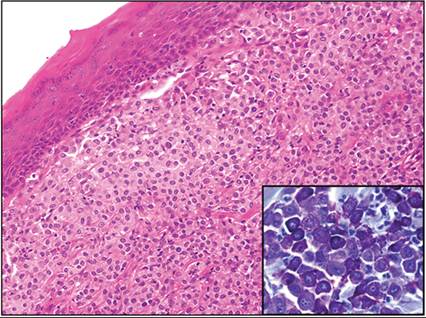
Figure 18.23 Cutaneous mass on the pinna of a dog; mast cell tumor. Extending from below the hyperplastic epidermis throughout the superficial and mid-dermis is a mass composed of sheets of monotypic round cells. The cells exhibit mild anisocytosis and anisokaryosis and possess a round nucleus and pale eosinophilic to finely gray granular cytoplasm (mast cells). There are also occasional scattered eosinophils admixed (H&E, 200? magnification). Inset: toluidine blue staining results in the characteristic bright purple (metachromatic) color of cytoplasmic granules of the round cells, confirming the diagnosis of mast cell tumor (toluidine blue stain, 400? magnification).
Melanocytomas and melanomas
Melanocytomas and melanomas may also be seen on the pinnae, particularly in cats. The majority of feline melanocytic neoplasms are behaviorally benign, but recurrence and metastasis have been reported (Miller et al., 1991; Luna et al., 2000). Lesions may be flattened or nodular, and are often dark brown to black (amelanotic melanomas may be pale pink). The cytology of melanocytic neoplasms is characterized by a moderate to high cellularity specimen composed of round to polygonal to spindled cells. The nucleus is typically round and most often central, with a fine sieve-like chromatin pattern, and small nucleoli may be seen. The cytoplasm is pale basophilic and contains moderate to large numbers of fine, gold to brown to black to blue/green–black granules, consistent with melanin. A differential diagnosis for melanocytic neoplasms is pigmented basal cell tumor or basilar neoplasia. Basal cell/basilar neoplasms are composed of small epithelial cells, which possess a high N:C ratio and form tightly cohesive clusters, compared with melanocytic neoplastic cells, which are discrete cells with a moderate N:C ratio. In more aggressive melanocytic neoplasms, there is pleomorphism, nuclear criteria of malignancy, and reduced granularity of the cells (granules may be entirely absent in aggressive amelanotic melanomas). On histopathology, cutaneous melanocytic neoplasms typically arise in the dermis and form sheets of polygonal to spindled cells. Well-granulated tumors are often so densely pigmented that nuclear and cytoplasmic detail cannot be examined. Pleomorphism, high mitotic rate, reduced granularity, presence of neoplastic melanocytes within the epidermis (junctional activity), and vascular and lymphatic invasion are consistent with more malignant behavior (Smedley et al., 2011).
Cutaneous lymphoma
Cutaneous lymphoma may be seen on the pinnae or periauricular regions of dogs and cats, but this is usually part of systemic disease. The lesions may present as nodules, or as plaques, ulcers, areas of alopecia, or scale (Sula, 2012). Cytologic preparations contain a monomorphic population of lymphocytes. The cytologic appearance varies depending on the subtype: from small to large-sized lymphocytes with a round to irregular nucleus, smooth to clumped chromatin, with or without nucleoli, and pale to deeply basophilic cytoplasm, which may be scant, have indistinct borders (veil appearance), or may be eccentric (hand-mirror or pseudopod). Moderate numbers of variably sized cytoplasmic fragments are often seen in the background. Concurrent ulceration with resultant inflammation or infection may complicate the cytologic picture and necessitate histopathology for diagnosis. As with the cytology, histopathology of cutaneous lymphoma will also vary depending on the subtype, but comprises a monomorphic population of round cells forming sheets. The neoplastic lymphocytes may be positive for CD3 (T cell) or CD79a and CD20 (B cell). The vast majority of feline and canine cutaneous lymphomas are T-cell phenotype; cutaneous B-cell lymphomas are extremely rare (Day, 1995; Ponce et al., 2010).
Epithelial neoplasms
Squamous cell carcinoma
SCC is the most common neoplasm found on the pinnae of cats (Fan & de Lorimier, 2004). The majority are ultraviolet (UV) light-induced, with white cats 13 times more likely to develop pinnal SCC than pigmented cats (Dorn et al., 1971). They may also be seen in the sparsely haired preauricular region, and can also be seen occasionally in dogs (Miller Shanley, 1991). The lesions are usually red, crusted, flattened lesions with ulceration. Scraping of the lesions reveals an often pleomorphic population of medium-sized to large polygonal to elongated cells present singly and in cohesive clusters (Figure 18.24). They have a moderate N:C ratio with variable and often moderate to high anisocytosis and anisokaryosis. The nucleus is round with coarse to open chromatin, often with distinct nucleoli, and the cytoplasm is pale to moderately basophilic (described as sky or robin’s egg blue) and hyaline. Fine pink granules (keratohyalin granules) may be seen in the cytoplasm. Very large cells with large prominent nucleoli, binucleate and multinucleate cells, and atypical mitotic figures may be seen. Frequently, there are low to high numbers of neutrophils present, and neutrophils may be seen within the cytoplasm of the neoplastic epithelial cells (emperipolesis). Secondary bacterial infection may be seen in ulcerated lesions. Histopathology of SCC is typified by cords, islands, and trabeculae of squamous epithelial cells (Figure 18.25). There is dysmaturation characterized by abrupt cornification within islands forming concentric laminar whorls of eosinophilic keratin (keratin pearls). Pinnal SCCs are typically locally aggressive but infrequently metastasize; thus prognosis with complete surgical excision is fairly good (Lana et al., 1997).
