Chronic Inflammatory Otitis
Nearly all of the pathologic changes that occur in ear disease are associated with alteration in form and function of one or more of these structures: cerumen, epithelium, sebaceous glands, ceruminous glands, fibroblasts, or cells of the immune system.
Without repeating a detailed analysis of the pathogenesis of otitis externa, the primary causes of disease can be summarized as chronic inflammatory diseases (atopy, adverse food reaction, parasitism), transient inflammatory diseases (parasitism, viral, contact hypersensitivity), obstructive diseases (neoplasia, foreign objects), and hyper- keratotic diseases (hypothyroidism, primary keratinization defects). Secondary bacterial and yeast infections can be associated with any of these causes, contributing to inflammation, worsened clinical signs, and perpetuation of the disease state. This section focuses on the histopathologic changes associated with chronic inflammatory diseases such as atopy and adverse food reactions.
In response to acute inflammatory stimulus, three principal changes occur: (1) dilation of blood vessels and increased vascular permeability, resulting in dermal edema; (2) alteration of epidermal barrier function; and (3) changes in cerumen composition. Grossly, edema and vascular dilation are seen as erythema and stenosis of the canal with inflamed but still pliable tissue. Loss of barrier function increases penetration of microorganism antigens and exotoxins, exacerbating local inflammation. Cerumen production tends to increase as the result of inflammation. Alterations in composition may also affect antimicrobial function, but the precise changes and effects are not well understood.29,32,38 Narrowing of the canal and occlusion with ceruminous debris provide a better environment for microorganism overgrowth. This cycle amplifies both primary inflammatory disease and secondary infection, resulting in progressive worsening of clinical otitis externa.
Early ceruminous gland dilation or hyperplasia may be seen at this stage. This can be observed grossly as dilated ceruminous glands throughout the ear canal appear slightly raised over the surrounding epidermis, contributing to what is described as a “cobblestone” appearance of the ear canal.With continued inflammation the epithelium changes from a thin layer of migrating cells to hyperplastic stratified squamous epithelium, characterized by multiple layers of cells, increased cellular turnover, and orthokeratotic hyperkeratosis.30-32 Normal epithelial migration is disrupted, resulting in greater accumulation of debris and shedding of keratin sheets directly into the lumen. If bacteria colonization or infection is a significant component of otitis, neutrophils may infiltrate the dermis, migrate through the epidermis, and form a purulent exudate in the lumen. The combination of bacterial exotoxins and neutrophil proteases can result in significant damage to the epithelium, causing erosion and ulceration. This is particularly true of infections by Pseudomonas aeruginosa.
Ongoing inflammatory stimuli from hypersensitivity to environmental allergens, dietary antigens, and bacterial or yeast products, result in hyperplasia of the three prominent cell types in the dermis: sebaceous glands, ceruminous glands, and fibroblasts. The precise mechanism for hyperplasia of these tissues is not well described but likely involves cytokines and growth factors associated with inflammation. With glandular hyperplasia there is a dramatic change in the volume of tissue occupying the limited diameter of the cartilage boundaries.28,30,32 As glandular tissue increases, the lumen of the ear canal decreases, leading to severe stenosis of the canal. Frequently, large hyperplastic folds of tissue are visible on gross and otoscopic examination; occasionally folds completely fill the canal, and no obvious opening can be found.
In one study comparing histopathologic specimens from the horizontal ear canal of dogs undergoing total ear canal ablation surgery for end-stage otitis externa, three primary tissue reaction patterns were observed: (1) predominantly sebaceous glandular hyperplasia, (2) predominantly ceruminous glandular hyperplasia, and (3) fibro- sis.33 Interestingly there is substantial variation in the predominant tissue response pattern, depending on the breed of dog affected.
Cocker Spaniels were found to have predominantly ceruminous gland response, while non-Cocker Spaniels exhibited fibrosis most often. Less commonly observed tissue reactions included lichenoid interface dermatitis, eosinophilic infiltration, and ulcerative otitis.A separate study reported similar findings. The area covered by sebaceous glands was not significantly different in a comparison of spaniel dogs with or without otitis externa.32 However, the area covered by ceruminous glands was markedly increased with otitis externa. Increases in glandular tissue occurred by both hyperplasia and marked dilation of the central lumens (ectasia). Grossly, this may be seen as hyperplastic folds with a cobblestone surface or in some cases dilated purple, blue, or clear cystic structures.
Hyperplasia and dilation of ceruminous glands is frequently accompanied by inflammation, resulting in ceruminous gland adenitis (Figure 3-10). The resultant destruction of glandular epithelium and leakage of glandular contents into the interstitial space results in large amounts of lipid. Macrophages filled with lipofuscin, a wear-and-tear pigment associated with oxidative stress, were observed around inflamed ceruminous glands (Figure 3-11). The presence of lipofuscin-laden macrophages is positively correlated with breed, ceruminous gland tissue response
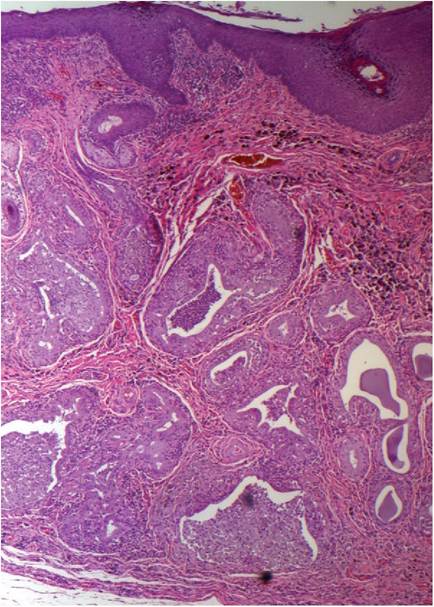
Figure 3-10
Severe ceruminous gland hyperplasia, ectasia, and inflammation. Large numbers of neutrophils are present both around the glands, in the gland walls, and in the dilated gland lumens. Note the tremendous thickening of the epithelial layer from one to two cells thick to 20 to 30 cells thick.
pattern, and osseous metaplasia (unpublished data). Lipofuscin cannot be broken down by the body; as a result, the large amounts of lipofuscin-laden macrophages may create a chronic granulomatous inflammation that cannot be resolved.
Continued cytokine and growth factor production from these macrophages may contribute to perpetuation of glandular hyperplasia, fibrosis, osseous metaplasia and other changes observed in end-stage otitis externa.In addition to macrophages, ear canal tissue may be infiltrated with large numbers of neutrophils, T-lymphocytes, and plasma cells. With chronicity, lymphoid nodules may develop in the deep dermis.
One of the most clinically significant histopathologic changes associated with chronic inflammatory otitis is calcification. A common misconception of this process is that the cartilage tube transforms to calcified tissue. In fact, the majority of calcification occurs in the soft tissue outside the cartilage boundaries (Figure 3-12). The process is true osseous metaplasia, where the resident fibroblasts transform to
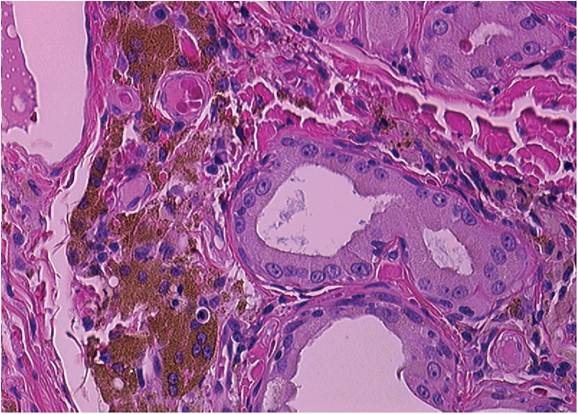
Figure 3-11
Photomicrograph of lipofuscin-laden macrophages. Lipofuscin is the yellow-brown granular pigment in the tissue adjacent to the ceruminous gland.