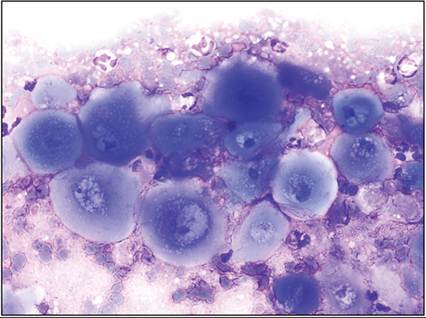
Figure 18.24 Tissue from a dog; squamous cell carcinoma. Many large, pleomorphic, well-keratinized squamous cells are present on a background of blood and mild suppurative inflammation. Cells exhibit moderate anisocytosis and anisokaryosis, have large, pleomorphic nuclei with prominent nucleoli, and exhibit perinuclear vacuolization. Features indicating keratinization include the angular appearance of some of the cells, the pale to deep ‘sky’ or ‘robin’s egg’ blue cytoplasmic color, and the waxy or ground glass appearance of the cytoplasm (Wright–Giemsa, 500? magnification).
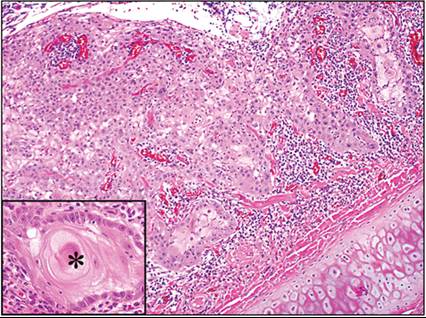
Figure 18.25 Ulcerated mass on the pinna of a cat; squamous cell carcinoma. The dermis is expanded and infiltrated by clusters of epithelial cells forming trabeculae and nests. There are frequent clusters with abrupt keratinization and keratin pearls. There are also moderate numbers of neutrophils and lymphocytes with fewer plasma cells in the surrounding dermis. Note that there is also complete loss of normal epidermis (ulceration) with a partially adherent exudate on the surface. Neoplastic cells do not infiltrate the cartilage. Inset: note the moderate anisocytosis and anisokaryosis in the neoplastic epithelial cell population and the large central area of abrupt cornification with keratin pearl formation (asterisk). There are mixed inflammatory cells in the surrounding dermis (H&E: main, 100? magnification; inset, 400? magnification).
Cutaneous basilar neoplasm (‘basal cell tumor’)
Cutaneous basilar neoplasms or basal cell tumors are morphological umbrella terms encompassing neoplasms of the germinal cells of the hair follicle and adnexal structures. These neoplasms may be classified as to the tissue of origin on histology, e.g. trichoblastoma for hair follicle origin and ductular adenoma as apocrine (sweat) gland origin. However, it is usually not possible to determine the tissue of origin on cytology, hence the common use of the umbrella terms. Basal cell tumors are the most common cutaneous neoplasm in the cat and are often seen on the head and neck, including the pinnae and periauricular region (Miller et al., 1991). Basilar neoplasms may also be seen in dogs. They are typically seen as solitary nodules. FNAs yield moderately to highly cellular smears composed of tightly cohesive clusters of uniform small epithelial cells. Some cells may be present in linear arrays. The epithelial cells are round to slightly elongate with a high N:C ratio, a round central or eccentric nucleus, finely clumped chromatin, and basophilic cytoplasm. Nucleoli are usually not apparent (Bohn et al., 2006). The cytoplasm may contain fine, gold to brown to black granules consistent with melanin; therefore a melanocytic neoplasm is a differential for pigmented tumors (Figure 18.26; Stockhaus et al., 2001). Histopathology sections of basilar neoplasia reveal an expansile, dermal mass composed of lobules of small, uniform epithelial cells (Figure 18.27). Cystic areas may be present within the mass (Bohn et al., 2006). Basal cell tumors are usually behaviorally benign but may be locally aggressive (Day et al., 1994). Some basal cell tumors in dogs can grow quite large.
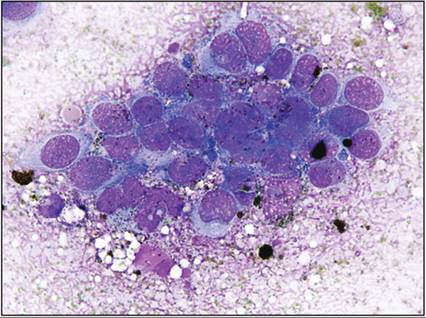
Figure 18.26 Aspirate of a mass on the pinna of a cat; pigmented basal cell tumor/basilar neoplasm. A cluster of mildly pleomorphic epithelial cells is present on a background of protein and free melanin granules. The epithelial cells are medium in size with mild anisocytosis and anisokaryosis. They have round to oval nuclei, visible nucleoli, and a thin rim of moderate basophilic cytoplasm containing variable numbers of melanin granules. Pigmented basilar neoplasms can easily be mistaken for melanoma (Wright–Giemsa, 1,000? magnification).
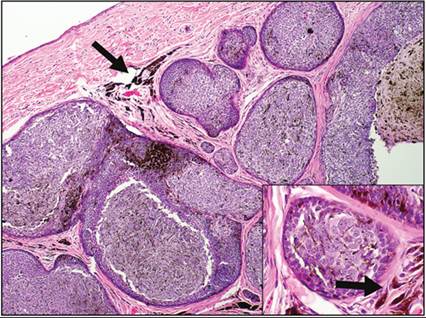
Figure 18.27 Mass on the pinna of the ear of a cat; basilar neoplasm, trichoblastoma. The dermis is expanded by multifocal well-demarcated lobules of uniform epithelial cells. At the periphery of the lobules, the epithelial cells are smaller, more hyperchromatic, and have a high N:C ratio (basilar). Toward the center of the lobule, they are slightly larger, paler, with a moderate to high N:C ratio (parabasal). Many of the epithelial cells contain a small to moderate amount of brown/black granular pigment in the cytoplasm (melanin). Macrophages containing phagocytized melanin (melanomacrophages) are present in the surrounding dermis (arrow). Inset: islands of follicular epithelial cells containing melanin pigment. Note the melanomacrophages (arrow) in the surrounding dermis. These neoplasms are typically cured by complete excision (H&E: main, 100? magnification; inset, 400? magnification).