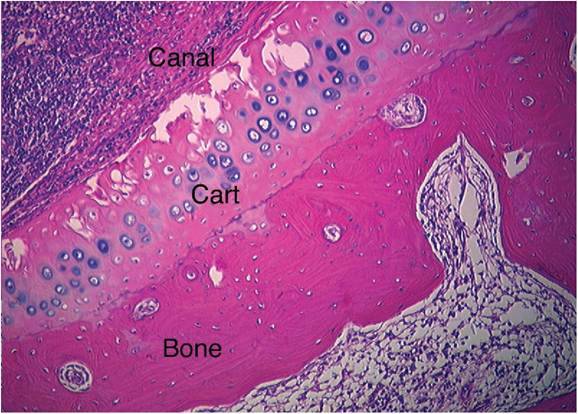
Figure 3-12
Osseous metaplasia. Figure shows a cross-section of vertical ear canal from a dog with end-stage otitis externa. The ear canal tissue is filled with large numbers of white blood cells. The cartilage border separates the ear canal tissue from the new bone being formed outside of the ear canal.
produce bonelike tissues in an inappropriate location. Palpation of the para-aural space reveals rigid calcification, usually surrounding the dorsal, lateral, and ventral canal in a semicircular formation. The new bone is easily visible on computed tomography (CT) scans or radiographs of the skull (Figure 3-13). This change is irreversible and represents progression toward an end-stage canal, which is less likely to respond to medical therapy.
Progression from edema to epidermal hyperplasia, glandular hyperplasia and ectasia, deposition of lipofuscin, lymphoid nodules, fibrosis, and osseous metaplasia represents a spectrum of histopathologic changes associated with otitis externa. Understanding these changes and the mechanisms driving them can assist in diagnosis, prognosis, and appropriate therapeutic decision making in the management of chronic inflammatory otitis.
Cocker Spaniels
In a review of 80 dogs undergoing total ear canal ablation for end-stage inflammatory otitis externa, 48 of the dogs were Cocker Spaniels (60%).33 Over the same time period, Cocker Spaniels represented only 4.2% of the general hospital population. The next most commonly represented breeds were six mixed-breed dogs (7.5%). No other pure breed was represented by more than two dogs (2.5%). Cocker Spaniels do not have a higher incidence of atopy, food allergy, or ear mites, which would have
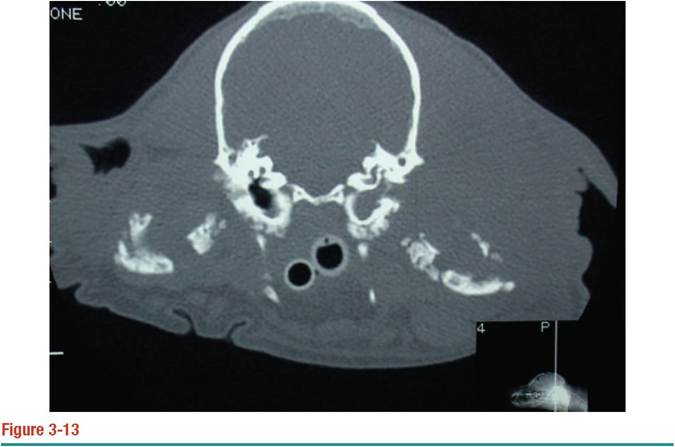
CT scan of a Cocker Spaniel with osseous metaplasia. The skull is visible centrally. Both tympanic bullae can be seen. Contrast the air-filled bulla on the left with the fluid-filled bulla on the right. Bone lining the bulla is thickened and irregular. New bone is visible in the soft tissue on both sides of the skull.
explained the 24-fold increase in incidence of end-stage otitis over the next most represented pure breed or a 14-fold increase over the incidence predicted by breed popularity. The most likely explanation for the observed overrepresentation is that Cocker Spaniels have a different pathologic response to primary conditions causing otitis externa. This hypothesis was supported by substantial differences in histopathologic findings from the horizontal ear canal. Most notably, 72.9% of Cocker Spaniels had changes dominated by ceruminous gland hyperplasia and ectasia (Figures 3-14 and 3-15). By comparison, only 28.1% of all other breeds demonstrated this tissue response pattern. The most common pattern observed in other breeds was fibrosis, seen in 40.6% of other breeds and 8.3% of Cocker Spaniels (Figure 3-16).33
Cocker Spaniels were also found to have a higher incidence of lipofuscinladen macrophages infiltrating the tissue than other breeds of dogs; this feature was observed in 70.8% of the Cocker Spaniels, compared with 25% of other breeds.
Osseous metaplasia in the soft tissue surrounding the horizontal canal was observed in 60.4% of the Cocker Spaniels but only 21.9% of non-Cocker Spaniel breeds.33Overall, these differences in histopathologic changes in end-stage otitis externa suggest that American Cocker Spaniels have different physiologic responses to inflammatory stimuli. The differences in tissue response result in more severe expression of disease, confirming previous observations that Cocker Spaniels have more frequent and more severe otitis externa than other breeds.
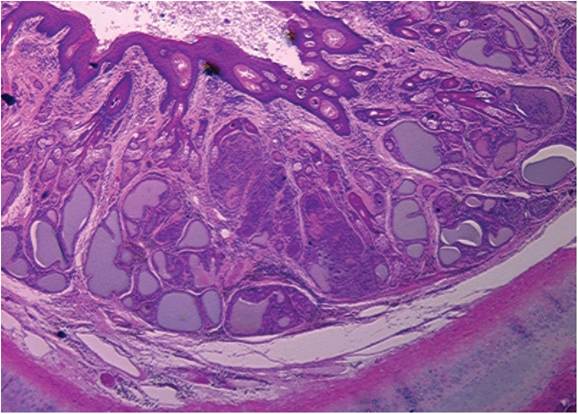
Figure 3-14
Cocker Spaniel with ceruminous gland tissue response, characterized by hyperplasia of ceruminous glands, dilation of glands, and inflammation.
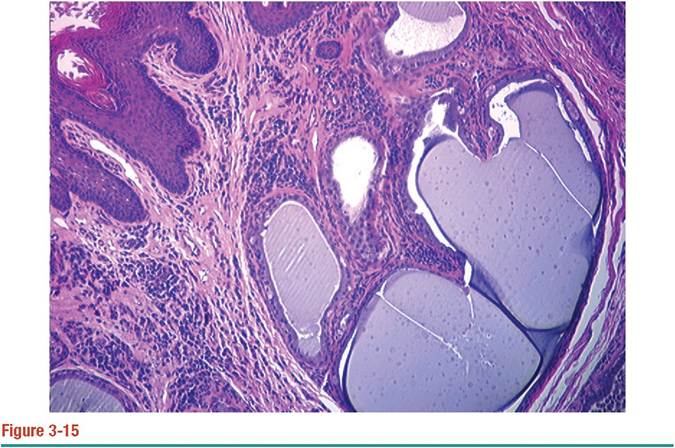
Close-up of single-hair follicular unit from same dog as in Figure 3-14.
Neoplasia
In general the ear canal is an uncommon site for tumor development. The true incidence of ear canal tumors in dogs and cats is not known, but based on surveys of total submissions to pathology laboratories, less than 1% of all tumors in dogs and less than 2% of all tumors in cats occur in the ear canal.39 Tumors can arise from epithelium, ceruminous glands, sebaceous glands, fibroblasts, mast cells, and virtually any other cell type found in the lining of the external canal.
Any nodule, mass, or polyp found in the ear canal should be biopsied for histopathologic diagnosis. Biopsy of nodules deep in the canal can be difficult due to the limited confines of the canal and diminished visualization due to debris. Care should be taken not to crush the tissue with hemostats, alligator forceps, or other blunt, grasping instruments. A diagnostic sample can best be obtained using biopsy forceps (Figure 3-17). If available, video-otoscopic guided CO2 laser can be a practical alternative to grasping and pulling.
Because neoplasia can occur due to transformation of chronically inflamed tissue, histopathology should also be obtained of any tissue removed during lateral ear canal resection or total ear canal ablation, even if the patient has a history of longstanding disease. Do not section the ear canal prior to submission; the entire canal should be submitted in situ, so that the pathology laboratory personnel can trim ear canals using a standard method.