Sebaceous adenoma/epithelioma/carcinoma
Sebaceous neoplasms may also be seen on the pinnae of dogs and, less frequently, cats. They are most often small, cauliflower-like masses. Aspiration of sebaceous proliferations reveals multiple cohesive clusters of uniform, small to medium-sized epithelial cells, which have uniformly and finely vacuolated cytoplasm. Acinar or tubular structures may be seen, which can contain a central aggregate of amorphous eosinophilic secretory material. The N:C ratio is typically low to moderate, with a central nucleus possessing dense chromatin and no obvious nucleoli. The background is often pale eosinophilic to basophilic, and proteinaceous with scattered clear lipid vacuoles. Sebaceous hyperplasia cannot be differentiated from adenoma on cytology.
Sebaceous epitheliomas also appear similar, although representative smears typically contain a predominance of basal-type epithelial cells (similar to those described above for basal cell and basilar tumors; Figure 18.28). Sebaceous adenocarcinomas are rare, and they often have multiple criteria of malignancy with increased anisocytosis and anisokaryosis, high N:C ratios, multinucleated cells, and prominent nucleoli. There may be few lipid vacuoles in the cytoplasm to indicate their identity (Dickinson & Young, 2005). With sebaceous hyperplasia and adenomas, surgical excision is usually curative and regrowth rare. Adenocarcinoma is more aggressive, invasive, and may metastasize (Scott & Anderson, 1990). On histopathology sections, sebaceous hyperplasia forms lobules of mature, finely vacuolated, sebaceous epithelial cells around a central duct, with a single layer of basal reserve cells. Adenomas are similar, forming solid lobules of sebaceous epithelial cells, while sebaceous epitheliomas have a predominance of basal reserve cells, with multiple areas of sebaceous differentiation. Adenocarcinomas are poorly circumscribed multilobular masses of pleomorphic and atypical epithelial cells, which may have few lipid vacuoles within the cytoplasm (Goldschmidt et al., 1998).
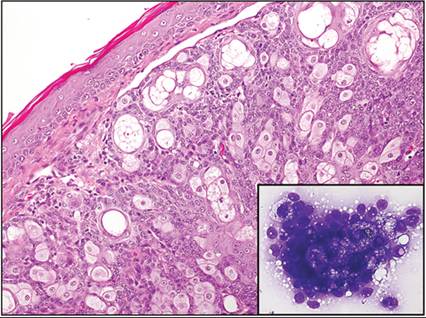
Figure 18.28 Mass on the ear of a dog; sebaceous epithelioma. Expanding the dermis is a densely cellular mass composed of sheets and lobules of polygonal epithelial cells. Epithelial cells are predominantly small and hyperchromatic with a high N:C ratio (basilar cells), that occasionally abruptly differentiate into larger cells with pale foamy cytoplasm, consistent with sebaceous epithelial cells. Frequent ductal differentiation is seen. Occasional mitotic figures are present. The overlying epidermis is unaffected. The predominance of basilar cells is the reason this is diagnosed as a sebaceous epithelioma rather than an adenoma (H&E, 200? magnification). Inset: aspirate from the same tumor showing a cluster of small basophilic basilar epithelial cells with a focus of larger, foamy sebaceous cells at the center (Wright–Giemsa, 500? magnification).
Papillomas
Papillomas are benign neoplasms of the epidermis. They are fairly common in dogs but very rare in cats (Munday et al., 2007). In younger dogs they are often induced by canine papillomavirus and in older dogs they are more often spontaneous (Sula, 2012). They may be nodular or exophytic. Cytology may be variably cellular and contain uniform, small to medium-sized, polygonal to slightly elongated epithelial cells present singly or in clusters. They typically possess a moderate N:C ratio with a central nucleus, finely clumped chromatin, and no obvious nucleoli. The cytoplasm may vary from moderately to palely basophilic, and may be somewhat hyaline or contain pink granules, depending on the stage of keratinization of the proliferating cells. Papillomas caused by papillomavirus typically contain a dusty magenta cytoplasm and may have visible nucleoli. Viral inclusions are usually absent (Sprague & Thrall, 2001). On histopathology, some epithelial cells may contain shrunken dark nuclei surrounded by a clear halo (koilocytes) and, in papillomavirus-induced papillomas, rare cells may have basophilic intranuclear viral inclusions (Figure 18.29; Goldschmidt et al., 1998). Complete excision is typically curative, but additional lesions may appear elsewhere, especially when they are induced by papillomavirus.
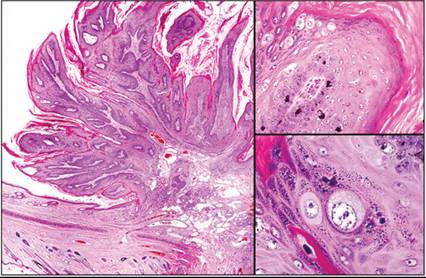
Figure 18.29 Exophytic mass on the ear pinna of a dog; papilloma. Left: the subgross appearance of the mass. Note the growth of the pattern is in an upward and inward manner typical of a viral-induced papilloma. The epidermis is markedly hyperplastic and thrown into exaggerated folds with deep rete pegs (exophytic). Upper right: there is moderate to marked anisocytosis and anisokaryosis of keratinocytes, particularly in the stratum spinosum. Lower right: scattered hypertrophic individual keratinocytes are rounded up and have an expanded pale watery to granular cytoplasm (koilocytes) (H&E: left, subgross image; upper right, 200? magnification; lower right, 400? magnification).
Mesenchymal lesions
Hemangioma/hemangiosarcoma
The vascular neoplasms hemangioma and hemangiosarcoma can be seen on the pinnae and the sparsely haired preauricular region of cats and, less frequently, dogs. These tumors are most often UV light-induced (Nikula et al., 1992). They appear as red, flattened to raised lesions. Hemangiosarcomas are more often seen in cats, while hemangiomas are more common in dogs (Sula, 2012). FNA or scrapings of vascular tumors are largely unrewarding due to their very nature. A background of hemodilution with macrophages exhibiting erythrophagia or containing hemosiderin may be seen. Plump polygonal to spindled cells may also be seen, but often diagnosis is not definitive and histopathology is required.