The most common tumors of the ear canal in both cats and dogs are ceruminous gland adenoma and adenocarcinoma. Contrary to early reports indicating that tumors
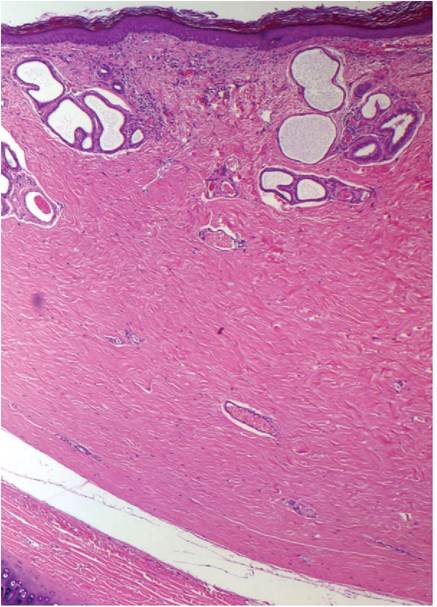
Figure 3-16
Example of fibrosis tissue response pattern. Note the absence of inflammation and sparse follicular units in the deep dermis, which is replaced by large amounts of collagen tissue.
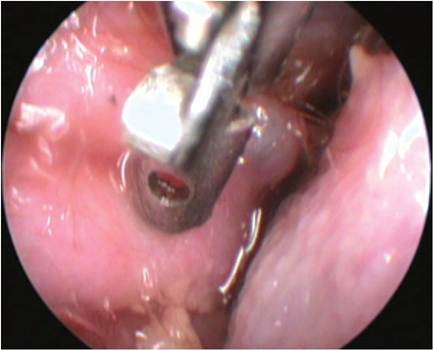
Figure 3-17
Video-endoscopic biopsy forceps obtaining sample from nodule in the vertical canal.
of ceruminous gland origin were more frequently benign in dogs and malignant in cats, this distinction may not be entirely accurate or reliable. In a large review of 124 ceruminous tumors, 61% of dogs and 69% of cats had adenocarcinoma.39 The frequency of malignancy is high enough that any tumor of the ear canal should be treated suspiciously until proven otherwise by histopathologic diagnosis.
Typical histopathologic findings of adenoma are well-differentiated proliferation of polypoid cuboidal-to-columnar epithelium. The neoplastic tissue forms acini and secretory ducts. Mitotic figures are rare. Individually cells have minimal atypia, ovoid- to-round nuclei, and a single prominent nucleolus. Glands tend to retain normal myoepithelial basement membrane boundaries and do not invade connective tissue parenchyma.39
In contrast, adenocarcinoma is characterized by moderate or marked nuclear atypia and common mitotic figures. Neoplastic tissue fails to form normal-appearing secretory gland patterns. Orientation of the apical surface to the myoepithelial basement membrane is absent. Squamous differentiation, characterized by individual necrotic keratinocytes, dyskeratosis, and keratin pearl formation, can be seen. As tumors outgrow effective blood supply, central necrosis can be observed. Most significantly, adenocarcinoma frequently invades connective tissue parenchyma, occasionally penetrating the auricular or annular cartilage.39
Other tumors diagnosed by histopathology include squamous cell carcinoma, mast cell tumor, malignant melanoma, hemangiosarcoma, fibrosarcoma, lymphoma, and basal cell carcinoma.
Nasopharyngeal polyps are a common tumorlike disease in cats. Polyps are fleshy, nodular masses of fibrous connective tissue that develop from respiratory epithelial tissue of the nasopharynx, eustachian tube, or tympanic cavity. Some patients present with respiratory signs such as nasal discharge, sneezing, and stertor or with dysphagia and recurrent gagging. If the polyp fills the tympanic cavity, it may rupture the tympanic membrane and protrude into the external canal, resulting in obstructive otitis. Biopsy should be taken to rule out neoplasia. Histopathologically, polyps are characterized by an irregular mass of fibrous connective tissue covered by a layer of respiratory epithelium. The pathognomonic finding is respiratory cilia on the surface of the mass. Less commonly, dogs can also develop benign fibrous polyps arising from the external ear canal, tympanic membrane, or respiratory epithelium.
Cocker Spaniels
Not only are Cocker Spaniels more likely to have more severe histopathologic changes associated with chronic inflammation, but American Cocker Spaniels are also overrepresented in studies of ear canal tumors.31,40 In a large review of 81 dogs with ear canal tumors, Cocker Spaniels were found to represent 17% of all cases of malignant tumors, and 27% of the benign tumors.41 In the same review, 35% of dogs with malignant neoplasia had a prior history of chronic otitis. This finding is not surprising, since chronic inflammation and ceruminous gland hyperplasia are suspected risk factors for neoplastic transformation.42