Hemangiomas are typified histologically by a fairly well-demarcated dermal mass of uniform plump cuboidal to spindled cells forming vascular channels that contain variable numbers of erythrocytes (Figure 18.30). Hemangiosarcomas are invasive and exhibit cellular and nuclear atypia, and cells may form solid sheets, requiring a careful search to find vascular channels. Hemangiomas are cured by complete excision. Hemangiosarcomas frequently recur, but metastasis of cutaneous lesions is not considered to occur commonly (Miller et al., 1992).
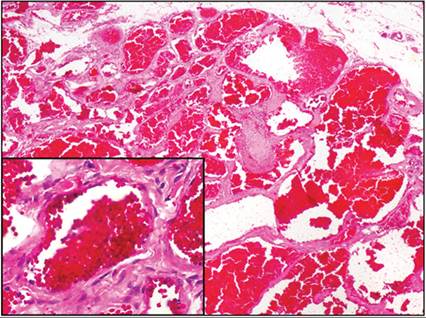
Figure 18.30 Mass at the base of the ear from a dog; hemangioma. The dermis is markedly expanded by a well-demarcated mass composed of uniform spindle cells forming blood-filled vascular channels, which are quite uniform in size. Inset: a higher-power view of a vascular channel. The spindle cells forming the stroma can be clearly seen, as can the flattened endothelial cells lining the channel. FNA would yield chiefly fresh blood and, possibly, a few uniform spindle cells (H&E: main, 40? magnification; inset, 200? magnification).
Fibrosarcoma/soft tissue sarcoma
Fibrosarcomas and soft tissue sarcomas are malignant neoplasms derived from soft connective tissues (Dennis et al., 2011). Fibrosarcomas can occur on the pinnae, particularly in cats (nonvaccine-associated; Gross et al., 2005). The lesions are firm and raised and may have indistinct margins. FNAs of fibrosarcomas are often poorly cellular. High yielding specimens, such as impression smears or scrapings of biopsies, contain a population of medium-sized to large spindled cells, which may be pleomorphic. Neoplastic fibroblasts have an ovoid to elongate nucleus, often with an open chromatin pattern, one to multiple nucleoli, and pale basophilic cytoplasm that is wispy and may be bipolar.
Although nomenclature is often in flux, currently for dogs, fibrosarcomas come under the collective term of cutaneous/subcutaneous soft tissue sarcoma (may also be called spindle cell tumor of soft tissue), along with perivascular wall tumor/hemangiopericytoma and (peripheral) nerve sheath tumor. They are termed collectively since although they may exhibit different morphological patterns chiefly appreciable on histopathology, the patterns do not always correlate with cell type of origin on a panel of immunohistochemical stains or electron microscopy. In any case, their behavior is not influenced by morphological patterns/subtypes but they are all generally predictable by the same histopathologic grading scheme, which is applicable only to dogs (Dennis et al., 2011). Aspirates of canine soft tissue sarcomas are typically high-yield. They yield clumps and individualized medium- to large-sized spindle cells which possess moderate N:C ratio with an ovoid nucleus, dense chromatin, small nucleoli, and pale to moderately basophilic wispy cytoplasm, sometimes with low numbers of fine clear vacuoles or a light dusting of pink material. Scattered binucleate and multinucleate cells may be seen, and multinucleate cells may have peripheral nuclei (‘crown cells’). Clumps are associated with a small amount of pink fibrillar matrix. On histopathology, soft tissue sarcoma is seen within the dermis as an infiltrative and poorly demarcated mass composed of interlacing bundles of often pleomorphic spindle cells forming streams and whorls (Figure 18.31). Fibrosarcomas/soft tissue sarcomas in both cats and dogs are locally aggressive so recurrence is common, especially for feline fibrosarcomas and grade II and III canine soft tissue sarcomas with close surgical margins, but they all infrequently metastasize (Hendrick et al., 1995; Dennis et al., 2011).
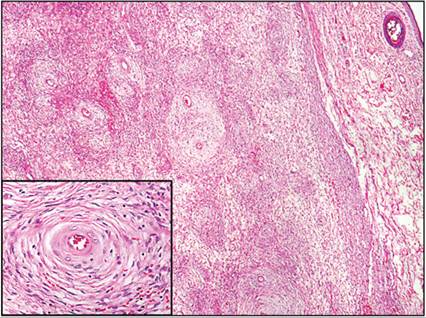
Figure 18.31 Mass on the ear pinna of a dog; soft tissue sarcoma, grade 2. The middle to deep dermis is markedly expanded by a fairly well-demarcated and nonencapsulated mass composed of streams and whorls of neoplastic mesenchymal cells. The mesenchymal cells are spindled to stellate and frequently are arranged in concentric perivascular whorls around blood vessels. Such a pattern is characteristic of perivascular wall tumors; however, immunohistochemistry is required to further distinguish the soft tissue sarcoma subtypes. In practice, the subtype does not typically influence the prognosis, as soft tissue sarcomas behave in similar ways. Inset: A high-power view of a blood vessel surrounded by concentric whirls of neoplastic spindle cells (H&E: main, 40? magnification; inset, 200? magnification).
Feline sarcoids
Feline sarcoids are masses formed by proliferating fibroblasts induced by infection with bovine papillomaviruses (Sula, 2012). They are most frequently seen in young male cats in rural areas. The pinna is a common site for these masses (Gross et al., 2005). The lesions are likely poorly exfoliative on aspiration, but scrapings may be adequately cellular. The cytology would be consistent with a mesenchymal cell proliferation, with plump spindled to polygonal cells with wispy pale basophilic cytoplasm, which may show some atypia. Histopathology of feline sarcoids typically shows an expansile and poorly demarcated mass of mesenchymal cells sometimes forming whorls. The characteristics that assist differentiation of feline sarcoid from soft tissue sarcomas are lining up of cells at the dermoepidermal junction perpendicular to the basement membrane (‘picket fence’ appearance) and involvement of the epidermis with hyperplasia and prominent rete ridges. Papillomavirus DNA may be isolated from fresh/frozen tissues with PCR (Gross et al., 2005).
Ear canal
Inflammatory lesions
Inflammatory diseases of the ear canal can develop from the external environment, via the hematogenous route, or, uncommonly, via extension from the middle ear through a ruptured tympanic membrane.
Infectious
Ear mites
The ear mite Otodectes cynotis is the cause of approximately 50% of cases of otitis externa in cats. As few as two or three mites can trigger otitis via a type I (immediate) hypersensitivity response (Weisbroth et al., 1974; Powell et al., 1980). O. cynotis can also infect dogs. Otodectic mange is variably pruritic and the consistency of the cerumen is variable. Mites may be seen grossly in the ear canal as tiny white specks that move. Swabs from infected animals yield variable numbers of mites. On cytology, O. cynotis adult mites are up to 450 μm long and 280 μm wide with a round body, a thick chitinous exoskeleton, jointed appendages with two pairs rostrally and two pairs caudally, and tapered biting mouthparts (Loshe et al., 2002). Adults, nymphs, or eggs (100 ? 210 μm) may be seen (Figure 18.32). The presence of even one mite or egg indicates infection. Examination of stained ear swab cytology is also useful to assess any secondary infections. Treatment of ear mites is by application of topical acaricides (Angus, 2004).
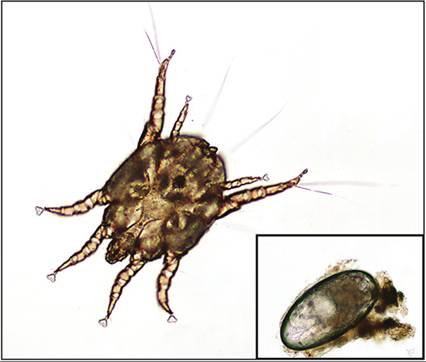
Figure 18.32 Ear swab from a cat; otodectic mange. An adult mite and egg (inset). Mites are not considered part of the normal flora of the external ear canal: even a single mite or egg warrants treatment (oil preparation: main, 100? magnification; inset, 200? magnification). (Courtesy Dr. Kelli Ferris.)
Bacterial and fungal infections
Bacterial and fungal infections of the external ear canal are almost always secondary to an underlying allergic inflammatory disease or, less commonly, a foreign body, which alters the permeability of the epidermis in the ear canal and results in a change in the otic microenvironment (Murphy, 2001). Pinnal conformation, the presence of hair within the ear canal, external temperature, and humidity have not been found to correlate with the risk for otitis externa (Grono, 1970a, 1970b; Huang & Huang, 1999; Yoshida et al., 2002; Cole, 2009).
The most common microorganisms involved in ear diseases are the cocci Staphylococcus pseudintermedius in dogs and Staphylococcus aureus and S. pseudintermedius in cats, M. pachydermatis yeasts, and Pseudomonas aeruginosa rods (Guillot & Bond, 1999; McEwan, 2000; Petersen et al., 2002; Nardoni et al., 2005). Although a variety of saprophytic fungi can be cultured from the ears of dogs and cats, pathogenic infections caused by fungi other than Malassezia are rare (Figure 18.33). Pathogenic fungal infections (otomycosis) have been reported with Candida albicans, Aspergillus spp., Sporothrix schenkii, and the dermatophyte Microsporum canis in Persian cats (Dion Speckmann, 1978; McKellar et al., 1990; Godfrey, 2000; Coyner, 2010; Ghibaudo Peano, 2010; Goodale et al., 2016). Other fungal infections including Cryptococcus spp. causing otitis interna in a cat have been rarely reported (Paulin et al., 2012).
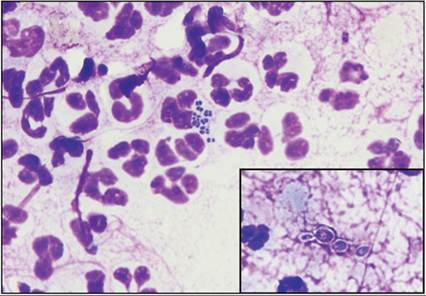
Figure 18.33 Swab from the ear of a dog; concurrent bacterial and fungal infections. The majority of the slide shows numerous degenerate neutrophils with many intra- and extracellular paired cocci bacteria. Inset: also present are rare, small, round to oval yeasts, occasionally forming chains (pseudohyphae). Although not cultured in this case, the most likely agent is Candida (modified Wright–Giemsa, 1,000? magnification). (Courtesy Dr. Frane Banovic.)
Cytology of otitis externa typically contains a background of anucleate squamous epithelial cells with associated debris. The microorganisms seen will vary but are most often cocci (Figure 18.34) and/or peanut-shaped Malassezia yeasts (in numbers above that considered ‘normal’ in the ear canal: see Table 18.1; Figure 18.35). There may also be variably degenerate neutrophils present, indicating inflammation. Bacterial rods may be seen in some cases (Figure 18.36), typically associated with more severe inflammatory responses (Figure 18.37). Rarely, Candida spp. yeasts, pseudohyphae, or hyphae may be seen or, with Aspergillus, septate, branching hyphae. Cytology will allow selection of appropriate antibiotic or antifungal medications, as well as guide the requirement for anti-inflammatory therapy (presence and numbers of neutrophils). A reproducible, semiquantitative method of evaluating ear cytology may be utilized for assessing severity of otitis externa, as well as to monitor response to treatment (Table 18.2).
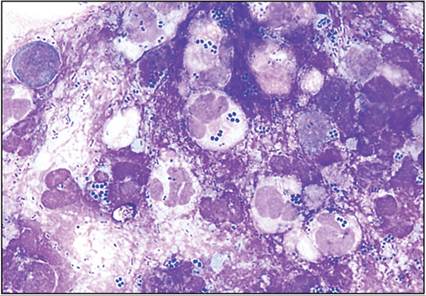
Figure 18.34 Discharge from the ear canal of a dog; suppurative inflammation with intralesional cocci bacteria. Sheets of degenerate neutrophils with myriad intra- and extracellular cocci, often in pairs, are present. This dog presented for vestibular disease. Culture of fluid from the middle ear grew Providencia stuartii (a Gram-negative bacillus) and Staphylococcus pseudintermedius (Wright–Giemsa, 1,000? magnification).
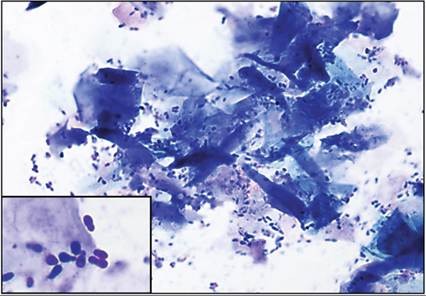
Figure 18.35 Discharge from the ear canal of a dog; yeast otitis. Clumps of angular keratinized squamous cells are present together with numerous peanut/shoeprint-shaped Malassezia spp. yeasts. Yeasts are adhered to the squamous cells and are present in the background. Inset: high-power appearance of the yeast (modified Wright–Giemsa: main, 500? magnification; inset, 1,000? magnification). (Courtesy Dr. Valarie Pallatto.)
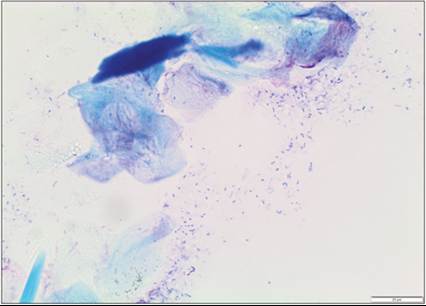
Figure 18.36 Swabfrom the ear canal of a dog; mixed bacteria. Scattered and clumps of anucleate keratinocytes with occasional melanization (bottom; black/golden granules) and mixed bacteria: cocci and bacilli (rods) (modified Wright–Giemsa: 600? magnification).
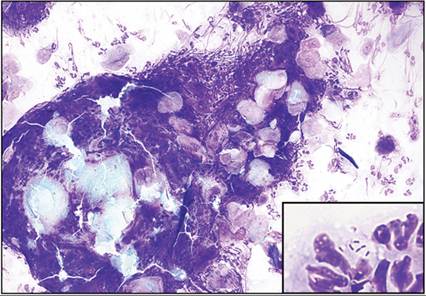
Figure 18.37 Discharge from the ear canal of a dog; suppurative inflammation with intralesional bacilli. A large clump of material composed of anucleate keratinocytes (pale to bright blue angular structures) admixed with many neutrophils is present. Inset: neutrophils are degenerate and occasionally contain bacilli (Wright–Giemsa: main, 200? magnification; inset: 1,000? magnification).
Table 18.2 Scale for use in the cytologic evaluation of otitis externa
| Scale | Description |
| 0 | No bacteria, yeast, or inflammatory cells (normal) |
| 1+ | Occasional bacteria or yeast (may be normal), or inflammatory cells seen on careful detection |
| 2+ | Bacteria, yeast, or inflammatory cells present in low numbers but detectable rapidly without difficulties |
| 3+ | Bacteria, yeast, or inflammatory cells present in larger numbers but detectable rapidly without difficulties |
| 4+ | Massive amount of bacteria, yeast, or inflammatory cells present and detectable rapidly without difficulties |
| From: Budach SC, Mueller RS (2012) Reproducibility of a semiquantitative method to assess cutaneous cytology. Vet Dermatol 23:426–480. | |
Histological assessment of otitis externa is usually only performed following total ear canal ablation. Variable numbers of anucleate squamous epithelial cells, cocci, yeasts, or rods are present in the canal. The epidermis is often moderate to markedly thickened (hyperplastic) and may have variable thickening of the stratum corneum (orthokeratotic or parakeratotic hyperkeratosis). Intercellular edema (spongiosis) or intracellular edema (ballooning degeneration) may be seen, and there are frequently moderate numbers of neutrophils traversing (exocytosing) the epidermis into the canal. There may be erosion or ulceration of the epidermis. Hair follicles may also be affected. The subjacent dermis frequently has moderate to high numbers of lymphocytes and plasma cells in a perivascular, periadnexal, or diffuse pattern (Figure 18.38). The inflammation may form discrete aggregates of lymphocytes (lymphoid follicles). There may also be hyperplasia of ceruminous glands and/or sebaceous glands (Figure 18.39).
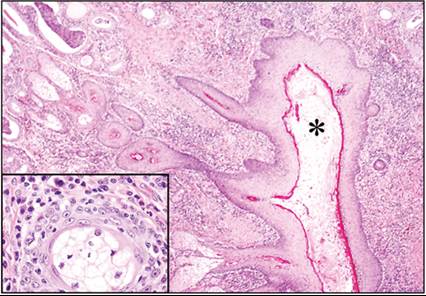
Figure 18.38 Ear canal from an American Cocker Spaniel dog; lymphoplasmacytic otitis externa. The ear canal (asterisk) is markedly stenotic and filled with cerumen and keratinous debris. The epidermis is markedly thickened. The dermal changes are characterized by a moderate to marked lymphoplasmacytic inflammatory response with ceruminous hyperplasia. The dermal collagen is abundant and dense, indicating fibrosis. Inset: an island of sebaceous cells is surrounded by lymphoplasmacytic inflammation. This dog presented for a total ear canal ablation for treatment of chronic otitis. Staphylococcus pseudintermedius and Pseudomonas aeruginosa were cultured from the ear canal (H&E: main, 40? magnification; inset: 400? magnification).
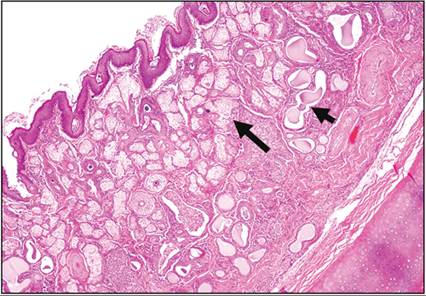
Figure 18.39 External ear canal from a dog; proliferative otitis externa. The epidermis is moderately thickened and folded with pronounced rete ridges. There is marked ceruminous (short arrow) and sebaceous (long arrow) gland hyperplasia. An accompanying mild lymphoplasmacytic inflammatory response is also present (H&E, 40? magnification).
Noninfectious lesions
Excessive cerumen may, occasionally, be the result of noninfectious causes. Overexuberant use of ear cleaners can macerate the ear canal and impair the migration of anucleate squamous epithelial cells. Ear swab cytology is composed only of squamous epithelial cells, which are predominantly anucleate. The treatment is to simply decrease the frequency of ear cleaner use (Rosychuk, 1994).
Primary secretory otitis media in the Cavalier King Charles Spaniel (Figure 18.40) can extend out into the external ear canal if the tympanic membrane is ruptured. The ear canal contains a variably colored viscous plug, which cytologically is composed of mucus (Figure 18.41), which stains Alcian blue and periodic acid-Schiff positive, and sometimes, variable numbers of neutrophils and macrophages (Weinstein et al., 2016). Rarely, yeasts, cocci, or epithelial cells are also seen in the plug material (Stern-Bertholtz et al., 2003).
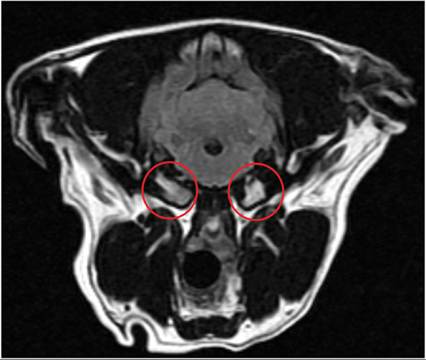
Figure 18.40 Bilateral middle ear lesions of a Cavalier King Charles Spaniel; primary secretory otitis media. MRI T2w FLAIR image showing material in both tympanic bullae (red circles). Radiologist description: the tympanic bullae are filled with T1-weighted hypointense, T2-weighted hyperintense, T2 FLAIR hyperintense, non-contrast enhancing material bilaterally with no overt increased mucosal contrast enhancement. (Courtesy Dr. Caitlin Doran and Dr. Yu Hung (Alex) Hsieh.)
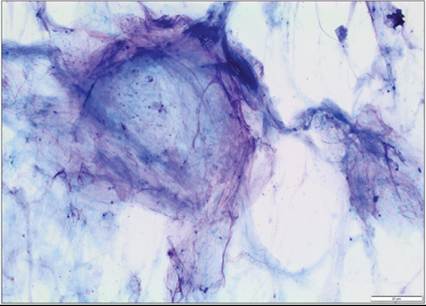
Figure 18.41 Bilateral middle ear lesions of a Cavalier King Charles Spaniel; primary secretory otitis media. Fine needle aspiration was performed of the material in the middle ear which yielded abundant mucus (modified Wright–Giemsa, 100? magnification).
Cholesterol granulomas have been rarely reported in the middle ears of dogs and cats. In these lesions, granuloma formation is secondary to the presence of cholesterol (acicular clefts) which accumulates due to cellular breakdown and lack of clearance, and acts like a foreign body. They cause disease from space-occupying lesion effects (Fliegner et al., 2007). Note that acicular clefts can form secondary to any cause of otitis media and are not diagnostic for cholesterol granuloma (Sula et al., 2014).
Proliferative, necrotizing otitis externa is an uncommon disease of young cats class="lazyload" data-src="/files/uch_group75/uch_pgroup311/uch_uch7426/image/image1042.jpg" alt=fig18.46.jpg>
Figure 18.46 Opening of the ear canal of a cat; ceruminous gland adenomas. One large and several small darkly pigmented masses are present. (Courtesy Dr. Frane Banovic.)
The cytology of ceruminous gland adenomas is dominated by cohesive clusters of small to medium-sized round to polygonal epithelial cells. Clusters are regular and may appear mosaic-like. The cells possess a low to moderate N:C ratio with a round to oval nucleus, finely clumped chromatin, and a single prominent nucleolus. The cytoplasm ranges from pale to moderately basophilic. The degree of anisocytosis and anisokaryosis is usually mild, but may be moderate when there is a secondary bacterial infection present, and may result in misdiagnosis of adenocarcinoma. In the background there may be blue to black, variably smooth to coarse granular material, which can resemble melanin but represents secretions from ceruminous ducts (Figure 18.47; De Lorenzi et al., 2005). Adenomas cannot be reliably differentiated from hyperplasia on cytology.
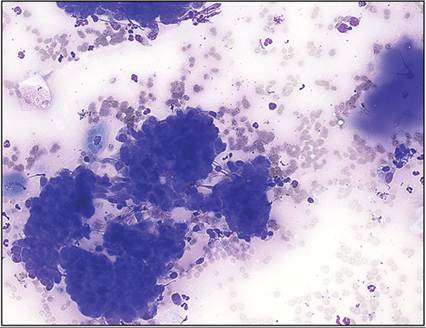
Figure 18.47 Mass in the ear canal of a dog; ceruminous gland adenoma. Clusters of deeply basophilic epithelial cells are present. Cells are uniform in appearance with round to oval nuclei and moderate amounts of deeply basophilic cytoplasm. To the right, there is a small lake of amorphous extracellular blue material consistent with ceruminous secretions. Mild suppurative inflammation is also present (Wright–Giemsa, 250? magnification).
Histopathology of ceruminous gland adenoma reveals a polypoid to papillary dermal mass that is expansile and well-demarcated. The mass is composed of uniform cuboidal to columnar epithelial cells present in tubules, papillary clusters, and acini, contained by an intact basement membrane. The individual cells have a moderate to high N:C ratio with a round to ovoid nucleus, stippled chromatin, and a single, small prominent nucleolus. The cytoplasm is pale eosinophilic. The lumens of acini contain pale basophilic to brown, finely granular material admixed with few neutrophils and nuclear and cellular debris (Figure 18.48). Mitotic figures are infrequent to rare. Variable numbers of lymphocytes, plasma cells, neutrophils, and macrophages are present in the surrounding dermis (Moisan & Watson, 1996).
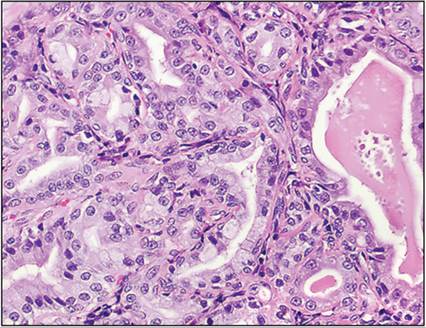
Figure 18.48 Polypoid mass in the ear canal of a cat; ceruminous adenoma. Expanding the dermis is a neoplasm composed of uniform cuboidal epithelial cells forming tubules and acini. The cells exhibit mild anisocytosis and anisokaryosis. Occasional acini contain pale eosinophilic amorphous material within the lumen (cerumen) (H&E, 300? magnification).
Ceruminous gland adenocarcinomas have multiple cellular criteria of malignancy in cytology samples including marked anisocytosis and anisokaryosis, coarse chromatin, large nuclei, macronucleoli, and binucleate and multinucleate cells (Figure 18.49). Variable numbers of neutrophils with cocci bacteria and amorphous basophilic debris (necrosis) are often observed. Blue to black extracellular material/granules may be present in the background (ductal secretions). Cell clusters may be regular and mosaic-like, as in adenomas, or nuclear molding may be present. A useful feature to assist differentiation from adenomas is the presence of acinar clusters in adenocarcinomas (De Lorenzi et al., 2005). Take care with interpretation of cellular atypia in the presence of inflammation and bacterial infection. Ceruminous gland neoplasms are frequently accompanied by otitis externa, which can complicate differentiation of adenoma from adenocarcinoma.
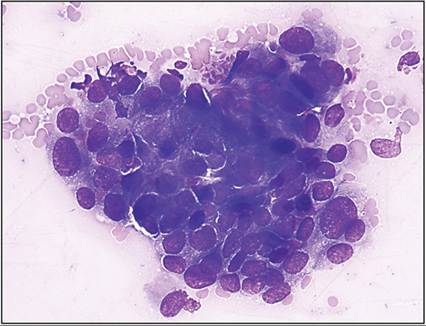
Figure 18.49 Mass in the ear canal of a dog; ceruminous gland adenocarcinoma. This tumor shows significant pleomorphism with moderate anisocytosis and anisokaryosis, cellular crowding, nuclear molding, and visible nucleoli. Biopsy confirmed a ceruminous gland adenocarcinoma (modified Wright–Giemsa, 500? magnification). (Courtesy Dr. Rebekah Gunn-Christie.)
Histologically, adenocarcinomas are exophytic to polypoid dermal masses, which are locally invasive through the dermis and subjacent stroma but do not usually invade through the auricular cartilage. Epidermal invasion may be seen. Adenocarcinomas form tubules, nests, acini, and sheets. Individual cells often exhibit loss of polarity, where the nucleus is no longer at the basolateral aspect of the acinus. Multiple cellular criteria of malignancy are typical with marked anisocytosis and anisokaryosis and frequent mitotic figures (up to 10/hpf). Areas of necrosis and mixed inflammation are usually present (Figure 18.50). Transition to squamous epithelial cells with abrupt keratinization may be seen (squamous differentiation). Tumors may occasionally be mixed, with chondroid metaplasia reported (Moisan & Watson, 1996). Surgical removal usually requires total ear canal ablation, but invasion through the tympanic membrane into the middle ear appears to be rare. The reported frequency of metastasis varies between references, with older references citing up to 50% metastasis rates and more recent references suggesting that metastasis is less common (Legendre & Krahwinkel, 1981; London et al., 1996; Moisan & Watson, 1996). Reported sites of metastasis are regional lymph nodes, lungs, and abdominal organs (Legendre & Krahwinkel, 1981). FNA of submandibular and retropharyngeal lymph nodes may be warranted as part of the clinical staging.
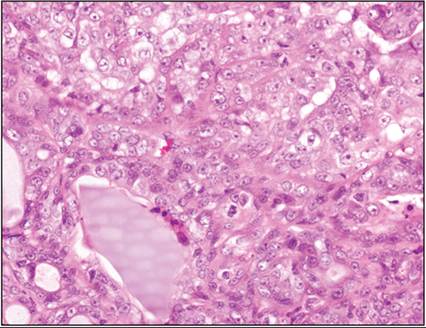
Figure 18.50 Ear canal mass from a dog; ceruminous adenocarcinoma. The dermis is infiltrated by a poorly demarcated neoplasm composed of epithelial cells forming jumbled clusters, nests, and acini. Occasional acini contain pale amphophilic material within the lumen (cerumen) (H&E, 400? magnification).
Endolymphatic sac tumor
Endolymphatic sac tumors have been rarely described in dogs. They arise from the posterior wall of the temporal bone in the inner ear, and may be found in the inner or middle ear. These tumors are locally invasive and can cause lysis of the temporal bone, but metastasis has not been reported. Histologically, they are comprised of one to two layers of well-differentiated cuboidal epithelial cells forming papillary projections on a thin fibrovascular stalk (Barnes et al., 2017). To the authors’ knowledge, cytology of these tumors has not yet been described.